Effect of Early Administration of Anti‐MRSA Drugs for Febrile Neutropenia in Allogeneic Hematopoietic Cell Transplantation
Anna Akaogi, Junya Kanda, Fumiya Wada, Yasuyuki Arai, Chisaki Mizumoto, Toshio Kitawaki, Kouhei Yamashita, Akifumi Takaori‐Kondo

TL;DR
Early use of anti-MRSA drugs in patients with febrile neutropenia after a bone marrow transplant may help reduce fever duration and lower the risk of complications in older patients.
Contribution
This study provides evidence that early administration of anti-MRSA drugs improves fever resolution and reduces aGVHD risk in older allo-HCT patients.
Findings
Early administration of anti-MRSA drugs was associated with shorter fever duration (p = 0.044).
Late administration was linked to a lower chance of fever resolution by Day 7 (OR: 0.45).
Older patients with late anti-MRSA drug use had increased aGVHD risk (HR: 2.22).
Abstract
In febrile neutropenia (FN), the empirical use of anti‐methicillin‐resistant Staphylococcus aureus (MRSA) drugs is recommended, particularly when mucosal damage occurs during fluoroquinolone antibiotic administration. Therefore, the early use of anti‐MRSA drugs may be recommended in many cases of FN after allogeneic hematopoietic cell transplantation (allo‐HCT), but the evidence regarding their efficacy is limited. To assess the impact of early administration of anti‐MRSA drugs on the resolution of fever in patients undergoing allo‐HCT. We retrospectively analyzed 186 allo‐HCT patients. Patients receiving anti‐MRSA drugs within 3 days of fever onset formed the early‐decision group; those treated on or after Day 4 or untreated formed the late‐decision group. The early group showed a significantly shorter fever duration than the late group. (p = 0.044). Multivariate logistic regression…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
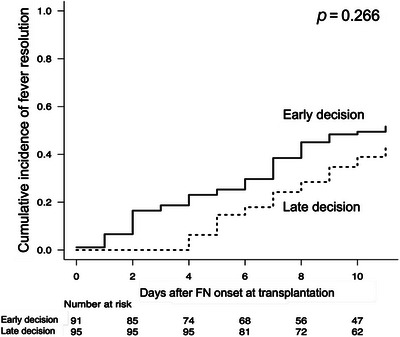 FIGURE 1
FIGURE 1| Characteristics | Overall ( | Early decision group ( | Late decision group ( |
| ||
|---|---|---|---|---|---|---|
| Age at transplant | 55.00 [17.00, 70.00] | 44.00 [17.00, 68.00] | 55.00 [20.00, 70.00] | < 0.001 | ||
| Recipient sex | Female | 74 (39.8) | 29 (31.9) | 45 (47.4) | 0.036 | |
| Male | 112 (60.2) | 62 (68.1) | 50 (52.6) | |||
| Disease | AML | 74 (39.8) | 40 (44.0) | 34 (35.8) | 0.657 | |
| ALL | 30 (16.1) | 14 (15.4) | 16 (16.8) | |||
| CML | 7 (3.8) | 4 (4.4) | 3 (3.2) | |||
| MDS | 27 (14.5) | 10 (11.0) | 17 (17.9) | |||
| MPAL | 1 (0.5) | 1 (1.1) | 0 (0.0) | |||
| NHL | 24 (12.9) | 10 (11.0) | 14 (14.7) | |||
| HL | 2 (1.1) | 1 (1.1) | 1 (1.1) | |||
| ATL | 11 (5.9) | 5 (5.5) | 6 (6.3) | |||
| Other lymphoma | 4 (2.2) | 1 (1.1) | 3 (3.2) | |||
| Plasma cell neoplasm | 2 (1.1) | 2 (2.2) | 0 (0.0) | |||
| Other | 4 (2.2) | 3 (3.3) | 1 (1.1) | |||
| Source of stem cells | Bone marrow | 101 (54.3) | 49 (53.8) | 52 (54.7) | 0.542 | |
| Peripheral blood | 18 (9.7) | 11 (12.1) | 7 (7.4) | |||
| Cord blood | 67 (36.0) | 31 (34.1) | 36 (37.9) | |||
| Conditioning regimen | Myeloablative | 109 (58.6) | 59 (64.8) | 50 (52.6) | 0.103 | |
| CY + TBI regimen | 79 (42.5) | 47 (51.6) | 32 (33.7) | |||
| Other TBI regimen | 1 (0.5) | 0 (0.0) | 1 (1.1) | |||
| BU + CY regimen | 11 (5.9) | 6 (6.6) | 5 (5.3) | |||
| Other non TBI regimen | 18 (9.7) | 6 (6.6) | 12 (12.6) | |||
| Reduced intensity | 77 (41.4) | 32 (35.2) | 45 (47.4) | |||
| FL + BU regimen | 7 (9.1) | 5 (15.6) | 2 (4.4) | |||
| FL + CY regimen | 1 (1.3) | 0 (0.0) | 1 (2.2) | |||
| FL + Mel regimen | 68 (88.3) | 27 (84.4) | 41 (91.1) | |||
| Other regimen | 1 (1.3) | 0 (0.0) | 1 (2.2) | |||
| GVHD prophylaxis | CyA based | 15 (8.1) | 8 (8.8) | 7 (7.4) | 0.792 | |
| Tac based | 171 (91.9) | 83 (91.2) | 88 (92.6) | |||
| Use of ATG | No | 181 (97.3) | 90 (98.9) | 91 (95.8) | 0.369 | |
| Yes | 5 (2.7) | 1 (1.1) | 4 (4.2) | |||
| Disease status | CR | 118 (63.4) | 61 (67.0) | 57 (60.0) | 0.63 | |
| Non CR | 36 (19.4) | 16 (17.6) | 20 (21.1) | |||
| Untreated | 32 (17.2) | 14 (15.4) | 18 (18.9) | |||
| HLA compatibility | Match | 95 (51.1) | 47 (51.6) | 48 (50.5) | 0.885 | |
| Mismatch | 91 (48.9) | 44 (48.4) | 47 (49.5) | |||
| Variable | Univariate | Multivariate | |||
|---|---|---|---|---|---|
| OR (95% CI) |
| OR (95% CI) |
| ||
| Anti‐MRSA drug administration | Early decision | 1 | Reference | 1 | Reference |
| Late decision | 0.51 (0.27−0.96) | 0.037 | 0.45 (0.22−0.92) | 0.028 | |
| Age at transplant (continuous) | 1.02 (1.00−1.04) | 0.099 | 1.03 (1.00−1.06) | 0.044 | |
| Disease status | CR | 1 | Reference | 1 | Reference |
| Non CR | 0.47 (0.19−1.14) | 0.096 | 0.49 (0.19−1.29) | 0.149 | |
| Untreated | 1.94 (0.89−4.25) | 0.095 | 1.47 (0.59−3.66) | 0.403 | |
| Source of stem cell | Bone marrow | 1 | Reference | 1 | Reference |
| Peripheral blood | 3.12 (1.16−8.39) | 0.024 | 3.30 (1.08−10.10) | 0.037 | |
| Cord blood | 0.51 (0.26−1.01) | 0.054 | 1.12 (0.39−3.23) | 0.835 | |
| Disease | Myeloid | 1 | Reference | — | — |
| Lymphoid | 0.60 (0.31−1.15) | 0.124 | — | — | |
| Conditioning | MAC | 1 | Reference | — | — |
| RIC | 1.50 (0.80−2.81) | 0.201 | — | — | |
| HLA | Match | 1 | Reference | 1 | Reference |
| Mismatch | 0.52 (0.28−0.99) | 0.045 | 0.51 (0.20−1.31) | 0.164 | |
| Mucosal disorder | Mild | 1 | Reference | 1 | Reference |
| Severe | 1.92 (1.01−3.62) | 0.045 | 1.91 (0.94−3.90) | 0.076 | |
| Subgroup | No. of events | OR (95% CI) |
| |
|---|---|---|---|---|
| Mucosal disorder | Mild | 119 | 0.59 (0.22−1.56) | 0.288 |
| Severe | 67 | 0.36 (0.12−1.11) | 0.075 | |
| Age at transplant | < 51 | 93 | 0.46 (0.15−1.37) | 0.162 |
| ≥ 51 | 93 | 0.44 (0.17−1.16) | 0.097 | |
| Disease Status | CR | 118 | 0.42 (0.17−1.00) | 0.049 |
| Non CR | 36 | — | — | |
| Untreated | 32 | 0.72 (0.12−4.48) | 0.723 | |
| Source of stem cells | Bone marrow | 101 | 0.28 (0.11−0.75) | 0.011 |
| Peripheral blood | 18 | 0.21 (0.01−3.26) | 0.263 | |
| Cord blood | 67 | 1.12 (0.29−4.29) | 0.87 | |
| HLA compatibility | Match | 95 | 0.31 (0.11−0.81) | 0.018 |
| Mismatch | 91 | 0.68 (0.23−1.97) | 0.474 | |
| Variable | Univariate | Multivariate | |||
|---|---|---|---|---|---|
| HR (95% CI) |
| HR (95% CI) |
| ||
| Anti‐MRSA drug administration | Early decision | 1 | Reference | 1 | Reference |
| Late decision | 1.39 (0.90−2.15) | 0.14 | 1.42 (0.92−2.19) | 0.12 | |
| Age at transplant (continuous) | 1.00 (0.99−1.02) | 0.76 | — | — | |
| Disease status | CR | 1 | Reference | — | — |
| Non CR | 0.94 (0.54−1.63) | 0.836 | — | — | |
| Untreated | 1.18 (0.70−1.99) | 0.54 | — | — | |
| Source of stem cell | Bone marrow | 1 | Reference | — | — |
| Peripheral blood | 0.53 (0.22−1.29) | 0.16 | — | — | |
| Cord blood | 1.33 (0.86−2.04) | 0.2 | — | — | |
| HLA compatibility | Match | 1 | Reference | 1 | Reference |
| Mismatch | 1.58 (1.02−2.44) | 0.041 | 1.6 (1.03−2.49) | 0.036 | |
| Conditioning regimen | MAC | 1 | Reference | — | — |
| RIC | 1.06 (0.68−1.65) | 0.79 | — | — | |
| Disease | Myeloid | 1 | Reference | — | — |
| Lymphoid | 1.15 (0.74−1.78) | 0.53 | — | — | |
| Mucosal disorder | Mild | 1 | Reference | — | — |
| Severe | 0.71 (0.44−1.14) | 0.15 | — | — | |
| Subgroup | No. of events | HR (95% CI) |
| |
|---|---|---|---|---|
| Mucosal disorder | Mild | 119 | 1.43 (0.84−2.44) | 0.19 |
| Severe | 67 | 1.25 (0.56−2.76) | 0.58 | |
| Age | < 51 | 93 | 0.86 (0.44−1.69) | 0.67 |
| ≥ 51 | 93 | 2.22 (1.06−4.64) | 0.034 | |
| Disease Status | CR | 118 | 1.06 (0.61−1.84) | 0.84 |
| Non CR | 36 | 1.70 (0.55−5.24) | 0.36 | |
| Untreated | 32 | 2.74 (0.84−8.96) | 0.1 | |
| Source of stem cell | Bone marrow | 101 | 1.81 (0.96−3.40) | 0.066 |
| Peripheral blood | 18 | 1.04 (0.19−5.82) | 0.96 | |
| Cord blood | 67 | 1.10 (0.54−2.05) | 0.89 | |
| HLA compatibility | Match | 95 | 1.25 (0.64−2.43) | 0.52 |
| Mismatch | 91 | 1.53 (0.86−2.70) | 0.15 | |
- —JSPS KAKENHI
- —Takeda Science Foundation10.13039/100007449
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeutropenia and Cancer Infections · Blood disorders and treatments · Immune Response and Inflammation
Introduction
1
Febrile neutropenia (FN) is a common complication of allogeneic hematopoietic cell transplantation (allo‐HCT), with treatment strategies varying across institutions and cases. The empirical use of anti‐methicillin‐resistant Staphylococcus aureus (MRSA) drugs, such as vancomycin, teicoplanin, and daptomycin, is not universally recommended for FN. However, empiric administration is recommended in cases of hemodynamic instability, Gram‐positive cocci detected in blood culture, severe catheter infection or skin and soft tissue infection, prior fluoroquinolone prophylaxis with mucositis, and MRSA or penicillin‐resistant Streptococcus pneumoniae infection [1, 2]. Allo‐HCT patients are at high risk for these conditions. Therefore, the early use of anti‐MRSA drugs is recommended in many cases of FN after allo‐HCT. However, in practice, these drugs are often initiated based on blood culture results or as additional therapy when the patient does not respond well to the initial treatment.
In contrast, many cases of Viridans group streptococci (VGS) and S. aureus are treated with cefepime, and some authors have questioned the necessity of additional anti‐MRSA drug administration [3]. However, this study was conducted in the general population, and it is not appropriate to apply the results to the patient population of allo‐HCT patients, where delays in appropriate antibiotic administration can be fatal. Against this background, we performed a retrospective analysis to assess the impact of the early administration of anti‐MRSA drugs on the course of FN in allo‐HCT patients. We also analyzed the effects of the timing of anti‐MRSA drug administration on the course of transplantation.
Methods
2
Study Cohort and Design
2.1
From January 2008 to December 2019, a total of 229 consecutive allo‐HCT patients who did not receive antibiotics on Day 0 and developed FN were included in the study. A total number of 43 patients who recovered from fever within 3 days without receiving anti‐MRSA drugs were excluded. This left 186 patients for the analysis. There were no established criteria for the administration of anti‐MRSA drugs at the facility, and the decision was made by the physician based on individual case evaluations. In principle, Kyoto University Hospital restricts the use of prophylactic antimicrobial agents, including allo‐HCT, for the treatment of hematopoietic malignancies. This restriction is primarily aimed at preventing the emergence of fluoroquinolone‐resistant Gram‐negative bacteria, including multidrug‐resistant Pseudomonas aeruginosa [4]. Additionally, evidence that antibiotics do not show a statistically significant difference in all‐cause or infection‐related mortality rates supports this restriction [5]. This study was approved by the Kyoto University Ethics Committee and adhered to the principles of the Declaration of Helsinki. Informed consent was obtained from all the patients. The variables presented in the tables and figures were retrospectively gathered from the patients' medical records.
Endpoints
2.2
The primary endpoint was the success rate of fever resolution on Day 7 after the onset of FN. Secondary endpoints included engraftment rate, hospital stay duration, incidence of Grade II–IV acute graft‐versus‐host disease (aGVHD), and non‐relapse mortality (NRM). Additionally, the difference in renal function between the early‐ and late‐decision groups was assessed based on creatinine values on Days 1 and 7 of anti‐MRSA drug administration.
Definitions
2.3
Patients receiving anti‐MRSA drugs within 3 days of fever onset formed the early‐decision group. Those treated on or after Day 4 or untreated constituted the late‐decision group. Fever was defined as ≥ 37.5°C, and resolution as maintaining < 37.5°C for 72 h. The analysis only considered the first fever after transplantation. Mucosal disorders include lesions of the oral mucosa and gastrointestinal tract. The severity of lesions was classified according to the CTCAE v5.0 criteria [6], with Grade III or higher disorders being classified as severe and Grade I–II as mild. Patients with lesions in both the oral and gastrointestinal tracts, where either one or both were severe, were classified into the severe group, whereas the others were classified into the mild group.
Statistical Analysis
2.4
In terms of patient background, continuous variables were summarized as medians and ranges and compared using the Mann–Whitney U test. Categorical variables were summarized as numbers and percentages and compared using Fisher's exact test. Multivariate logistic regression analysis was used to analyze the association between background and fever resolution rate on Day 7 after FN onset. The variables included the timing of anti‐MRSA drug administration, age at transplantation, disease type (myeloid vs. lymphoid), transplant source, conditioning intensity, disease stage, and HLA compatibility (full match vs. others). GVHD prophylaxis and ATG use were not included as covariates because cyclosporine and ATG were used in only a small number of cases (8.1% and 2.7% of the total cohort, respectively). The incidences of fever resolution, aGVHD, engraftment rate, discharge, and NRM were analyzed using cumulative incidence methods; death without event was defined as a competing factor for the incidences of fever resolution, aGVHD, engraftment rate, and discharge, and relapse was defined as a competing factor for NRM. These were compared using Gray's test. Fine and Gray proportional hazards models were used for multivariate analysis. For the analysis of FN, follow‐up for each patient was defined as the time from FN onset to confirmed fever resolution, or to the date of death if fever resolution was not achieved. Serum creatinine levels on Day 1 and Day 7 of anti‐MRSA drug administration were compared between the early and late‐decision groups using the Mann–Whitney U test. Statistical significance was set at p < 0.05. R (version 3.1.1; R Development Core Team) and EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan) were used for statistical analyses [7].
Result
3
Patient Characteristics
3.1
Table 1 presents the clinical characteristics of the entire patient cohort and compares the early and late anti‐MRSA drug‐decision groups. The early‐decision group consisted of 91 patients, and the late‐decision group consisted of 95 patients. The underlying diseases included acute myeloid leukemia (74 patients), acute lymphoblastic leukemia (30 patients), chronic myeloid leukemia (7 patients), myelodysplastic syndrome (27 patients), and other malignancies. The median age at HCT was 55 years (range: 17–70), with 112 males and 74 females. The disease status was complete remission (CR) in 118 patients, non‐CR in 36, and no high‐intensity chemotherapy treatment in 32. The conditioning regimens included myeloablative conditioning (MAC) in 109 patients and reduced‐intensity conditioning (RIC) in 77. The transplant sources were the bone marrow (101 cases), peripheral blood (18 cases), and cord blood (67 cases), with HLA matching in 95 cases and mismatch in 91 cases. Acute GVHD prophylaxis included cyclosporine in 15, tacrolimus in 171, and ATG in 5 patients. Age and sex varied between the early‐ and late‐decision groups (*p *< 0.001 and 0.036), but the other characteristics were similar.
Success Rate of Fever Resolution in all Patients
3.2
The median number of days from hematopoietic cell infusion to FN onset was 5 days (range: 1–19 days) in the early‐decision group and 6 days (range: 1–27 days) in the late‐decision group, with no significant difference between the two groups (p = 0.23). The number of days from FN onset to fever resolution was significantly shorter in the early‐decision group than in the late‐decision group (median 11.0 vs. 12.0 days, p = 0.044) (Figure S1). The cumulative incidence of fever resolution on Day 7 after FN onset in the entire cohort was 38.5% (95% CI: 29%–48%) in the early‐decision group and 24.2% (95% CI: 16%–33%) in the late‐decision group (Figure 1), with no significant difference (*p *= 0.266). In the multivariate analysis, a negative correlation was found between the late‐decision group and successful resolution (OR: 0.45 [95% CI 0.22–0.92], p = 0.028) (Table 2).
Effect of early or late decision of anti‐MRSA drug administration on fever resolution.
Success Rate of Fever Resolution Stratified by Patient and Transplant Backgrounds
3.3
Multivariate analyses were performed according to the degree of mucosal damage, age, disease status, HLA compatibility, and source of transplantation (Table 3). The results showed lower resolution rates in the late‐decision group, regardless of patient background, except in cases of cord blood transplantation; however, most of these differences were not statistically significant. In cases with severe mucosal disorders, the odds ratio in the late‐decision group was lower than that in the analysis of the entire cohort (OR: 0.36 [0.12–1.11], p = 0.075).
Days to Engraft and Discharge
3.4
For engraftment and discharge after FN onset, the cumulative incidence rates of the late‐decision group were compared with those of the early‐decision group. On the Day 30 after the onset of fever, the cumulative incidence rates of engraftment were 87.8% in the early‐decision group (95% CI: 79%–93%) and 86.3% in the late‐decision group (95% CI: 78%–92%), with no significant difference (p = 0.332). At the Day 60, the cumulative discharge rates were 38.5% in the early‐decision group (95% CI: 29%–48%) and 43.2% in the late‐decision group (95% CI: 33%–53%); however, the difference was not significant (p = 0.272).
Acute GVHD Incidence
3.5
On Day 100 from FN onset, the cumulative incidence of Grade II–IV aGVHD was 38.8% (95% CI: 29%–49%) in the early‐decision group and 47.4% (95% CI: 37%–57%) in the late‐decision group (p = 0.123) (Figure S2). Multivariate analysis showed an HR of 1.42 (95% CI: 0.92–2.19, p = 0.12) for aGVHD in the late‐decision group compared to the early‐decision group (Table 4). No significant correlation was observed between the timing of MRSA drug administration and the development of aGVHD in the entire cohort. However, in a stratified analysis, the incidence of Grade II–IV aGVHD was significantly higher in the late‐decision group in patients aged 51 years or older (HR: 2.22 [1.06–4.64], p = 0.034) (Table 5).
Blood Culture Results
3.6
In Tables S1 and S2, the blood culture outcomes of the initial FN episodes are described for the 186 patients included in the study. Among them, 58 had positive blood cultures. In the early anti‐MRSA medication group, 33 of 91 patients had positive blood cultures, whereas in the late‐decision group, 25 of 95 patients had positive cultures. The positivity rate did not differ significantly between the groups (p = 0.157). The total number of positive cultures was 79, with 46 Gram‐positive, 32 Gram‐negative, and one fungus (Candida albicans). Gram‐positive bacteria were significantly more prevalent in the early‐decision‐making group (p < 0.001). The reasons for deciding to administer anti‐MRSA drugs in the early‐decision group are shown in Table S3. In addition to blood culture results, these reasons included the presence of mucosal damage, focal signs of infection, such as in the skin or central venous catheter, hemodynamic instability, the physician's judgment that fever resolution was delayed, and a history of MRSA or Vancomycin‐resistant Enterococcus infection.
The study also assessed fever resolution rates while excluding cases in which decisions on anti‐MRSA drug administration based on blood culture results were made within 3 days of fever onset. Thus, in this cohort, the decision regarding the initiation and timing of anti‐MRSA drugs was made based on factors other than blood culture results. This analysis covered 149 cases, removing 19 from the early‐decision group, in which Gram‐positive bacteria led to anti‐MRSA administration, and 18 from the late‐decision group, in which Gram‐negative bacteria led to withholding. The results showed that the rate of fever resolution tended to be lower in the late‐decision group (OR: 0.45 [0.21–1.01], p = 0.052) (Table S4). In the stratified analysis, fever resolution rates were lower in the late‐decision group, regardless of patient background (Table S5). Similarly, when examining the impact of anti‐MRSA drug timing on the development of Grade II–IV aGVHD in this cohort, no association was observed in all patients (Table S6). However, patients aged 51 years or older and those with HLA mismatch in the late anti‐MRSA decision group showed a significant increase in aGVHD incidence (HR: 2.66, 95% CI: 1.23–5.77, p = 0.013, and HR: 1.85, 95% CI: 1.06–3.23, p = 0.031, respectively.) (Table S7).
Empiric Antibiotic Therapy
3.7
In the analyzed cohort, the β‐lactam antibiotics used included cefepime, meropenem, and piperacillin/tazobactam. There was no significant difference between the early‐ and late‐decision groups in the use of β‐lactam antibiotics with anaerobic coverage (meropenem and piperacillin/tazobactam) (p = 0.814).
NRM
3.8
The incidence of NRM at Day 100 after FN onset was 8.9% (95% CI: 4.1%–15.7%) in the early‐decision group and 5.3% (95% CI: 2.0%–11.2%) in the late‐decision group (p = 0.329). No significant differences were observed between the two groups (Figure S3).
Renal Function
3.9
The median serum creatinine level was 0.63 and 0.60 mg/dL in the early‐decision group and late‐decision group, respectively, on Day 1 of anti‐MRSA drug administration, with no significant difference between the two groups (p = 0.327). On Day 7, the median serum levels were 0.63 and 0.59 mg/dL in the early and late groups, respectively. Similarly, there was no significant difference between the two groups (p = 0.49) (Figure S4).
Discussion
4
In this study, we demonstrated that an early decision to administer anti‐MRSA drugs results in the rapid resolution of fever in FN after allo‐HCT. We consider early fever resolution to be an important indicator reflecting the early suppression of inflammation in FN. Furthermore, it should be regarded as a clinically meaningful outcome in terms of ensuring careful systemic management after transplantation and relieving patient discomfort at an early stage. Stratified analysis revealed higher resolution rates in the early‐decision group, regardless of patient background, except in cases involving cord blood transplantation. Additionally, among patients aged 51 years or older, the incidence of Grade II–IV acute GVHD was significantly lower in the early‐decision group, suggesting that older individuals may benefit from early administration of anti‐MRSA drugs.
A controlled study comparing persistent FN patients who were administered either placebo or placebo with added anti‐MRSA drugs showed no difference in the fever resolution rate [8, 9]. Similarly, the Japanese guidelines state that even in cases where fever persists 3 to 4 days after the onset of FN, the same initial antibiotics can be continued if there are no other significant findings besides fever and the patient is in good condition [10]. In contrast, in our study, the group that initiated anti‐MRSA medication within 3 days of fever onset had a significantly higher rate of fever resolution on FN Day 7 than the group that received it after 4 days of fever or did not receive it. This disparity in results may be attributed to the differences in patient populations, as our study included only allo‐HCT cases. The median time to fever resolution in our study cohort was 12 days, which differed from the median time to fever resolution of 5 days in the general FN population [11]. Patients receiving fluoroquinolone prophylaxis were excluded from this study because of their small sample size. These results suggest that early administration of anti‐MRSA drugs may be effective in allo‐HCT even in the absence of fluoroquinolone administration. Because infections treated with fluoroquinolone prophylaxis are more likely to be caused by Gram‐positive bacteria [12], an earlier decision to administer anti‐MRSA drugs is likely to contribute to a more frequent resolution of fever in centers where fluoroquinolone prophylaxis is administered.
Several factors contribute to early fever resolution in allo‐HCT‐FN with the early administration of anti‐MRSA drugs. Previous reports indicate that the breakdown of blood cultures in early allo‐HCT is 50.6%–52.5% Gram‐positive and 41.6%–47.5% Gram‐negative bacteria [13, 14], highlighting the importance of vigilance for Gram‐positive bacteria. Additionally, the insertion of central venous catheters in almost all patients increases the risk of Gram‐positive bacterial infections, including S. aureus and Staphylococcus epidermidis. Furthermore, in allo‐HCT, despite the small number of cases that do not experience fever at the time of engraftment, bacteremia occurs in only 25%–53.3% of cases [13, 14, 15, 16]. Even in our study cohort, in which all patients developed FN, 31.0% of patients had positive blood cultures at the time of engraftment, which is consistent with previous reports. Thus, in more than half of the cases, the organisms were not identified by blood culture, and the decision to add antibiotics based solely on blood culture results was not an appropriate strategy. In the early‐decision group, the detection rate of Gram‐positive bacteria was significantly higher than in the late‐decision group. This high detection rate suggests that, in many cases, the prediction of Gram‐positive bacterial infections based on clinical findings, including mucosal damage, was correct. To eliminate the influence of biases from blood culture results, we conducted an analysis excluding cases where the decision to administer anti‐MRSA drugs was based on blood culture results, focusing on 149 cases. The results showed that, even in this group, early administration of anti‐MRSA drugs contributed to early fever resolution. Therefore, it is worthwhile to administer anti‐MRSA drugs without waiting for the blood culture results.
The fact that patients with severe mucosal disorders benefit from early administration of anti‐MRSA drugs may be related to infections caused by commensal bacteria in the oral and gastrointestinal tracts. Barrier failure due to damage to the oral mucosa can act as a gateway for VGS, a commensal organism in the oral cavity. In the gastrointestinal tract, problems caused by mucosal barrier failure are related to enteric bacteria in the gastrointestinal tract, including Enterococcus spp. VGS and Enterococcus faecium, among enterococci, are important causes of severe infections in neutropenic hosts [17, 18]. The presence of penicillin‐resistant strains of VGS and E. faecium may increase the need for anti‐MRSA drug therapy in allo‐HCT cases with barrier failure.
Furthermore, the lower incidence of Grade II–IV aGVHD in the early‐decision group of patients aged 51 years or older may be due to the early decline of FN‐induced cytokines, such as IL‐2Rα, TNFR‐1, HGF, and IL‐8, which are known biomarkers of aGVHD. In particular, high serum IFNγ levels on Day 6 of transplantation are considered to be a risk factor for the development of aGVHD [19]. Early resolution of fever and suppression of inflammatory cytokines may decrease the incidence of aGVHD.
This study has several limitations. First, one limitation of this study is the potential for lead time bias: by definition, patients in the late‐decision group received anti‐MRSA drugs later, making a direct comparison of the number of days from fever onset to resolution between the early‐ and late‐decision groups inherently unfair. To support our findings, we conducted an additional analysis using a Cox proportional hazards model in which anti‐MRSA drug administration was treated as a time‐dependent covariate. As a result, the fever resolution on FN Days 8, 9, 10, or 11 was significantly associated with the use of anti‐MRSA drugs (data not shown). These findings support the notion that anti‐MRSA therapy is effective in patients undergoing allo‐HCT and that many of these patients may have a latent need for such treatment. Second, this was a single‐center retrospective study and may have included an insufficient number of cases. Finally, the efficacy of the antibiotic treatment was assessed on Day 7 after the onset of fever; however, there may be room for debate regarding the validity of this timing for assessing treatment effects. However, a sensitivity analysis was conducted, and consistent results were obtained when investigating the success rate of fever resolution at Days 8, 9, 10, and 11 after fever onset (data not shown). Analysis of the fluoroquinolone prophylaxis group, which may benefit from earlier administration of anti‐MRSA drugs owing to a higher incidence of Gram‐positive bacteria, is not yet available and requires further study.
In conclusion, early administration of anti‐MRSA agents was associated with a shorter duration of fever in patients with FN following allo‐HCT. Moreover, early administration of anti‐MRSA drugs may be associated with a lower incidence of Grade II–IV aGVHD in older patients, suggesting that the timing of anti‐MRSA therapy could be clinically relevant in this population. Early administration of anti‐MRSA drugs may be relevant not only to the course of FN but also to the overall post‐transplant course, including the development of aGVHD.
Author Contributions
Conceptualization and design of the study: Anna Akaogi and Junya Kanda. All the authors have made substantial contributions to the design of the work, the analysis and interpretation of the data, and the drafting or revision of the manuscript. All authors have approved the final manuscript for publication.
Funding
This work was supported in part by the JSPS KAKENHI Grant Number 24K11515 (JK) and the Takeda Science Foundation (JK).
Ethics Statement
This study was approved by the Kyoto University Ethics Committee and adhered to the principles of the Declaration of Helsinki.
Consent
Informed consent was obtained from all the patients.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Supporting Figure 1: jha270251‐sup‐0001‐figuresS1‐S4.pdf
Supporting Table 1: jha270251‐sup‐0001‐tablesS1‐S7.xlsx
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1“Prevention and Treatment of Cancer‐Related Infections Version 1.2023,” National Comprehensive Cancer Network , published June 28, 2023, https://www.nccn.org/professionals/physician_gls/pdf/infections.pdf.
- 2A. G. Freifeld , E. J. Bow , K. A. Sepkowitz , et al., “Clinical Practice Guideline for the Use of Antimicrobial Agents in Neutropenic Patients With Cancer: 2010 Update by the Infectious Diseases Society of America,” Clinical Infectious Diseases 52, no. 4 (2011): e 56–e 93, 10.1093/cid/cir 073.21258094 · doi ↗ · pubmed ↗
- 3A. J. Zimmer , E. Stohs , and J. Meza , “Bloodstream Infections in Hematologic Malignancy Patients With Fever and Neutropenia: Are Empirical Antibiotic Therapies in the United States Still Effective?” Open Forum Infectious Diseases 9, no. 7 (2022): ofac 240, 10.1093/ofid/ofac 240.35854988 PMC 9277632 · doi ↗ · pubmed ↗
- 4T. Saito , S. Yoshioka , Y. Iinuma , et al., “Effects on Spectrum and Susceptibility Patterns of Isolates Causing Bloodstream Infection by Restriction of Fluoroquinolone Prophylaxis in a Hematology–Oncology Unit,” European Journal of Clinical Microbiology & Infectious Diseases 27, no. 3 (2008): 209–216, 10.1007/s 10096-007-0428-8.18058141 · doi ↗ · pubmed ↗
- 5S.‐I. Kimura , Y. Akahoshi , H. Nakano , et al., “Antibiotic Prophylaxis in Hematopoietic Stem Cell Transplantation. A Meta‐Analysis of Randomized Controlled Trials,” Journal of Infection 69, no. 1 (2014): 13–25, 10.1016/j.jinf.2014.02.013.24583063 · doi ↗ · pubmed ↗
- 6“Common Terminology Criteria for Adverse Events Version 5.0,” National Cancer Institute , published November 27, 2017, https://ctep.cancer.gov/protocol Development/electronic_applications/ctc.htm#ctc_50.
- 7Y. Kanda , “Investigation of the Freely Available Easy‐To‐Use Software ‘EZR’ for Medical Statistics,” Bone Marrow Transplantation 48, no. 3 (2013): 452–458, 10.1038/bmt.2012.244.23208313 PMC 3590441 · doi ↗ · pubmed ↗
- 8A. Cometta , W. V. Kern , R. De Bock , et al., “Vancomycin Versus Placebo for Treating Persistent Fever in Patients With Neutropenic Cancer Receiving Piperacillin‐Tazobactam Monotherapy,” Clinical Infectious Diseases 37, no. 3 (2003): 382–389.12884163 10.1086/376637 · doi ↗ · pubmed ↗