Effect of aromatic stimulation on CPAP adherence and sleep quality in patients with obstructive sleep apnea: a pilot study
Erina Ishimizu, Ayako Inoshita, Yo Suzuki, Masahiro Nakamura, Takatoshi Kasai, Fumihiko Matsumoto

TL;DR
This pilot study explores whether using lavender or cypress aromas can improve CPAP adherence and sleep quality in patients with obstructive sleep apnea.
Contribution
The study introduces aromatic stimulation as a novel, noninvasive method to enhance CPAP adherence and sleep outcomes in OSA patients.
Findings
Median PSQI scores improved significantly after 67 days of aromatic stimulation.
CPAP usage duration increased from 149 to 231 minutes per night following the intervention.
Exposure to essential oils was associated with improved adherence and subjective sleep quality.
Abstract
Continuous positive airway pressure (CPAP) therapy remains the cornerstone of obstructive sleep apnea (OSA) treatment, considerably reducing the risk of cardiovascular complications and improving patient outcomes. However, adherence to CPAP therapy is a major challenge and poor compliance limits its efficacy. This study investigated the potential of aromatherapy, a noninvasive, cost-effective intervention, to improve CPAP adherence and enhance sleep quality in patients with OSA. A prospective observational pilot study was conducted in patients with obstructive sleep apnea who demonstrated poor CPAP adherence (< 70% usage and < 4 h/night). Participants were exposed to lavender or cypress aroma oil during sleep. Pre- and post-intervention subjective sleep measures Pittsburgh Sleep Quality Index (PSQI) and Epworth Sleepiness Scale (ESS), and objective CPAP usage metrics were collected.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
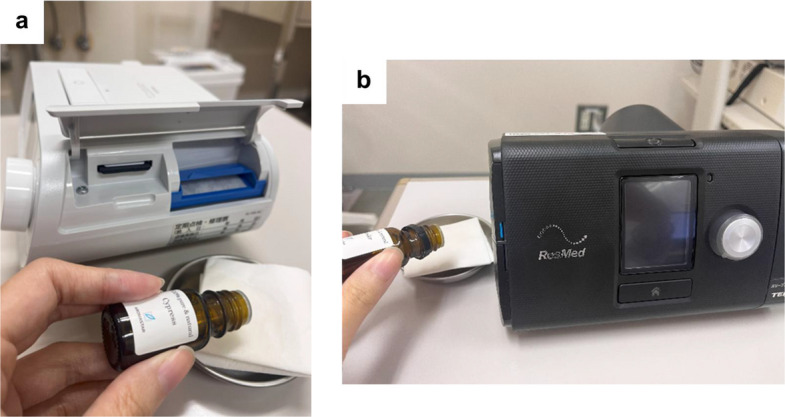 Figure 1
Figure 1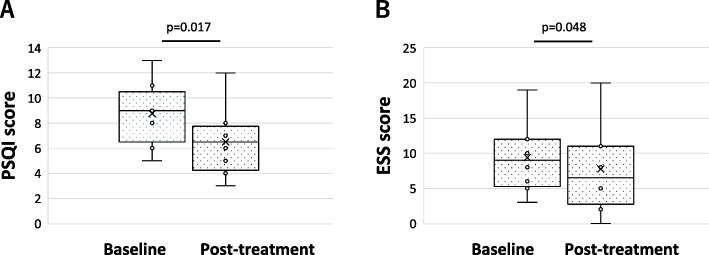 Figure 2
Figure 2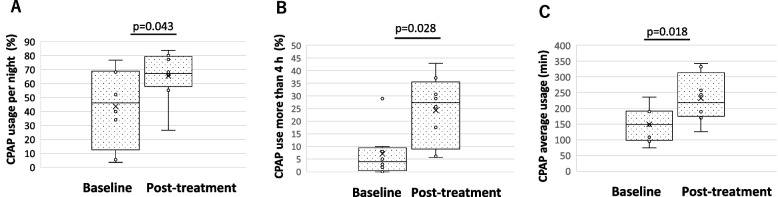 Figure 3
Figure 3- —https://doi.org/10.13039/501100001691Japan Society for the Promotion of Science
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsObstructive Sleep Apnea Research · Olfactory and Sensory Function Studies · Sleep and related disorders
Introduction
Obstructive sleep apnea (OSA) is a common condition associated with significant morbidity and mortality, including excessive daytime sleepiness, automobile accidents, and cardiovascular complications such as hypertension and arrhythmias [1–3]. Continuous positive airway pressure (CPAP) therapy improves psychological and physical impairments in patients with OSA with sleepiness, fatigue, neurocognitive impairment, and depression. Moreover, it can prevent hypertension, adverse cardiovascular events, and arrythmia [1, 4]. CPAP is gold standard treatment for patients with moderate to severe OSA [5, 6].
However, the effectiveness of CPAP therapy is strongly dependent on treatment adherence. Optimal therapeutic benefit requires at least 4 h of nightly use on > 70% of nights, yet adherence rates remain suboptimal, ranging from 30 to 60% worldwide [7, 8]. Poor CPAP adherence is a major clinical challenge, leading to persistent symptoms, increased healthcare utilization, and higher risk of cardiovascular events. Common barriers include mask discomfort, nasal symptoms, dryness, pressure intolerance, and psychological resistance to device use [9]. Although interventions such as mask fitting optimization, humidification, nasal therapy, and behavioral support are routinely implemented, a considerable proportion of patients continue to struggle with CPAP acceptance and adherence [10]. Thus, alternative or adjunct strategies to improve tolerance and long-term adherence are urgently needed.
Alternative or adjunctive treatments for OSA include oral appliances, uvulopalatopharyngoplasty (UPPP) and upper airway surgeries [11], and hypoglossal nerve stimulation (HGNS) has emerged as an option for CPAP-intolerant patients [12]. Nevertheless, surgical approaches are invasive and limited to selected candidates [13], highlighting the need for non-invasive, patient-friendly methods to support CPAP use.
Recently, medical aromatherapy has been used to examine the impact of essential oil scents, such as lavender, cypress, and rose, on psychological and physiological states, garnering particular interest in their potential to enhance sleep quality [14, 15]. In clinical practice, aromatherapy has been introduced in various clinical settings, including palliative care, intensive care units, and bathing methods [16, 17]. However, despite these findings, little is known about whether aromatherapy can specifically support CPAP adaptation and adherence in patients with OSA, and no standardized approach currently exists for integrating aromatherapy into CPAP use. Given these considerations, this pilot study aimed to investigate whether aromatic stimulation could improve CPAP tolerability, enhance adherence, and improve subjective sleep quality in patients with OSA who exhibit difficulty with CPAP therapy.
Materials and methods
Patients
This prospective observational pilot study included eight CPAP-intolerant patients with OSA who had received CPAP treatment at the Sleep-Disordered Breathing Center of Juntendo University Hospital between March 8, 2019 and February 10, 2020. Patients were intentionally selected using a purposive sampling method according to the following inclusion criteria: a confirmed diagnosis of OSA; CPAP use for at least three months with an average nightly usage of less than 4 h; no nasal or mask-related problems; and absence of other sleep disorders.
Nasal endoscopy was performed in all patients to confirm the absence of nasal polyps, hypertrophic rhinitis, and olfactory fissure occlusion. The presence of olfactory disturbances was confirmed through interviews. The CPAP equipment used was Sleep mate®10 (ResMed, San Diego, USA) or Dream Station® (Philips Respironics, Amsterdam, NLD). The exclusion criteria were as follows: (1) age < 20 years, (2) nasal diseases with olfactory dysfunction, (3) a history of allergy to lavender or cypress oil, (4) no smell of aroma oil, (5) pregnancy, and (6) neuromuscular disease. This study was approved by the Ethics Committee of the Juntendo University Faculty of Medicine (E18-213) and conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines. Written informed consent was obtained from all participants.
Aromatherapy
The patients were provided with specific instructions to place a tissue or cotton ball infused with one–three drops of aroma oil adjacent to their CPAP apparatus before commencing their nightly sleep regimen. The quantity of aroma oil applied was tailored to individual smell intensity preferences. Two distinct types of essential oil, lavender and cypress (100% pure&nature lavender® and 100% pure&nature cypress® AROMASTAR, Nagoya, JPN) were applied based on previous reports on their effects on good sleep [16, 18]. The methodology for administering these aroma oils was comprehensively elucidated during outpatient consultations with practical demonstrations utilizing the actual aroma oil (Fig. 1). Patients confirmed aroma use on CPAP nights via a daily diary, which was used to monitor compliance.Fig. 1. The actual setting of aroma oil. Aroma oils on a tissue of cotton were placed nearby CPAP filter. A Sleep mate®10, B Dream Station®
Outcomes
For evaluation purposes, two established tools, the Epworth Sleepiness Scale (ESS) and the Pittsburgh Sleep Quality Index (PSQI), were administered both before and after the aroma oil trial [16–19]. Excessive daytime sleepiness was measured using the ESS, with scores of 11 or higher indicating excessive daytime sleepiness. To measure subjective sleep quality, a widely used self-administered questionnaire, the PSQI, was completed in the previous month. To assess the effect on sleep onset, we compared the sleep onset latency before and after using the oil. Sleep-onset latency was measured by self-reporting using the PSQI. Post-intervention assessments of ESS and PSQI were obtained approximately two months after initiation of the aromatherapy intervention.
The downloaded CPAP data were compared before the use of the aroma oil and the last two months of the trial. The following CPAP parameters were evaluated: (1) percentage of days with CPAP usage (%), (2) percentage of days with CPAP usage > 4 h (%), (3) average usage per night (min), and (4) average apnea–hypopnea index (AHI) on CPAP (events/h). CPAP usage metrics were likewise evaluated over the final two months of the aromatherapy period. No additional interventions, such as therapeutic education, phone calls, proactive follow-up, or telemonitoring, were provided.
Statistical analyses
No statistical sample size calculation was conducted, as this was an exploratory pilot study.
A post hoc power analysis was performed using the observed effect sizes for the main outcomes (PSQI, ESS, and CPAP adherence). However, post hoc power analyses indicated that the study had 91%, 66%, and 98% power to detect the observed differences in PSQI, and ESS, and CPAP usage (> 4 h), respectively.
Each score in the survey items was compared using the t-test for normally distributed continuous variables and the Wilcoxon signed-rank test for non-normally distributed continuous variables. A value of p < 0.05 was considered to be statistically significant. All values are shown as the median interquartile range.
Results
Among 388 patients undergoing CPAP therapy, 8 met the inclusion criteria and were enrolled in this study. The median age was 53.5 years [50.3–71], and four of the eight were male (Table 1). The median duration of CPAP use with aroma usage was 67 days [46–116]. Patients applied the aroma oil on the nights they used CPAP and documented its use in a daily diary for compliance monitoring. The results are summarized in Table 2.Table 1. Patient characteristicsVariableValueAge, years58.4 ± 11.3, 53.5 [50.3–71]Sex Male, n (%)4 (50.0) Female, n (%)4 (50.0)Complications Hypertension, n (%)3 (37.5) Diabetes, n (%)1 (12.5) Heart failure, n (%)2 (25.0) Respiratory disease, n (%)0 (0.0)AHI at OSA diagnosis (events/hour)43.1 ± 13.2, 46.8 [33.4–50.5]Duration of CPAP use (month)26.6 ± 32.4, 10 [8.5–34]PSQI score8.8 ± 2.5, 9 [7.5–9.5]ESS score9.4 ± 5.0, 9 [5.8–12]Data are presented as mean ± SD, median [IQR], or n (%)AHI apnea hypopnea index, OSA obstructive sleep apnea, CPAP continuous positive airway pressureTable 2PSQI,ESS, and CPAP use before and after using aroma oilVariableBaselinePost-treatmentp-valuePSQI score9.0 [7.5–9.5]6.5 [4.8–7.3]0.006 *ESS score9.0 [5.8–12]6.5 [4.3–11]0.034 *Sleep onset latency (minutes)15 [9–23]9 [5–10]0.390Download date from CPAP Percent days with CPAP usage (%)43.6[26.9–68.3]66.1 [63.2–77.8]0.043 * Percent of days with CPAP usage > 4 h (%)5.0 [1.4–8.5]25.7 [14.7–32.2]0.028 * Average usage (min)149 [105–191]231 [184–276]0.018 * Average AHI on CPAP (events/h)3.2 [1.8–4.2]1.3 [1.0–3.0]0.226Data are presented as median [IQR]PSQI Pittsburgh Sleep Quality, ESS Epworth Sleepiness Scale, CPAP continuous positive airway pressure, AHI apnea hypopnea index
The PSQI for sleep quality significantly decreased from 9 [7.5–9.5] to 6.5[4.8–7.3] (p = 0.006) (Fig. 2A). The ESS, which was for subjective symptoms of daytime drowsiness significantly decreased from 9 [5.8–12] to 6.5 [4.3–11] after oil use (p = 0.034) (Fig. 2B).Fig. 2. Changes before and after treatment with aroma oils in questionnaires. A PSQI score showed significant improvement after the aroma therapy from 9.0 [7.5–9.5] to 6.5 [4.8–7.3 (p = 0.006). B ESS score showed significant improvement after the aroma therapy from 9.0[5.8–12] to 6.5[4.3–11 (p = 0.034)
As for CPAP, the usage rate increased from 43.6% [26.9–68.3] to 66.1% [63.2–77.8] (p = 0.043) (Fig. 3A), the percentage of days used for more than 4 h from 5.0% [1.4–8.5] to 25.7% [14.7–32.2] (p = 0.028) (Fig. 3B), and the average duration of use from 149 min [105–201] to 231 min [184–276] (p = 0.018) (Fig. 3C), showing significant improvement in all parameters. No significant differences were observed in AHI under CPAP use from 3.2 events/h [1.8–4.0] to 1.3 events/h [1.0–3.0] (p = 0.226) and sleep onset latency from 15 min [9–23] to 9 min [5–10] (p = 0.390). None of the patients had unpleasant feelings with the smell of aroma oil or nasal symptoms such as nasal obstruction.Fig. 3. Changes before and after treatment with aroma oils in CPAP data. A CPAP usage per night showed significant improvement after the aroma therapy from 43.6 [26.9–68.3] % to 66.1 [63.2–77.8] % (p = 0.043). B CPAP usage per night more than 4 h showed significant improvement after the aroma therapy from 5.0 [1.4–8.5] % to 25.7 [14.7–32.2] % (p = 0.028). C CPAP average usage time showed significant improvement after the aroma therapy from 149 [105–191] minutes to 231 [184–276] minutes (p = 0.018)
Discussion
In this pilot study, we investigated whether aromatic stimulation could improve the tolerability of CPAP in patients with OSA. Several notable findings emerged. First, both ESS and PSQI scores improved after exposure to aroma oils, suggesting enhanced subjective sleep quality. Additionally, total CPAP usage, the proportion of nights with > 4 h of use, and average CPAP usage duration all increased. These results indicate that aromatic stimulation may have a positive influence on CPAP adherence. Importantly, improvements in subjective sleep quality and increased CPAP usage were observed in parallel, suggesting a potential bidirectional interaction whereby more restorative sleep may facilitate mask tolerance, while increased CPAP use may further enhance sleep quality.
Although CPAP is the first-line therapy for moderate to severe OSA, mask intolerance can limit its effectiveness [20]. Alternative therapies such as OA confer certain cardiovascular benefits but may cause side effects such as jaw discomfort [21–23]. Surgical options, including uvulopalatopharyngoplasty (UPPP) and HGNS, may improve AHI but are only suitable only for selected patients and carry risks of complications [24–28]. Therefore, developing effective noninvasive strategies to enhance CPAP adherence remains clinically important. Importantly, improvements in subjective sleep quality and increased CPAP usage were observed in parallel, suggesting a potential bidirectional interaction whereby more restorative sleep may facilitate mask tolerance, while increased CPAP use may further enhance sleep quality.
This study indicated that the effects of aromatic stimulation may have positively influenced sleep centers. The olfactory system plays a pivotal role in the mediation of the effects of aromatherapy. Odor molecules are transmitted from the olfactory epithelial mucosa in the nasal passages to the olfactory bulb, where they initiate a cascade of signals that traverse various brain regions, including the anterior piriform cortex, anterior olfactory nucleus, amygdala, hypothalamus, and entorhinal cortex. From the piriform cortex, these signals are relayed to the frontal olfactory cortex of the cerebral cortex, where they are cognitively processed as distinct odors. Notably, the amygdala and hypothalamus govern emotions, whereas the hippocampus is associated with memory [29]. In addition, because the hypothalamus contains sleep and autonomic nervous centers, odor stimuli may affect sleep quality and autonomic nervous system activity [29]. The results of this study suggest that the transmission of lavender and cypress oil, which are considered to have good odors, through these pathways stimulates sleep and autonomic nerve centers, resulting in deep sleep, which may be involved in improving CPAP adherence and sleep quality. Odor stimulation may also increase the parasympathetic nervous system activity, which may reduce the physical and emotional stress caused by CPAP use. Okabe et al. examined healthy subjects immediately after rose odor stimulation during REM sleep and asked them about their dreams; many responded that they had bad dreams [14]. However, in our results, although dreams were not included in the survey items and olfactory elements were not the same components, the PSQI results indicated that olfactory stimulation improved sleep quality. Furthermore, pleasant odors induce a deep "sniffing response" during sleep, and even the anticipation of being presented with pleasant odors can induce a sniffing response [30]. The present study demonstrated an improvement in CPAP adherence, suggesting that the aroma oil load during sleep, which is perceived as pleasant, may have facilitated and stabilized breathing.
The results of this study suggest a new perspective that low-cost olfactory stimulation is potentially effective for improving sleep quality in CPAP-intolerant patients.
Previous studies have reported a high prevalence of olfactory dysfunction in patients with OSA, correlating with disease severity [31, 32], potentially due to nasal obstruction, impaired mucociliary clearance, or neuronal injury from intermittent hypoxia [33]. CPAP therapy may improve olfactory function by restoring nasal airflow, reducing inflammation, and mitigating hypoxia-related neuronal damage [31, 32]. Although our participants did not report olfactory dysfunction, these findings support the rationale that olfactory stimulation may complement CPAP therapy by engaging neural pathways involved in sleep regulation and adherence.
Pearl et al. demonstrated that respiration-triggered olfactory stimulation could reduce OSA severity, as measured by AHI and oxygen desaturation indices [33]. In contrast, our study applied continuous exposure to pleasant aroma oils during sleep. Despite differences in stimulation method, both studies support the notion that olfactory input can positively influence sleep and respiratory parameters. In our study, improvements in PSQI and ESS scores were accompanied by increases in total CPAP usage, proportion of nights with > 4 h of use, and average nightly usage duration, suggesting that continuous aromatic stimulation may enhance sleep quality and facilitate adherence to CPAP therapy. Previous studies examined olfactory function in patients with OSA, showing a higher prevalence of olfactory dysfunction compared to healthy controls and correlations with AHI [34, 35]. Causes may include nasal obstruction, impaired mucociliary clearance from chronic upper airway inflammation, or neuronal damage due to intermittent hypoxia [36]. The results of this study suggest a new perspective that low-cost olfactory stimulation is potentially effective for improving sleep quality in CPAP-intolerant patients.
This study has several limitations. Sleep electroencephalography recordings were not incorporated into our study protocol, thereby precluding the opportunity for an objective assessment of sleep patterns and characteristics. The sample size was small, and no a priori sample size calculations were performed, and no control group was included. Baseline olfactory function was not formally tested, and the amount of aroma oil used was not standardized. Nevertheless, we cannot exclude the possibility that the use of aroma oils itself enhanced patients’ motivation or awareness toward CPAP therapy, indirectly contributing to better adherence. As a pilot study, further research is needed, but our findings suggest that low-cost olfactory stimulation may represent a promising adjunctive approach to enhance sleep quality and CPAP adherence in patients with poor compliance.
Conclusion
Aroma oil appears to have the potential to enhance sleep quality, improve daytime sleepiness, and promote greater adherence to CPAP therapy in patients with OSA who experience difficulty with CPAP treatment. A plausible mechanism underlying these effects is the impact of olfactory stimulation on sleep and autonomic regulatory centers, particularly those mediated through the hypothalamus. These findings represent a promising step towards addressing adherence changes in patients with CPAP intolerance. Non-invasive, inexpensive, easily applicable, and cost-effective aromatic stimulation could be beneficial for these patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Newman AB, Javier Nieto F, Guidry U, Lind BK, Redline S, T G Pickering TG, et al. Relation of Sleep-disordered Breathing to Cardiovascular Disease Risk Factors. Am J Epidemiol. 2001;154:1–12.10.1093/aje/154.1.5011434366 · doi ↗ · pubmed ↗
- 2Wozniak DR, Lasserson TJ, Smith I. Educational, supportive and behavioural interventions to improve usage of continuous positive airway pressure machines in adults with obstructive sleep apnoea. Cochrane Database Syst. 2014;1:CD 007736. 10.1002/14651858.CD 007736.pub 2. 10.1002/14651858.CD 007736.pub 224399660 · doi ↗ · pubmed ↗
- 3Knötzele J, Riemann D, Frase L, Bernd Feige, Elst LT, Kornmeier J. Presenting rose odor during learning, sleep and retrieval helps to improve memory consolidation: a real-life study. Sci Rep. 2023;13:2371.10.1038/s 41598-023-28676-z PMC 991172236759589 · doi ↗ · pubmed ↗