Terlipressin Treatment for Acute Esophageal Variceal Bleeding: Bolus or Infusion?
Ali Şenkaya, Ferit Çelik, İlkçe Kurtulmuş Akgün, Seymur Aslanov, Alper Uysal, Abdullah Murat Buyruk, Nalan Gülşen Ünal, İlker Turan, Ulus Salih Akarca, Zeki Karasu

TL;DR
This study compares two ways of giving terlipressin to stop esophageal bleeding and finds no major difference in effectiveness or safety.
Contribution
The study provides evidence on the comparative efficacy and safety of bolus versus infusion terlipressin for acute esophageal variceal bleeding.
Findings
No significant differences in treatment failure, rebleeding, or mortality between bolus and infusion groups.
Infusion therapy may be preferred for patient comfort and ease of administration despite similar efficacy.
No significant differences in creatinine, sodium levels, or portal vein thrombosis incidence between groups.
Abstract
This study aimed to compare the efficacy of bolus versus infusion administration of terlipressin in patients with acute esophageal variceal bleeding and to elucidate any differences in clinical outcomes between the 2 approaches. This prospective study included patients divided into 2 groups. Group 1 received a 2 mg intravenous (IV) bolus followed by 1 mg IV every 4 hours. Group 2 received a 1 mg IV bolus followed by a 4 mg terlipressin infusion over 24 hours. Clinical and laboratory parameters, hospitalization duration, need for blood product transfusion, rebleeding or mortality within 6 weeks, and drug-related side effects were evaluated. Among the 46 patients, 23 (50%) received terlipressin as an IV bolus (group 1), and 23 (50%) received it as an infusion (group 2). Treatment failure occurred in 4 patients (8.7%), all from group 1, though the difference was not statistically…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1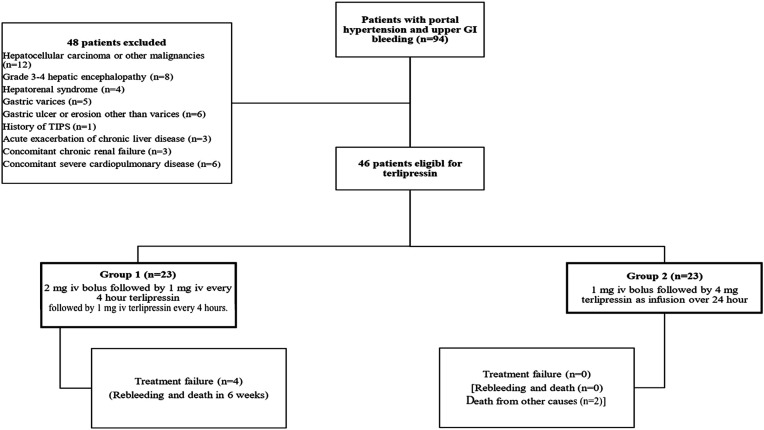 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLiver Disease and Transplantation
Introduction
Esophageal variceal bleeding is a common and life-threatening complication of portal hypertension, affecting nearly half of all patients with cirrhosis.^1^ Annually, 5%-15% of cirrhotic patients experience variceal bleeding, with reported mortality rates ranging from 7% to 20%.^2-4^ Standard treatment strategies include pharmacological agents such as vasoactive drugs, endoscopic interventions like sclerotherapy and endoscopic band ligation (EBL), and advanced modalities such as balloon tamponade, transjugular intrahepatic portosystemic shunt, or surgery.^5-7^ A combination of endoscopic and pharmacologic therapy is considered the most effective approach.^6^
Among endoscopic treatments, EBL is the most effective for acute esophageal variceal bleeding. The primary objective of endoscopic therapy is to reduce variceal wall tension and eradicate varices; however, it does not directly affect portal pressure.^8^ In contrast, medical management targets a reduction in splanchnic blood flow and portal pressure to control acute hemorrhage from esophageal varices.^9^ Vasoactive agents such as vasopressin, terlipressin, somatostatin, and octreotide are commonly employed to achieve hemostasis and prevent rebleeding.^2,9-11^
Terlipressin, a synthetic analog of vasopressin, exhibits potent vasoconstrictive activity with a relatively favorable side effect profile. Its mechanism of action involves the activation of V1 receptors located primarily on the smooth muscle of splanchnic arteries, leading to reduced splanchnic blood flow and portal pressure, thereby effectively controlling acute variceal hemorrhage.^12,13^ Terlipressin is typically administered at doses of 1-2 mg intravenously every 4 hours, although some protocols recommend a 2 mg dose every 6 hours.^5^ According to the Baveno VI consensus, terlipressin treatment should not exceed 5 consecutive days.^4^ Recent research has also demonstrated that continuous infusion of terlipressin can significantly lower portal pressure.^14,15^
Although both bolus and infusion routes are recommended for terlipressin administration in acute esophageal variceal bleeding, direct comparative studies remain limited. At the institution, terlipressin is administered using both approaches. Therefore, the present prospective study aimed to comparatively evaluate the efficacy and safety of bolus versus infusion methods of terlipressin administration in this clinical setting.
Materials and Methods
This prospective study included patients with acute esophageal variceal bleeding who underwent EBL and received terlipressin treatment in the Gastroenterology Department of Ege University hospital between January and December 2020. The diagnosis of portal hypertension was based on clinical, biochemical, ultrasonographic, and/or histopathological findings. The inclusion and exclusion criteria are summarized in Table 1, and patient data were recorded in case report forms as detailed in Table 2.
Following hemodynamic stabilization, upper gastrointestinal endoscopy was performed within 12 hours of hospital admission. Treatment failure was defined as the occurrence of 100 mL or more of fresh hematemesis within 2 hours of EBL, a decrease in hemoglobin of ≥3 g/dL without transfusion, or death. Terlipressin was administered in a sequential pattern, with 1 patient receiving bolus therapy and the next receiving infusion therapy. Based on the mode of administration, patients were divided into 2 groups. Group 1 received 2 mg of terlipressin as an intravenous (IV) bolus followed by 1 mg IV every 4 hours. Group 2 received a 1 mg IV bolus followed by a continuous infusion of 4 mg terlipressin over 24 hours.
The study was approved by the local ethics committee of Ege University (Approval date: December 25, 2019; Approval No. 19-12.1T/20) and conducted in accordance with the principles of the Declaration of Helsinki.All patients provided informed consent.
Statistical Analysis
All statistical analyses were performed using SPSS software version 22 (IBM SPSS Corp.; Armonk, NY, USA). Descriptive statistics are expressed as mean ± standard deviation (SD) for numerical variables and as frequencies and percentages for categorical variables. The Kolmogorov–Smirnov test was used to assess the normality of distribution. For comparisons between groups, the student’s t-test was used for normally distributed numerical variables, while the chi-square test or Fisher’s exact test was applied for categorical variables. Friedman’s test was employed to assess changes in laboratory parameters over time. When necessary, pairwise comparisons were conducted using the Wilcoxon signed-rank test, with Bonferroni correction applied. A 2-sided P value of <.05 was considered statistically significant.
Results
The study flowchart is presented in Figure 1. Of the 46 patients included, 23 (50%) received terlipressin as an IV bolus (group 1), and 23 (50%) received it as an IV infusion (group 2). Overall, 29 patients (63%) were male, and the mean age was 58.7 ± 12.7 years. A history of variceal bleeding was noted in 20 patients (43.5%), hepatic encephalopathy in 10 (21.7%), and prior EBL in 27 (58.7%). There were no statistically significant differences between groups regarding these variables (P = 1.000, P = .475, and P = .369, respectively).
Regarding medication history, 3 patients (6.5%) had used nonsteroidal anti-inflammatory drugs, 2 (4.3%) were on antiaggregant therapy, 4 (8.7%) were receiving anticoagulants, 20 (43.5%) were on diuretics, and 24 (52.2%) were taking prophylactic beta-blockers. There were no significant differences in medication use between the 2 groups.
At hospital admission, 16 patients (34.8%) presented with grade 1-2 hepatic encephalopathy, and 24 (52.2%) had nonrefractory mild ascites. Again, there were no significant intergroup differences (P = .536 and P = .555, respectively). However, the number of comorbidities differed significantly between the groups (P = .041). The demographic and clinical characteristics of the patients, along with their comparison by treatment type, are summarized in Table 3.
Laboratory and ultrasonographic findings are presented in Table 4. No significant differences were found between treatment groups regarding these parameters (P > .05). Similarly, endoscopic outcomes and treatment characteristics did not differ significantly between the 2 groups (Table 5).
The mean hospital stay was 9.8 ± 5.9 days. Treatment failure occurred in 4 patients (8.7%), all in group 1, although this difference was not statistically significant compared with group 2 (P = .109). Six patients experienced rebleeding and died within 6 weeks. Of these, 1 patient in group 2 died within the first 24 hours due to acute kidney injury and respiratory failure, and another in group 2 died due to acute-on-chronic liver failure (ACLF). The remaining 4 patients, all from group 1, died due to rebleeding and treatment failure. No statistically significant differences in clinical outcomes were found between treatment groups (Table 6).
There were no significant differences in serum creatinine or sodium levels between groups 1 and 2 at the beginning or end of treatment (P = .654).
During terlipressin therapy, electrocardiographic changes were observed in 4 patients—3 from group 1 and 1 from group 2. These changes included T-wave inversions in the anterior leads (n = 2), ST-segment depression (n = 1), and moderate sinus tachycardia (n = 1). None of these findings necessitated treatment discontinuation. All affected patients continued therapy following cardiology consultation.
Discussion
In this study comparing the efficacy of bolus versus infusion terlipressin treatment in patients with acute esophageal variceal bleeding, no significant differences were observed between the 2 groups regarding drug-related side effects, length of hospital stay, need for blood product transfusion, mortality, or rebleeding. These findings contribute meaningfully to the existing body of literature on terlipressin administration strategies.
Terlipressin has a half-life of approximately 50 minutes and cannot maintain therapeutic plasma levels beyond 4 hours.^16^ This pharmacokinetic limitation has led to investigations comparing bolus with continuous infusion regimens. Due to its potential for serious adverse effects—such as myocardial ischemia—terlipressin has also been used at lower doses via infusion in patients with septic shock to mitigate such risks.^17^ Moreover, low-dose infusion of terlipressin has been shown to be effective in the treatment of hepatorenal syndrome and is associated with fewer side effects than bolus administration.^18^
When administering terlipressin, it is important to monitor oxygen saturation (ensuring levels >90%) as well as signs of ischemia, arrhythmias, and blood pressure changes. Daily electrocardiography (ECG), along with monitoring of blood pressure, pulse, and oxygen saturation, are recommended. Regular evaluation of serum creatinine, sodium, and potassium levels is also essential.
In the present study, no significant differences were observed between the 2 treatment groups in terms of side effects requiring treatment discontinuation. Although ECG changes were more frequently observed in group 1, this difference was not statistically significant. These findings are consistent with those of Jha et al,^15^ who also reported no difference in adverse event profiles. In contrast, a recent study by Arora et al^19^ reported a significantly higher rate of side effects in the bolus group than the infusion group (bolus: 56.4% vs. infusion: 36.3%, P = .03). Similarly, Vaishnav et al^20^ compared 1- and 3-day bolus terlipressin regimens and found that shorter treatment duration was associated with fewer side effects (37.8% vs. 56%, P = .026). Although bolus administration is theoretically expected to be associated with more adverse events, this was not confirmed in the study.
The study found no significant differences between the bolus and infusion groups in terms of treatment efficacy, mortality, or rebleeding at 6 weeks. However, earlier studies by Jha and Arora^15,19^ reported higher rates of early rebleeding and mortality in the bolus group. In this study, 4 of the 6 total deaths occurred in group 1 and were attributed to treatment failure and rebleeding, whereas the 2 deaths in group 2 were due to respiratory failure, acute kidney injury, and ACLF. Although not statistically significant, the number of treatment failures (4 vs. 2; P = .109) and the number of patients with rebleeding and death within 6 weeks (4 vs. 2; P = .665) were higher in the bolus group, potentially supporting findings from previous studies.^15,19^
Amitrano et al^21^ suggested that the presence of portal vein thrombosis is an unfavorable prognostic factor in acute variceal bleeding. In this study, although 6 patients in group 2 had portal vein thrombosis, the number of deaths was lower in this group than in group 1, and this difference was not statistically significant. Interestingly, despite a higher burden of comorbidities in group 2, mortality was numerically lower than in group 1.
This study has several limitations. The relatively small sample size and the inability to measure hepatic venous pressure gradients limit the generalizability of the findings. Additionally, the low incidence of treatment failure and mortality restricted the statistical power to identify prognostic factors. Despite these limitations, the findings align with current evidence suggesting comparable efficacy between bolus and infusion administration, with the potential added benefits of lower drug doses, fewer side effects, and cost-effectiveness in the infusion group.
In conclusion, this study found no statistically significant differences between bolus and infusion terlipressin treatment in terms of treatment efficacy, mortality, rebleeding within 6 weeks, side effects, or treatment discontinuation. Although not statistically significant, the infusion group exhibited fewer adverse events. Based on these findings and the potential for reduced drug use and cost, terlipressin infusion therapy may be considered in the management of acute esophageal variceal bleeding.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jalan R Hayes PC . UK guidelines on the management of variceal haemorrhage in cirrhotic patients. British Society of Gastroenterology. Gut. 2000;46(Suppl 3):III 1 III 15. (10.1136/gut.46.suppl_3.iii 1)10862604 PMC 1766736 · doi ↗ · pubmed ↗
- 2D’Amico G Luca A . Natural history. Clinical-haemodynamic correlations. Prediction of the risk of bleeding. Baillieres Clin Gastroenterol. 1997;11(2):243 256. (10.1016/s 0950-3528(97)90038-5)9395746 · doi ↗ · pubmed ↗
- 3Abraldes JG Villanueva C Bañares R , et al. Hepatic venous pressure gradient and prognosis in patients with acute variceal bleeding treated with pharmacologic and endoscopic therapy. J Hepatol. 2008;48(2):229 236. (10.1016/j.jhep.2007.10.008)18093686 · doi ↗ · pubmed ↗
- 4Augustin S Altamirano J González A , et al. Effectiveness of combined pharmacologic and ligation therapy in high-risk patients with acute esophageal variceal bleeding. Am J Gastroenterol. 2011;106(10):1787 1795. (10.1038/ajg.2011.173)21625271 · doi ↗ · pubmed ↗
- 5Tripathi D Stanley AJ Hayes PC , et al. U.K. guidelines on the management of variceal haemorrhage in cirrhotic patients. Gut. 2015;64(11):1680 1704. (10.1136/gutjnl-2015-309262)25887380 PMC 4680175 · doi ↗ · pubmed ↗
- 6de Franchis R ; Baveno VI Faculty. Expanding consensus in portal hypertension: report of the Baveno VI consensus workshop: stratifying risk and individualizing care for portal hypertension. J Hepatol. 2015;63(3):743 752. (10.1016/j.jhep.2015.05.022)26047908 · doi ↗ · pubmed ↗
- 7Garcia-Tsao G Abraldes JG Berzigotti A Bosch J . Portal hypertensive bleeding in cirrhosis: risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the Study of Liver Diseases. Hepatology. 2017;65(1):310 335. (10.1002/hep.28906)27786365 · doi ↗ · pubmed ↗
- 8Poza Cordon J Froilan Torres C Burgos García A Gea Rodriguez F Suárez de Parga JM . Endoscopic management of esophageal varices. World J Gastrointest Endosc. 2012;4(7):312 322. (10.4253/wjge.v 4.i 7.312)22816012 PMC 3399010 · doi ↗ · pubmed ↗