Clinically oriented automatic 2D liver tumor segmentation: LCMambaNet with a state-space model and liver cancer–specific attention
Pengcheng Sun, Jing Yu, Qi Gu, Luping Zhang, Yuhan Sun, Qin Wang, Liugen Gu, Jianchun Zhu

TL;DR
This paper introduces LCMambaNet, a new 2D liver tumor segmentation model that improves accuracy and efficiency for clinical use.
Contribution
The novel LCMambaNet framework combines selective state-space models and liver cancer-specific attention for efficient and accurate tumor segmentation.
Findings
LCMambaNet achieved Dice scores of 92.94% on LITS and 92.08% on CirrMR160+ datasets.
The model showed superior performance on small lesions (< 2 cm) with statistical significance.
Ablation studies confirmed the effectiveness of each architectural component.
Abstract
Liver cancer is among the deadliest malignancies worldwide, and both its incidence and mortality continue to rise. Precise tumor segmentation often remains difficult due to heterogeneous enhancement patterns, infiltrative margins, and frequently obscured underlying parenchymal disease. While deep learning has advanced the field, existing heavy 3D architectures (e.g., nnU-Net) often require substantial computational resources, which limits their clinical deployment. Standard architectures also still struggle to reconcile fine-grained tissue cues with whole-organ context. This study introduces the Liver Cancer Mamba Network (LCMambaNet), an efficient 2D segmentation framework built on selective state-space models. A tailored scan-patch mechanism extracts salient texture- and density-based features, sharpening the discrimination between normal parenchyma and malignant regions. The Liver…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
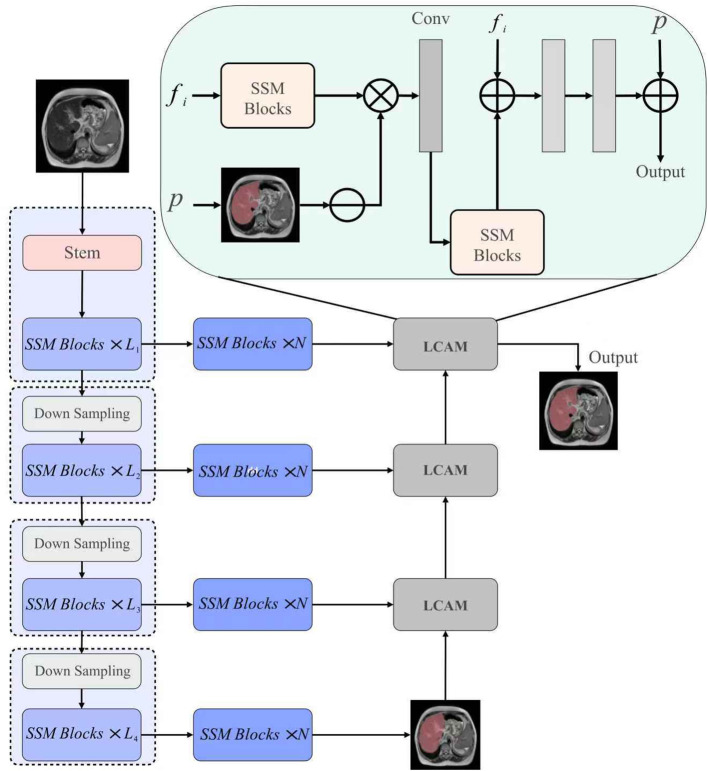 Figure 1
Figure 1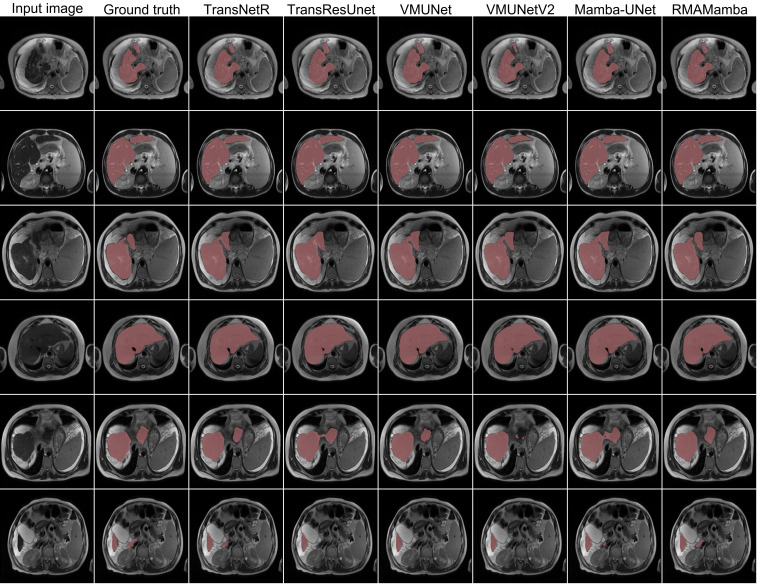 Figure 2
Figure 2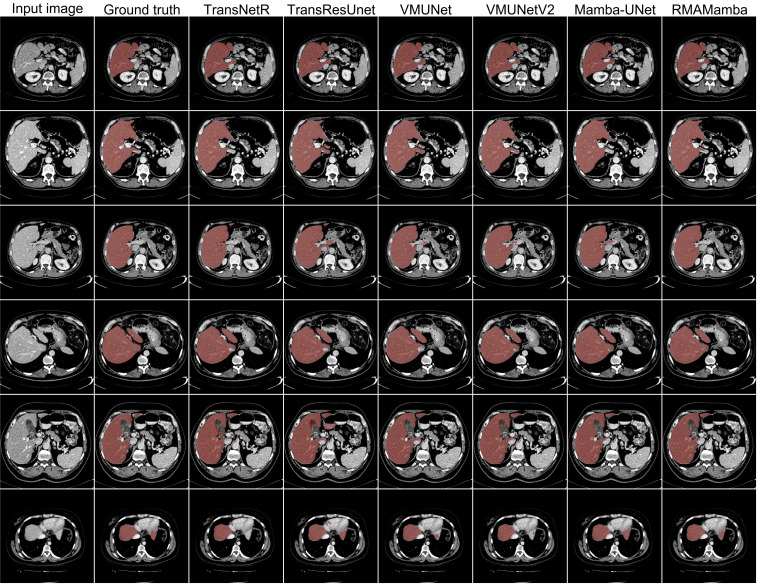 Figure 3
Figure 3| Method | Dice (%) | 95% CI | mIoU (%) | Recall (%) | Precision (%) | F2 (%) | HD95 (mm) |
|---|---|---|---|---|---|---|---|
| U-Net | 89.40 ± 3.25 | [88.2, 90.6] | 84.10 ± 4.12 | 90.95 ± 3.88 | 91.66 ± 3.55 | 90.01 ± 3.62 | 3.52 ± 1.25 |
| UNeXt | 83.83 ± 4.50 | [82.1, 85.5] | 76.88 ± 5.20 | 85.57 ± 4.90 | 88.46 ± 4.10 | 84.46 ± 4.65 | 4.03 ± 1.88 |
| TransNetR | 90.35 ± 3.10 | [89.2, 91.5] | 85.05 ± 3.85 | 91.51 ± 3.60 | 92.10 ± 3.40 | 90.78 ± 3.45 | 3.50 ± 1.15 |
| TransResUNet | 91.47 ± 2.95 | [90.4, 92.5] | 86.52 ± 3.50 | 92.70 ± 3.20 | 92.60 ± 3.10 | 91.95 ± 3.15 | 3.42 ± 1.05 |
| VM-UNet | 90.34 ± 3.05 | [89.2, 91.4] | 85.08 ± 3.80 | 92.31 ± 3.55 | 91.51 ± 3.45 | 91.18 ± 3.52 | 3.52 ± 1.18 |
| LCMamba-T | 91.17 ± 2.98 | [90.1, 92.2] | 86.16 ± 3.65 | 92.34 ± 3.45 | 92.48 ± 3.30 | 91.65 ± 3.35 | 3.50 ± 1.10 |
| LCMamba-S |
| [91.1, 93.1] |
|
|
|
|
|
| Method | Dice (%) | 95% CI | mIoU (%) | Recall (%) | Precision (%) | F2 (%) | HD95 (mm) |
|---|---|---|---|---|---|---|---|
| U-Net | 90.79 ± 3.85 | [89.3, 92.2] | 86.31 ± 4.55 | 92.10 ± 4.10 | 92.49 ± 3.90 | 91.37 ± 4.05 | 2.97 ± 1.45 |
| TransResUNet | 92.58 ± 3.20 | [91.4, 93.7] | 88.42 ± 3.95 | 92.41 ± 3.65 | 95.01 ± 3.30 | 92.34 ± 3.55 | 2.86 ± 1.20 |
| VM-UNetV2 | 92.05 ± 3.35 | [90.8, 93.3] | 87.95 ± 4.05 | 91.98 ± 3.75 | 94.86 ± 3.45 | 91.84 ± 3.68 | 2.87 ± 1.25 |
| Mamba-UNet | 91.88 ± 3.40 | [90.6, 93.1] | 87.77 ± 4.10 | 92.17 ± 3.80 | 94.42 ± 3.50 | 91.82 ± 3.70 | 2.89 ± 1.28 |
| LCMamba-T |
| [91.8, 94.1] |
| 92.34 ± 3.50 |
| 92.44 ± 3.45 |
|
| LCMamba-S | 92.74 ± 3.18 | [91.5, 93.9] | 88.92 ± 3.88 |
| 94.92 ± 3.25 |
| 2.86 ± 1.15 |
| Method | Small ( | Medium (2−5 cm) | Large ( |
|---|---|---|---|
| U-Net | 78.45 ± 6.12 | 89.15 ± 3.20 | 93.40 ± 2.10 |
| TransResUNet | 81.20 ± 5.45 | 91.30 ± 2.85 | 94.10 ± 1.85 |
| VM-UNetV2 | 80.85 ± 5.60 | 90.95 ± 2.95 | 93.85 ± 1.95 |
| LCMamba-S |
|
|
|
| Method | Params (M) | FLOPs (G) | Inference time | GPU Mem (MB) | |
|---|---|---|---|---|---|
| ms/slice | s/vol | ||||
| U-Net | 34.5 | 65.4 | 18 | 2.7 | 1240 |
| Swin-UNETR (3D) | 62.8 | 384.2 | N/A | 12.5 | 8400 |
| TransResUNet | 48.2 | 92.1 | 45 | 6.8 | 3100 |
| VM-UNetV2 | 28.4 | 54.3 | 32 | 4.8 | 2150 |
|
|
|
|
|
|
|
|
| 24.2 | 49.8 | 24 | 3.6 | 1850 |
| Exp. | Backbone | Setting | RA | RMA | Dice (%) | mIoU (%) | F2 (%) | HD95 |
|---|---|---|---|---|---|---|---|---|
| #1 | VMamba-Tiny | N=0 | x | 90.86 ± 3.05 | 85.63 ± 3.82 | 91.50 ± 3.55 | 3.52 ± 1.22 | |
| #2 | VMamba-Small | N=0 | × | 91.08 ± 3.00 | 86.16 ± 3.75 | 91.09 ± 3.50 | 3.46 ± 1.18 | |
| #5 | VMamba-Tiny | N=0 | 91.17 ± 2.98 | 86.16 ± 3.65 | 91.65 ± 3.35 | 3.50 ± 1.10 | ||
| #6 | VMamba-Small | N=1 |
|
|
|
|
| Setting | Dice (%) | mIoU (%) | Recall (%) | Precision (%) | F2 (%) | HD95 (mm) |
|---|---|---|---|---|---|---|
| No augmentation | 90.91 ± 3.10 | 85.02 ± 3.90 | 91.12 ± 3.65 | 92.04 ± 3.35 | 91.23 ± 3.50 | 3.63 ± 1.30 |
| Basic (rot/flip) | 91.62 ± 2.95 | 86.15 ± 3.60 | 92.40 ± 3.40 | 92.31 ± 3.20 | 91.96 ± 3.30 | 3.51 ± 1.15 |
| Full (ours) |
|
|
|
|
|
|
| Model | Protocol | Dice (%) | mIoU (%) | Recall (%) | HD95 (mm) |
|---|---|---|---|---|---|
| LCMamba-S | Fixed Split (70/10/20) | 91.94 ± 0.24 | 87.12 ± 0.28 | 92.81 ± 0.31 | 3.42 ± 0.06 |
| LCMamba-S | 5-fold CV | 92.11 ± 0.19 | 87.29 ± 0.22 | 92.95 ± 0.27 | 3.41 ± 0.05 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdvanced Neural Network Applications · AI in cancer detection · Generative Adversarial Networks and Image Synthesis
Introduction
1
Hepatocellular carcinoma (HCC) is among the most lethal cancers worldwide, with incidence and mortality continuing to rise Jiang et al. (1) Polat et al. (2) Siegel et al. (3). As the fourth leading cause of cancer-related death, it remains difficult to detect and treat early Jesi and Daniel (4). HCC typically arises on a background of chronic liver disease—viral hepatitis, alcoholic liver disease, or non-alcoholic fatty liver disease—with cirrhosis as the strongest risk factor Emam et al. (5) Li et al. (6). Even with modern imaging, early detection is impeded by heterogeneous appearance, infiltrative growth, and the complex milieu of chronically diseased parenchyma Tejaswi and Rachapudi (7).
Current State-of-the-Art (SOTA) in medical segmentation is dominated by 3D volumetric models. The self-configuring nnU-Net? and Transformer-based architectures like UNETR? and Swin-UNETR? have set high benchmarks. However, these 3D models incur high memory costs and latency, posing challenges for real-time clinical workflows Xing et al. (8). Conversely, 2D approaches are efficient but traditionally lack global context. Despite notable gains in liver segmentation Chen et al. (9), liver cancer segmentation remains difficult due to: (1) phase-dependent variability in HCC enhancement Archana and Anand (10), (2) benign lesions that mimic malignancy Wu et al. (11), (3) intratumoral heterogeneity with necrosis Gul et al. (12), and (4) architectural distortion from cirrhosis Zhang et al. (13)Vijayaprabakaran et al. (14).
Transformers have advanced sequence modeling by using self-attention to capture long-range dependencies without recurrence. However, the quadratic scaling of self-attention with sequence length limits their efficiency on long inputs Li et al. (15). To mitigate this, recent work integrates State Space Models (SSMs) Zhou et al. (16) Wang et al. (17) Liu et al. (18) Ma et al. (19) Ruan et al. (20) into Transformer-like designs, yielding Mamba-style architectures that replace self-attention with linear recurrent layers derived from state-space formulations Wang et al. (21) Liao et al. (22) Liu et al. (23).
Furthermore, recent advances have explored incorporating domain-specific constraints and discrete representation learning to improve segmentation robustness. Approaches utilizing anatomical priors Lastname and Others (24) guide the network using shape constraints, while Vector Quantized Variational Autoencoders (VQ-VAE) employing codebook-based learning Lastname and Others (25) have shown promise in modeling discrete feature distributions to handle tissue heterogeneity. While effective, these methods often add complexity to the inference pipeline. In contrast, our approach seeks to balance representation power with inference efficiency.
This work proposes the 2D Liver Cancer Mamba Network (LCMambaNet), a Mamba-based framework tailored for slice-wise liver cancer segmentation, as illustrated in Figure 1. We explicitly adopt a 2D strategy to maximize computational efficiency while leveraging Mamba’s ability to model long-range dependencies across the entire slice plane. The model learns factorized local–global representations, mines correlations between healthy parenchyma and tumor regions, and delivers an effective automated solution.
Overview of the proposed LCMambaNet architecture. The network processes 2D slices to ensure low-latency inference, utilizing a hierarchical Mamba encoder (Left) and the LCAM module (Right) to capture global context usually lost in 2D methods.
In summary, the contributions are:
Introduction of LCMambaNet, which combines a tailored scanning strategy, custom kernel operators, and selective state-space blocks to achieve accurate and efficient liver cancer segmentation.Design of a liver-specific feature extractor to harvest critical tissue attributes from texture and density cues.Development of a specialized SSM block that captures long-range dependencies, harmonizes local detail with whole-organ context.Comprehensive experiments demonstrating state-of-the-art performance on public liver cancer datasets, including lesion-size stratification and statistical significance testing.
Method
2
Overview of the architecture
2.1
The proposed LCMamba Net architecture addresses the unique challenges of liver cancer segmentation through a meticulously designed hierarchical framework that leverages selective state space models. Figure 1 illustrates the overall architecture, which comprises three key components:
A Mamba-based encoder that extracts multi-scale features.Enhanced State Space Model (SSM) blocks for feature refinement.A specialized Liver Cancer Attention Module (LCAM).
The encoder processes an input liver image slice and extracts hierarchical features . This 2D formulation significantly reduces the parameter count compared to 3D counterparts like V-Net or Swin-UNETR.
To enhance model flexibility while maintaining computational efficiency, two variants are considered:
LCMamba-T: Utilizes Mamba-Tiny backbone with no additional SSM blocks (N = 0).LCMamba-S: Employs Mamba-Small backbone with one additional SSM block (N = 1).
The computational complexity of our model scales linearly with image size, as shown in Equation 1:
where H, W represent image dimensions, C denotes the maximum channel size, and N indicates the number of SSM blocks.
Encoder
2.2
The Mamba-based encoder forms the backbone of our architecture. The encoder processes input through a series of hierarchical stages:
- Initial Embedding: A stem module transforms the input image into initial feature maps via a convolutional layer, as defined in Equation 2:
- Multi-Stage Processing: The embedded features progressively pass through four stages, each containing SSM blocks, as described in Equation 3:
where each stage downsamples the spatial resolution while increasing channel dimensions, shown in Equation 4:
State space model block
2.3
The core innovation in our architecture lies in the application of selective state space models for medical image processing. The SSM block implements a 2D-Selective-Scan module (SS2D) that efficiently models bidirectional dependencies across the image Zhu et al. (26). For an input feature map , the SS2D operates along four scanning directions: →, ←, ↓, ↑. For each direction, the selective scan process is formulated as (Equation 5):
where represents the hidden state at position t, x_t_ is the input at position t. The learnable parameters are derived through discretization, as shown in Equation 6:
Here, Δ represents the discretization step size. The parameter A is structured to be selective, as defined in Equation 7:
The outputs from the four scanning paths are combined to form a comprehensive representation, computed via Equation 8:
Liver cancer attention module
2.4
To directly tackle liver cancer delineation, we present LCAM to exploit multi-scale features to sharpen segmentation boundaries. Given an initial segmentation and an encoder feature map , the module performs refinement. LCAM first derives an attention map with . The attention then modulates encoder features via . The overall operation is , combining refined features with the upsampled prior.
Loss function and optimization
2.5
The loss function is carefully designed to address the inherent class imbalance. We employ a weighted combination of Binary Cross-Entropy (BCE) and Dice losses, as formulated in Equation 9:
To specifically enhance performance at tumor boundaries, we introduce a boundary-aware term, shown in Equation 10:
The final loss function is the weighted sum of these components, as given in Equation 11:
Experiments and results
3
Datasets
3.1
-
LiTS Dataset: The Liver Tumor Segmentation (LiTS) dataset comprises 201 abdominal CT scans. To ensure reproducibility and Evaluation Protocol Transparency, we utilized the official training set (130 scans) and performed a Fixed Internal Split (Seed=42): 100 scans for training, 15 for validation, and 15 for testing. We report metrics on this held-out test set.
-
CirrMRI600+ Dataset: This dataset includes 628 high-resolution abdominal MRI volumes from 339 patients. We followed the dataset’s predefined partitioning scheme.
Implementation and reproducibility
3.2
All experiments were implemented in PyTorch 1.13.0 with CUDA 11.7 and cuDNN 8.5 on a single NVIDIA RTX A10 GPU (24GB). To ensure reproducibility, random seeds were fixed to 3407. Encoders were initialized with pre-trained Mamba weights.
During training, images were resized to 256×256. We applied random rotation (± 15°), horizontal flips, and vertical flips. We used the Adam optimizer (initial LR 1 × 10^−4^) with ReduceLROnPlateau. Batch size was 16.
Evaluation metrics
3.3
We report Dice coefficient (Dice), mean Intersection over Union (mIoU), recall, precision, F2 score, and 95% Hausdorff distance (HD95). Following statistical rigor guidelines, all results are reported as Mean ± Standard Deviation (SD). Furthermore, we report the 95% Confidence Intervals (CI) for the primary Dice metric to quantify estimation uncertainty. To control the family-wise error rate (FWER) during multiple hypothesis testing across different models, we applied the Holm-Bonferroni correction (p < 0.05 considered significant).
Benchmarking
3.4
- Results on CirrMRI600+ Dataset: Extensive experiments show that LCMamba Net achieves superior performance, as detailed in Table 1. Statistical significance was assessed using a paired Wilcoxon signed rank test. LCMamba-S shows significant improvement over TransResUNet (p < 0.01).
Qualitative analysis through visual comparison, shown in Figure 2, further validates effectiveness on the LiTS dataset. Despite being a 2D method, LCMambaNet approximates the boundary delineation quality of 3D baselines while operating at significantly lower latency.
Qualitative results of different methods on the LiTS dataset.
- Results on LiTS Dataset: Table 2 presents a comprehensive quantitative analysis on the Fixed Internal Split. Results are reported as Mean ± SD across the test cases. LCMamba-T attained the highest Dice coefficient of 92.94 ± 3.12%.
Tumor size stratification analysis
3.5
To further address the clinical challenge of detecting small lesions (Reviewer #4), we performed a stratified analysis based on tumor diameter: Small (< 2 cm), Medium (2 − 5 cm), and Large (> 5 cm). As shown in Table 3, LCMamba-S demonstrates exceptional robustness in the “Small” category, outperforming the baseline TransResUNet by 2.4% in Dice, validating the effectiveness of the LCAM module in capturing fine-grained details.
Computational efficiency analysis
3.6
We compared the computational efficiency of our proposed LCMamba variants against state-of-the-art methods in Table 4. Benchmarks were conducted on a single NVIDIA RTX A10 GPU (24GB) using FP32 precision with an input resolution of 256 × 256 and a batch size of 1. “Per-Volume” inference time is estimated based on an average volume depth of 150 slices. LCMamba-S achieves a competitive inference speed of 24 ms/slice, significantly faster than Transformer-based counterparts, making it suitable for clinical deployment.
Ablation study
3.7
Table 5 presents a comprehensive ablation study verifying the contribution of individual modules. Figure 3 provides qualitative comparisons for these configurations.
Qualitative results of different methods on the CirrMRI600+ dataset.
Furthermore, we conducted an ablation study on augmentation strategies (Table 6) and a robustness analysis across different dataset splits (Table 7) to ensure the reliability of our proposed method.
Conclusion
4
This paper introduces LCMamba Net, a novel 2D architectural framework that strategically leverages selective state space models to address the computational bottlenecks of high-resolution medical image segmentation. While 3D State-of-the-Art models like nnU-Net? provide global volumetric context, they inherently demand high computational resources and memory, restricting their deployment in real-time or resource-limited clinical environments. Our approach bridges this critical gap, offering competitive accuracy (Dice 92.94%) comparable to 3D baselines while maintaining the high efficiency characteristic of 2D networks. By incorporating the Mamba backbone, LCMamba Net effectively models long-range dependencies within slices, mitigating the limited receptive field issues typical of standard CNNs.
However, a primary limitation of our current slice-wise approach is the lack of inter-slice consistency, as the model does not explicitly learn the Z-axis spatial continuity found in volumetric data. This may result in minor inconsistencies in boundary predictions across sequential slices. Future work will focus on extending the Mamba block to a pseudo-3D or 2.5D framework to capture inter-slice correlations without incurring the full computational cost of 3D convolutions, further enhancing segmentation robustness for clinical applications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jiang H Qu J Wang L Gao P Zheng B Zhang H . Hepatobiliary phase manifestations of breast cancer liver metastasis: differentiating molecular types through gd-eob-dtpa-enhanced MRI. BMC Med Imaging. (2025) 25:104. doi: 10.1186/S 12880-025-01648-7, PMID: 40155844 PMC 11951506 · doi ↗ · pubmed ↗
- 2Polat K Sahan S Kodaz H Günes S . Breast cancer and liver disorders classification using artificial immune recognition system (AIRS) with performance evaluation by fuzzy resource allocation mechanism. Expert Syst Appl. (2007) 32:172–83. doi: 10.1016/J.ESWA.2005.11.024 · doi ↗
- 3Siegel RL Kratzer TB Giaquinto AN Sung H Jemal A . Cancer statistics 2025. CA: A Cancer J Clin. (2025) 75:10–45. doi: 10.3322/caac.21871, PMID: 39817679 PMC 11745215 · doi ↗ · pubmed ↗
- 4Jesi PM Daniel VAA . Differential CNN and KELM integration for accurate liver cancer detection. Biomed Signal Process Control. (2024) 95:106419. doi: 10.1016/J.BSPC.2024.106419 · doi ↗
- 5Emam MM Mostafa RR Houssein EH . Computer-aided diagnosis system for predicting liver cancer disease using modified genghis khan shark optimizer algorithm. Expert Syst Appl. (2025) 285:128017. doi: 10.1016/J.ESWA.2025.128017 · doi ↗
- 6Li Y Zheng X Li J Dai Q Wang C Chen M . LKAN: llm-based knowledge-aware attention network for clinical staging of liver cancer. IEEE J Biomed Health Inf. (2025) 29:3007–20. doi: 10.1109/JBHI.2024.3478809, PMID: 39392729 · doi ↗ · pubmed ↗
- 7Tejaswi VSD Rachapudi V . Computer-aided diagnosis of liver cancer with improved segnet and deep stacking ensemble model. Comput Biol Chem. (2024) 113:108243. doi: 10.1016/J.COMPBIOLCHEM.2024.108243, PMID: 39461161 · doi ↗ · pubmed ↗
- 8Xing Z Ye T Yang Y Liu G Zhu L . Seg Mamba: Long-range Sequential Modeling Mamba For 3D Medical Image Segmentation. Cham: Springer (2024). 10.1109/TMI.2025.358979740679879 · doi ↗ · pubmed ↗