Endoscopic Management of a Rare Intraluminal Duodenal “Windsock” Diverticulum Causing Recurrent Pancreatitis
Oguz Ozturk, Yavuz Cagir, Muhammed Bahaddin Durak, Mucahit Ergul, Ali Atay, Ilhami Yuksel

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3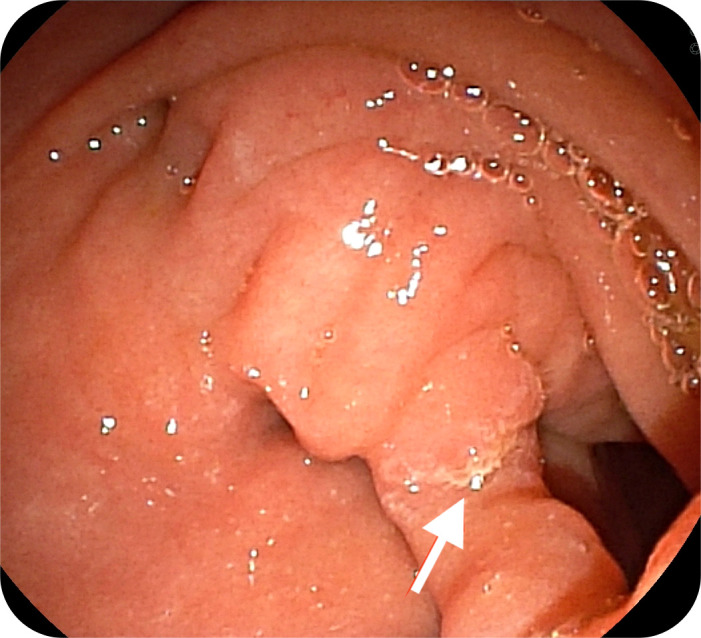 Figure 4
Figure 4 Figure 5
Figure 5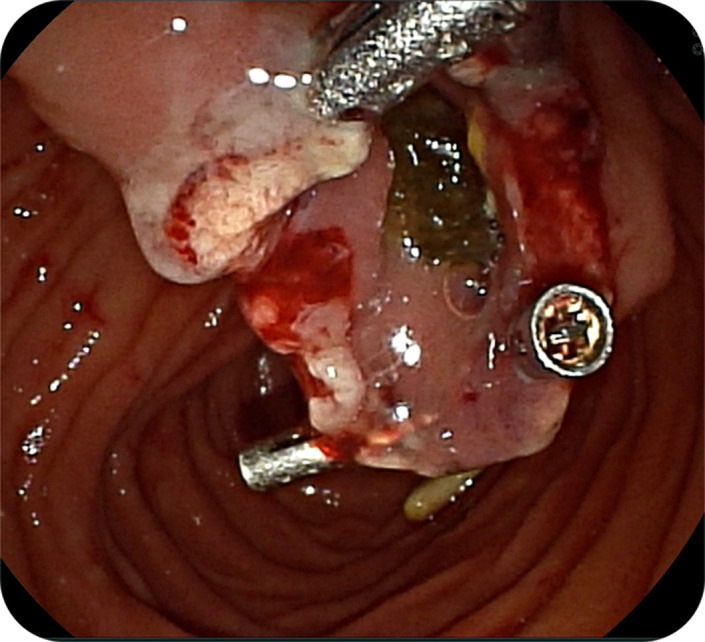 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Gallbladder and Bile Duct Disorders · Intestinal Malrotation and Obstruction Disorders
Introduction
Intraluminal duodenal diverticulum, named as windsock diverticulum, is a rare congenital anomaly caused by abnormal duodenal lumen formation due to failed embryonic recanalization. This anomaly may remain asymptomatic or manifest as dyspepsia, gastrointestinal bleeding, or symptoms related to duodenal obstruction, such as nausea, vomiting, and early satiety. In rare instances, especially when the diverticulum extends toward the ampulla of Vater, it may result in biliary or pancreatic duct obstruction, leading to recurrent acute pancreatitis.1
Case Presentation
A 22-year-old female applied for recurrent acute pancreatitis, having experienced 3 episodes over the previous year. Verbal informed consent was obtained. Her symptoms persisted despite pancreatic duct stenting performed at another institution. Magnetic resonance cholangiopancreatography was utilized to exclude alternative causes such as choledocholithiasis, strictures, or pancreatic masses. Side-viewing endoscopy confirmed a “windsock” diverticulum with the papillary orifice opening at the septal margin between the diverticulum and the duodenum (Figures 1 and 2).
Endoscopy revealed an intraluminal bulge separate from the duodenal lumen. A side-viewing endoscope was used to perform snare resection (Figure 3). Oozing bleeding occurred post-resection, and homeostasis was achieved with hemoclips (Figure 4). Histopathological examination confirmed the diagnosis of an epithelial-lined pouch, consistent with a windsock diverticulum, and excluded a duodenal duplication cyst. The patient experienced complete resolution of symptoms with no further episodes for 9 months of follow-up.
Discussion
The occurrence of pancreatitis as a result of a windsock diverticulum is an uncommon event. The proposed mechanism of the observed phenomenon may be functional ampullary obstruction or diverticulum occlusion with resultant debris accumulation. Another potential causative factor may be dyskinesia, which could result in intermittent blockage and subsequent development of pancreatitis. Biliary obstruction has also been documented in the extant literature.2^,^3 The differential diagnoses for this condition include the following: periampullary diverticula, duodenal duplication cysts, and congenital duodenal stenosis. It is notable that in the presented case, endoscopic examination from the lateral perspective proved to have a pivotal role in confirming the diagnosis.
The implementation of pancreatic duct stenting can offer symptomatic relief, though repeated procedures may be necessary. The endoscopic procedure with snare resection is a minimally invasive and definitive treatment. Previous reports have indicated favorable results when utilizing this method.4 Another recent case of a windsock-shaped intraluminal duodenal diverticulum was reported and treated successfully with endoscopic diverticulectomy, further supporting the safety and efficacy of this technique.5
Conclusion
This case underscores the utility of endoscopic snare resection as a safe and effective treatment for symptomatic windsock diverticulum. Given that endoscopic imaging is essential for diagnosis and therapeutic planning. Endoscopic resection may prevent recurrence, decrease complications, and obviate the need for repeated interventions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pumberger W Maier-Hiebl B Kargl S. Recurrent pancreatitis due to an intraluminal duodenal diverticulum: report of a case. Surg Today. 2012;42(6):589 592. (doi: 10.1007/s 00595-012-0123-y) 22270334 · doi ↗ · pubmed ↗
- 2Karagyozov P Tishkov I Georgieva Z Boeva I Tzankov D. Intraluminal duodenal (“windsock”) diverticulum: a rare cause of biliary obstruction and acute pancreatitis in the adult. Endosc Int Open. 2019;7(1):E 87 E 89. (doi: 10.1055/a-0808-3834) 30652119 PMC 6333535 · doi ↗ · pubmed ↗
- 3Antaki F Tringali A Deprez P A case series of symptomatic intraluminal duodenal duplication cysts: presentation, endoscopic therapy, and long-term outcome (with video). Gastrointest Endosc. 2008;67(1):163 168. (doi: 10.1016/j.gie.2007.08.006) 18155438 · doi ↗ · pubmed ↗
- 4Law R Topazian M Baron T. Endoscopic treatment of intraluminal duodenal (“windsock”) diverticulum: varying techniques from five cases. Endoscopy. 2012;44(12):1161 1164. (doi: 10.1055/s-0032-1325757) 23188665 · doi ↗ · pubmed ↗
- 5ÖdemişB Başpınar B ErdoğanÇ Ogutmen Koc D Özel Coşkun BD Torun S. A rare case of a windsock-shaped intraluminal duodenal diverticulum treated successfully with endoscopic diverticulectomy. Endoscopy. 2022;54(S 02):E 914 E 915. (doi: 10.1055/a-1864-9201) 35777382 PMC 9735393 · doi ↗ · pubmed ↗