Suture Bridge Fixation for Ulnar Sublime Tubercle Avulsion Fractures in High School Baseball Players: A Report of Two Cases
Takahiro Kaga, Kenichi Otoshi, Kinshi Kato, Hironori Numazaki, Yoshihiro Matsumoto

TL;DR
This paper presents two cases where high school baseball pitchers were successfully treated for rare elbow fractures using a suture bridge fixation technique.
Contribution
The study introduces suture bridge fixation as a viable surgical option for small avulsion fractures in adolescent athletes.
Findings
Suture bridge fixation achieved anatomical reduction and radiographic bone union in both cases.
Both athletes returned to full competitive pitching without symptom recurrence.
The technique is suitable when fragment size limits screw fixation.
Abstract
Ulnar sublime tubercle avulsion fractures caused by repetitive valgus stress are rare injuries predominantly observed in adolescent overhead throwing athletes. Although conservative management is typically the first-line treatment, surgical intervention may be required in cases of nonunion, displaced fragments, or persistent medial elbow pain. We report two high school baseball pitchers with symptomatic ulnar sublime tubercle avulsion fractures that were unresponsive to conservative treatment and were surgically treated using a suture bridge fixation technique. In both cases, the small, avulsed fragment was secured with a proximally placed suture anchor, and the suture limbs were tensioned laterally and fixed distally using a knotless anchor to achieve anatomical reduction. Radiographic bone union was confirmed at 16 and 24 weeks postoperatively, after which a progressive throwing…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
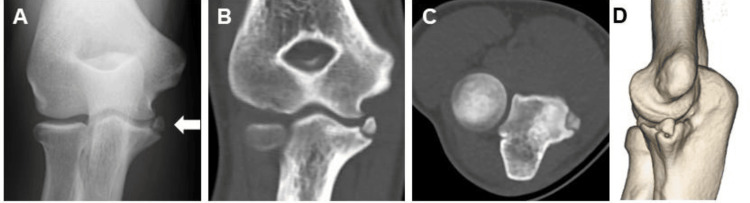 Figure 1
Figure 1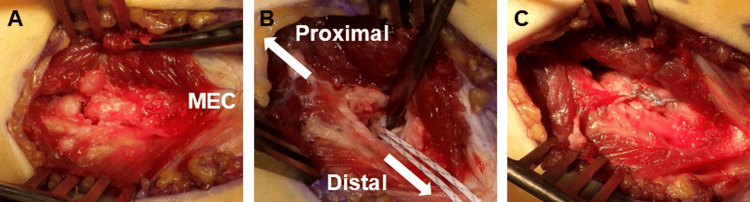 Figure 2
Figure 2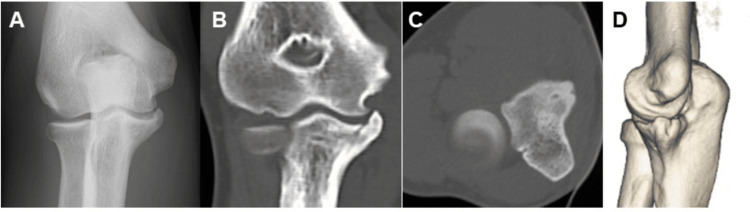 Figure 3
Figure 3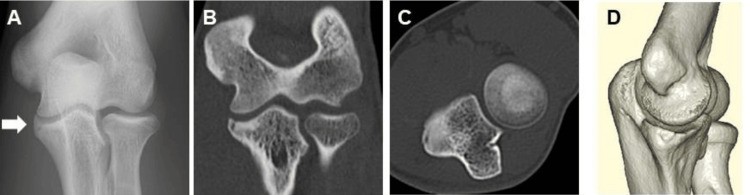 Figure 4
Figure 4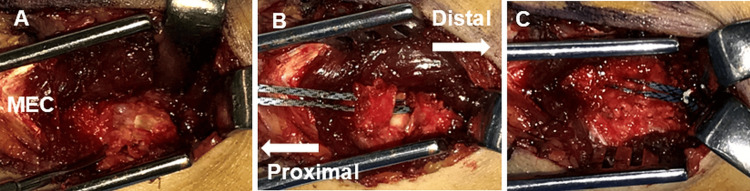 Figure 5
Figure 5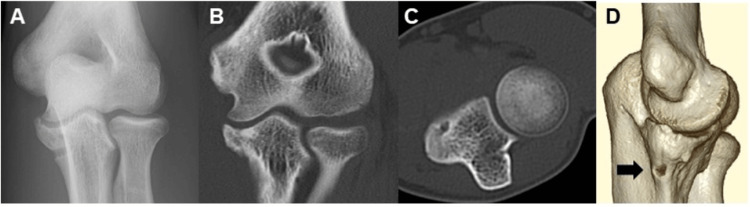 Figure 6
Figure 6| Variable | Case 1 | Case 2 |
| Age (years) | 16 | 16 |
| Hand dominance | Right-handed | Left-handed |
| Sport / Position | Baseball / Pitcher | Baseball / Pitcher |
| Affected side | Right elbow | Left elbow |
| Fragment size (mm) | 7 | 9 |
| Anchor configuration | ICONIX® suture anchor + SwiveLock® (suture bridge) | JuggerKnot® soft anchor with tape + SwiveLock® (suture bridge) |
| Reason for anchor selection | Standard suture anchor fixation | Tape-type anchor selected to enhance surface contact and distribute compressive forces |
| Time to radiographic union (weeks) | 16 | 24 |
| Post-union throwing program | Staged progression (net throwing → long-toss → bullpen) | Same as Case 1 |
| Time to bullpen pitching (weeks) | 32 | 26 |
| Time to return to competitive pitching (weeks) | 30 | 28 |
| Fastball velocity (preoperative) | 140 km/h (objectively measured) | Not objectively measured |
| Fastball velocity (postoperative, final follow-up) | 140 km/h (objectively measured) | Subjectively reported as unchanged |
| Recurrence of symptoms | None | None |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsElbow and Forearm Trauma Treatment · Shoulder Injury and Treatment · Orthopedic Surgery and Rehabilitation
Introduction
Ulnar sublime tubercle avulsion fractures are rare injuries predominantly observed in overhead throwing athletes [1-5]. This fracture involves the distal bony insertion of the anterior bundle of the medial ulnar collateral ligament (MUCL) and is thought to result from repetitive valgus overload on the medial elbow during throwing [1,3,4]. Because the anterior bundle of the MUCL has a relatively small and discrete bony footprint on the ulnar sublime tubercle, stable compression at this site is critical for achieving secure fixation. Prior studies have shown that medial epicondyle avulsion fractures, which involve the proximal MUCL attachment, occur at a mean age of 13.1 years [6], whereas sublime tubercle avulsion fractures involving the distal MUCL attachment occur at a mean age of 16.9 years [4]. This age corresponds to a period in which the physis is typically closed or nearing closure, suggesting that sublime tubercle avulsion fractures tend to arise during the later stages of skeletal maturation. Conservative management, including bracing [4], cast immobilization [2], and extracorporeal shock wave therapy (ESWT) [5], is commonly employed as the initial treatment. Surgical intervention may be required for nonunion, displaced fractures, or persistent medial elbow pain despite conservative management. Open reduction and internal fixation using a screw [1] or suture anchors [4] has been described, whereas MUCL reconstruction is reserved for irreparable fragments or cases of ligament insufficiency [7]. The suture bridge technique, originally developed for rotator cuff repair [8], has been adapted for fixation of small avulsion fragments, particularly at ligament or tendon insertions [9]. This transosseous-equivalent construct tensions suture limbs from medial anchors and secures them laterally with knotless anchors, thereby increasing stability and the tendon-bone contact area [8,9]. Giles et al. demonstrated its biomechanical advantages for bony Bankart lesions, showing reduced fragment migration and greater load-bearing capacity compared with single-row anchor repair or direct fragment suturing [7]. These findings suggest that suture bridge fixation may be broadly applicable to small bony avulsion injuries beyond the shoulder. In this study, we report two adolescent baseball players with ulnar sublime tubercle avulsion fractures treated with suture bridge fixation.
Case presentation
Case 1
A 16-year-old right-handed high school baseball pitcher presented with medial right elbow pain during throwing. He was initially evaluated at a local orthopedic clinic one month after symptom onset. After one month of conservative treatment, including rest, rehabilitation, and extracorporeal shock wave therapy (ESWT), follow-up radiographs were obtained prior to return to throwing; however, no substantial interval change compared with the initial imaging was observed, and definitive fracture healing was not confirmed. Despite the lack of radiographic healing, he returned to sports based on symptomatic improvement and remained asymptomatic while pitching for the subsequent five months. However, five months after resuming pitching, he developed recurrent medial elbow pain and was subsequently referred to our institution.
Physical examination revealed localized tenderness over the ulnar sublime tubercle and medial elbow pain with valgus stress. No mechanical symptoms, such as clicking or locking, were observed during the examination. Ultrasonographic evaluation under valgus stress demonstrated no medial joint space widening greater than 2 mm compared with the contralateral side, indicating the absence of gross valgus instability. Plain radiographs demonstrated a 7-mm displaced bony fragment at the ulnar sublime tubercle (Figure 1A), and computed tomography (CT) confirmed the morphology and displacement of the fragment (Figures 1B-1D). The physeal plate was closed on plain radiographs, indicating skeletal maturity. Given the chronic nature of the injury, failure of prior conservative management, and the patient’s desire for an expedited return to competitive pitching, surgical intervention was recommended.
Preoperative radiographic and CT findings of case 1A. Initial anteroposterior radiograph showing a small bony fragment at the ulnar sublime tubercle (white arrow). B. Coronal CT image. C. Axial CT image. D. Three-dimensional CT reconstruction.
Surgical procedure
Under general anesthesia, a standard medial elbow approach was used. A longitudinal split was made in the flexor carpi ulnaris (FCU), followed by splitting of the flexor digitorum superficialis (FDS), to expose the anterior bundle of the medial ulnar collateral ligament (MUCL) (Figure 2A). The ulnar nerve was identified and protected without routine retraction. Sharp dissection around the avulsed fragment was performed to preserve its continuity with the MUCL. The fragment was gently reflected, and the bony footprint was debrided to promote osteointegration.
Intraoperative views of case 1A. Muscle-splitting approach exposing the avulsed bone fragment. B. A soft suture anchor is inserted into the osteochondral transition zone of the footprint. C. Final appearance after completion of the suture bridge construct.
A 1.4-mm ICONIX® suture anchor (Stryker, Kalamazoo, MI, USA) was inserted proximal to the original footprint (Figure 2B). The anchor was seated to the manufacturer-recommended depth using the depth marker on the anchor, with the drill hole oriented away from the joint surface to avoid intra-articular penetration. The suture limbs were passed in a horizontal mattress configuration through the MUCL fibers just proximal to the fragment. To complete the suture bridge construct, the sutures were tensioned laterally and secured using a 3.9-mm SwiveLock® knotless anchor (Arthrex, Naples, FL, USA) placed distal to the sublime tubercle, thereby achieving anatomical reduction of the fragment (Figure 2C). The wound was then closed in layers.
Postoperative course
The elbow was immobilized in a cast for four weeks, followed by a posterior splint for an additional four weeks to minimize valgus stress until early bony healing. Gentle active range-of-motion exercises were initiated several times daily during the splinting period. After splint removal, a valgus-limiting hinged elbow brace was applied for four weeks while a structured rehabilitation program was initiated under the supervision of a physical therapist. The brace was locked to restrict valgus stress, and no specific limits were imposed on elbow flexion or extension. Rehabilitation included progressive passive and active-assisted range-of-motion exercises, along with early kinetic-chain training focusing on the lower extremities and trunk to support proper pitching mechanics.
Radiographic bone union was confirmed at 16 weeks postoperatively (Figure 3), after which a gradual throwing program was initiated. The program began with light net throwing during the first week, followed by progressive long toss up to approximately half the regulation throwing distance during the second week. Throwing intensity gradually increased to approximately 70-80% before advancing to full long toss over the subsequent week. Once the patient was able to throw at this intensity without symptoms, bullpen pitching was initiated. Because this was our first experience with this fixation technique, progression through the long-toss phase was intentionally conservative.
Postoperative radiographic and CT findings of case 1A. Postoperative anteroposterior radiograph showing satisfactory realignment of the fragment following suture bridge fixation. B. Coronal CT image. D. Three-dimensional CT reconstruction demonstrating successful bone union.
The patient returned to competitive pitching at 30 weeks postoperatively without recurrence of symptoms. Objective measurement confirmed that his fastball velocity had returned to the pre-injury level (140 km/h). Near-full pitching intensity was achieved approximately four weeks after initiation of bullpen training, and full recovery was confirmed at 36 weeks.
A 16-year-old left-handed high school baseball pitcher presented with medial left elbow pain during throwing. He had initially undergone one month of conservative management, including rest, rehabilitation, and extracorporeal shock wave therapy (ESWT), at a local orthopedic clinic. After returning to sports, he experienced recurrent medial elbow pain five months later and was subsequently referred to our institution.
Physical examination revealed localized tenderness over the ulnar sublime tubercle and medial elbow pain with valgus stress. No mechanical symptoms, such as clicking or locking, were observed during the examination. Ultrasonographic evaluation under valgus stress demonstrated no medial joint space widening greater than 2 mm compared with the contralateral side, indicating the absence of gross valgus instability. Plain radiographs demonstrated a 9-mm avulsion fragment at the ulnar sublime tubercle (Figure 4A), and computed tomography (CT) confirmed its morphology and displacement (Figures 4B-4D). The physeal plate was closed on plain radiographs, indicating skeletal maturity. Given the chronic course of symptoms, failure of prior conservative therapy, and the patient’s desire for a prompt return to competitive pitching, surgical treatment was recommended.
Preoperative radiographic and CT findings of case 2A. Initial anteroposterior radiograph showing a small bony fragment at the ulnar sublime tubercle (white arrow). B. Coronal CT image. C. Axial CT image. D. Three-dimensional CT reconstruction.
Surgical procedure
The procedure was performed using the same surgical approach and technique as described for case 1. A 1.4-mm JuggerKnot® soft anchor with tape (Zimmer Biomet, Warsaw, IN, USA) was used instead of the ICONIX® suture anchor (Figure 5). The tape-type anchor was selected to enhance surface contact and distribute compressive forces more evenly across the small avulsion fragment, allowing stable fixation while minimizing the risk of fragmentation. As in case 1, the anchor was seated to the manufacturer-recommended depth with the drill hole oriented away from the joint surface to avoid intra-articular penetration.
Intraoperative views of case 2A. Muscle-splitting approach exposing the avulsed bone fragment. B. A soft suture anchor is inserted into the osteochondral transition zone of the footprint. C. Final appearance after completion of the suture bridge construct.
Postoperative course
The elbow was immobilized in a posterior splint for six weeks. Gentle active range-of-motion exercises were initiated several times daily beginning in the fourth postoperative week to minimize joint stiffness. After splint removal, a valgus-limiting hinged elbow brace was applied for an additional four weeks while a structured rehabilitation program was initiated under the supervision of a physical therapist. The brace was locked to restrict valgus stress, and no specific limits were imposed on elbow flexion or extension. Rehabilitation included progressive passive and active-assisted range-of-motion exercises, along with early kinetic-chain training emphasizing the lower extremities and trunk.
Radiographic bone union was confirmed at 24 weeks postoperatively (Figure 6), after which a gradual return-to-throwing program was initiated. The postoperative throwing progression followed the same staged protocol as in case 1, including stepwise advancement from net throwing to long toss and subsequent bullpen pitching. The patient progressed smoothly through each phase and resumed full competitive pitching at 28 weeks postoperatively without recurrence of symptoms. At the final follow-up, the patient subjectively reported that his pitching velocity had returned to the pre-injury level, although objective velocity measurements were not obtained. Full recovery was achieved in 30 weeks (Table 1).
Postoperative radiographic and CT findings of case 2A. Postoperative anteroposterior radiograph showing anatomical realignment of the fragment following suture bridge fixation. B. Coronal CT image. C. Axial CT image. D. Three-dimensional CT reconstruction demonstrating successful bone union and the position of the lateral knotless anchor used in the suture bridge construct (black arrow).
Discussion
Surgical fixation of ulnar sublime tubercle avulsion fractures has been performed using either small screws or suture anchors. Although screw fixation can provide rigid stability, it is generally unsuitable for small avulsion fragments because of the risk of fragmentation or insufficient screw purchase. Accordingly, small avulsion fragments represent a primary indication for anchor-based fixation rather than screw-based open reduction and internal fixation. Historically, one or two anchors have been inserted into the fracture bed with transosseous bone tunnels created in the fragment for horizontal mattress suturing; however, this technique carries a risk of fragment fracture during tunnel creation or suture tightening. An alternative construct occasionally used in clinical practice involves placing anchors into the fracture bed and securing the fragment by wrapping sutures around it in a manner similar to a single-row rotator cuff repair. Compared with such constructs, suture bridge fixation may offer biomechanical advantages by providing broader footprint compression and more uniform contact pressure across the fragment surface, as demonstrated in studies comparing suture bridge and single-row constructs in rotator cuff repair [3,8].
In our cases, the fragment widths (7 and 9 mm) were unsuitable for safe screw fixation, which we consider a specific and primary indication for selecting a suture bridge technique. Based on our experience, avulsion fragments smaller than approximately 10 mm are at increased risk of fragmentation or inadequate screw purchase, making screw fixation potentially unsafe in this setting. Compared with medial ulnar collateral ligament (MUCL) reconstruction, which typically requires at least 12 months before athletes can return to throwing [10], suture bridge fixation may allow earlier functional recovery when fragment size permits secure anchor placement. This technique avoids graft harvesting and preserves native ligamentous anatomy, making it a less invasive option for skeletally immature throwing athletes. However, because the suture bridge construct can generate substantial compressive force, particularly in small avulsion fragments, careful tension control is essential. In our technique, the sutures were deliberately passed over the fragment via the attached ligament to ensure effective compression without loss of fixation, and tape-type sutures were used when appropriate to enhance surface contact and distribute compressive forces more evenly across the fragment.
Despite these advantages, successful fixation requires a sufficiently sized, non-comminuted fragment capable of supporting anchor placement. Extensive displacement, comminution, or combined ligament insufficiency may necessitate primary MUCL reconstruction rather than fragment fixation. Therefore, careful preoperative assessment of fragment morphology, displacement, and ligament integrity is essential when determining the optimal surgical strategy.
A technical challenge associated with this approach is the risk of drill-bit slippage during anchor-hole preparation along the narrow and curved surface of the distal ridge of the sublime tubercle. Precise control of drill trajectory and entry angle is required to avoid misdirection or inadequate penetration. In addition, meticulous anatomical reduction and preservation of surrounding soft tissue are critical for achieving stable fixation and promoting biological healing.
Because sublime tubercle avulsion fractures may be overlooked in adolescent throwers and can mimic traction apophysitis or medial epicondyle pathology, heightened clinical awareness is necessary for timely diagnosis. Early identification of a displaced avulsion fragment allows surgeons to consider fixation strategies that restore native valgus stability without resorting to reconstruction.
Postoperative rehabilitation in our cases emphasized restoration of range of motion, minimization of stiffness, and early kinetic-chain activation, which may reduce compensatory stress on the elbow and facilitate a safe return to throwing. Both athletes returned to competitive pitching within approximately seven months postoperatively without recurrence of symptoms or complications.
Although this report includes only two cases, sublime tubercle avulsion fractures remain rare, and the existing literature consists largely of isolated case reports. In this context, even small case series can provide meaningful clinical insights into fixation strategies for small avulsion fragments in adolescent throwers. While further biomechanical evaluation and larger multicenter studies are required to validate indications, reproducibility, and long-term outcomes, the favorable short-term recovery observed in these cases supports the clinical utility of suture bridge fixation in appropriately selected patients.
Conclusions
These cases suggest that suture bridge fixation provided stable fixation and successful union in these patients and may represent a viable option for treating ulnar sublime tubercle avulsion fractures in adolescent throwing athletes. The favorable short-term outcomes observed here support its consideration in appropriately selected patients. Sublime tubercle avulsion fractures remain underrecognized in adolescent overhead athletes, and early diagnosis is critical to prevent chronic valgus instability and prolonged time away from sport. Suture bridge fixation may provide a biomechanically stable construct in cases where conservative treatment fails, particularly in high-demand throwers who require early restoration of medial elbow stability. In particular, this technique may be well suited for small avulsion fragments in skeletally mature or near-mature adolescents, in whom screw fixation may be unsafe, and ligament reconstruction may be unnecessarily invasive. Further accumulation of cases and multicenter studies will be necessary to establish optimal surgical indications and to validate the long-term clinical outcomes of this technique.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Total avulsion fracture of the coronoid tubercle caused by baseball pitching. A case report Am J Sports Med Akagi M Ito T Ikeda N Nakamura T 5805822820001092165510.1177/03635465000280042401 · doi ↗ · pubmed ↗
- 2Nonoperative management of sublime tubercle fractures in adolescent throwing athletes: improved results with cast immobilization Orthop J Sports Med Fogleman SA Edmonds EW Fronek J 232596712412877781220243953968910.1177/23259671241287778 PMC 11558767 · doi ↗ · pubmed ↗
- 3Avulsion fracture of the sublime tubercle of the ulna: a newly recognized injury in the throwing athlete AJR Am J Roentgenol Glajchen N Schwartz ML Andrews JR Gladstone J 6276281701998949094210.2214/ajr.170.3.9490942 · doi ↗ · pubmed ↗
- 4Avulsion fracture of the ulnar sublime tubercle in overhead throwing athletes Am J Sports Med Salvo JP Rizio L 3rd Zvijac JE 4264313020021201608610.1177/03635465020300032001 · doi ↗ · pubmed ↗
- 5Extracorporeal shock wave therapy for avulsion fractures of the sublime tubercle of the ulna in high school baseball players: A report of two cases Asia Pac J Sports Med Arthrosc Rehabil Technol Tanaka K Kanamori A Yamamoto Y 131020172939210810.1016/j.asmart.2017.05.298PMC 5780296 · doi ↗ · pubmed ↗
- 6Acute, avulsion fractures of the medial epicondyle while throwing in youth baseball players: a variant of Little League elbow J Shoulder Elbow Surg Osbahr DC Chalmers PN Frank JS 9519571920102068854210.1016/j.jse.2010.04.038 · doi ↗ · pubmed ↗
- 7Suture anchor fixation of bony Bankart fractures: comparison of single-point with double-point "suture bridge" technique Am J Sports Med Giles JW Puskas GJ Welsh MF 262426314120132400775910.1177/0363546513501795 · doi ↗ · pubmed ↗
- 8Part I: Footprint contact characteristics for a transosseous-equivalent rotator cuff repair technique compared with a double-row repair technique J Shoulder Elbow Surg Park MC El Attrache NS Tibone JE 4614681620071732116110.1016/j.jse.2006.09.010 · doi ↗ · pubmed ↗