World’s Largest Tonsillolith Removal: A Case Report With Literature Review of Large Tonsil Stones on Record
Anukaran Mahajan, Anubhuti Dhanuka, Karunesh Gupta

TL;DR
This case report describes the successful removal of the largest recorded tonsil stone, which was initially mistaken for an abscess.
Contribution
The paper presents the first documented case of a tonsillolith measuring 5.2 × 2.5 × 2.5 cm being successfully removed.
Findings
A massive tonsillolith measuring 5.2 × 2.5 × 2.5 cm was successfully removed surgically.
The tonsillolith was initially mistaken for a peritonsillar abscess.
This case represents the largest tonsillolith ever successfully removed.
Abstract
Tonsil stones or tonsilloliths are mineralised concretions in the crypts of palatine tonsils. They are usually small and asymptomatic. Sometimes, they can be recurrent, large in size and produce symptoms like a sense of foreign body in throat, mild pain and heaviness in throat and halitosis. In such cases, a surgical intervention may be required for permanent cure. We came across one such patient with massive tonsillolith which mimicked a peritonsillar abscess initially. Eventually, the large tonsillolith was surgically removed in toto. It measured 5.2 × 2.5 × 2.5 cm which makes it the largest tonsillar stone ever to be successfully removed till date.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
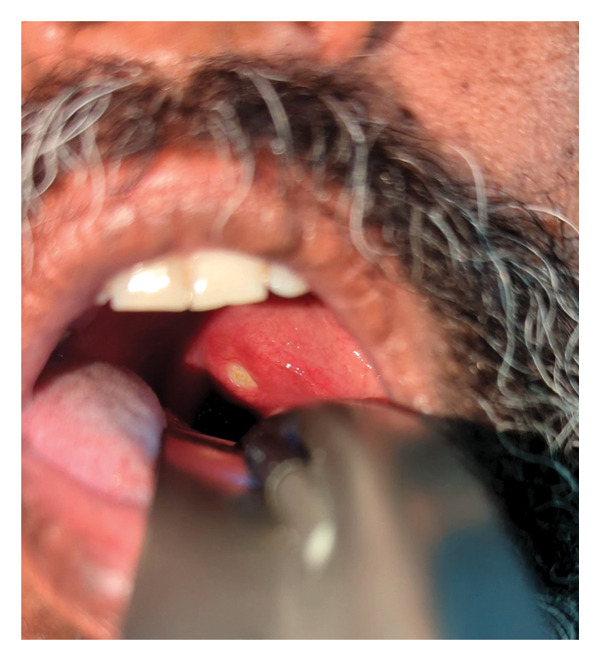 FIGURE 1
FIGURE 1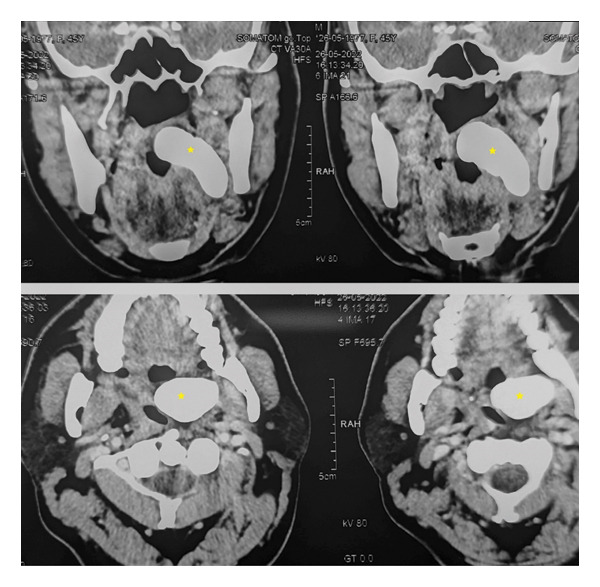 FIGURE 2
FIGURE 2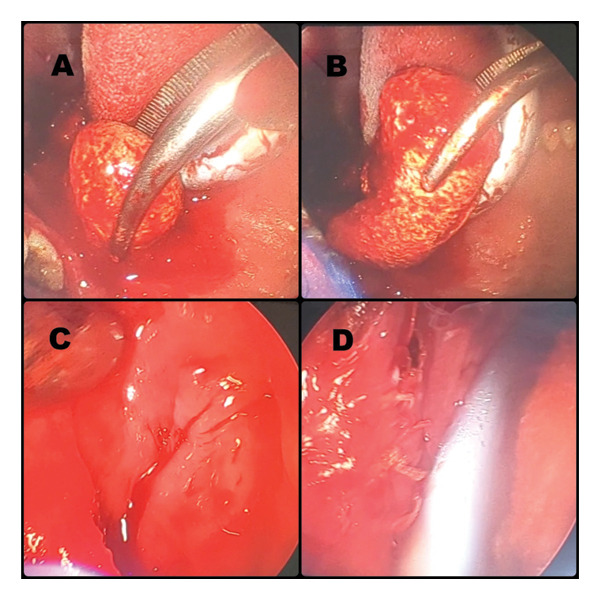 FIGURE 3
FIGURE 3 FIGURE 4
FIGURE 4| Author | Year | Age/sex | Location | Weight | Size | Signs and symptoms | Treatment |
|---|---|---|---|---|---|---|---|
| Swain [ | 1920 | 56/F | Right | NA | Large | Pain, dysphagia, enlarged tender lymph nodes, recurrent stones | NR |
| Woodman [ | 1920/21 | 64/M | Right | 6.2 g | NA | ‘Stone in the mouth’, abscess, neck sinus, recurrent stones | NR |
| Goodman [ | 1930 | 20/M | Left | 3.3 g | 2.1 ∗ 1.5 ∗ 1.54 cm | Sore throat | NR |
| Rubin [ | 1936 | 32/M | Right | 24.7 g | 3.7 ∗ 2.8 cm | Pain, lump in throat, TB | NR |
| Bugge [ | 1949 | 60/M | Bilateral | 3.5 g | NA | Recurrent tonsillitis | NR |
| 45/M | Bilateral | 4.5 g | NA | Sore throat | NR | ||
| Clarke [ | 1954 | 35/M | Right | 13.3 g | NA | Neck sinus, lump in throat, pain, halitosis, pneumonia | NR |
| Harding [ | 1962 | 57/F | Right | NA | 1 ∗ 1 cm, 0.5 cm | Sore throat | NR |
| Mishenkin [ | 1965 | 53/F | Palatine | 2.7 g | 3.4 ∗ 0.1 cm | Recurrent tonsillitis, pharyngeal heaviness | NR |
| 17/F | Palatine | 3.3 g | 2.5 ∗ 0.1 cm | Recurrent tonsillitis | NR | ||
| 33/M | Palatine | 37 g | 2.3 ∗ 2 cm | Pharyngeal heaviness | Prior tonsillectomy (at age 30) | ||
| Hiranandani [ | 1967 | 65/F | Right | 42 g | 2.5 ∗ 3 cm | Recurrent throat pain | Right tonsillectomy |
| Shrimali and Bhatia [ | 1972 | 63/F | Left | 32 g | 2.5 ∗ 2 cm | Throat pain, odynophagia | Enucleation under GA |
| Dale and Wing [ | 1974 | 54/F | Right | 0.56 g | 2 ∗ 1 cm | Halitosis | NR |
| Ramanjaneyulu [ | 1974 | 64/M | Right | NA | Large | Throat pain, cervical lymphadenopathy | Patient refused surgery |
| Samant and Gupta [ | 1975 | 45/M | Right | 30 g | NA | Painless slow growing swelling, history of right peritonsillar abscess | |
| 16/M | Right | 25 g | NA | Slow growing throat swelling, history of quinsy | |||
| Gapany‐Gapanavicius [ | 1976 | 26/M | Right | 6.7 g | 3.2 ∗ 2.1 ∗ 1.7 cm | Recurrent sore throat, swelling, fever | NR |
| Hoffman [ | 1978 | NA | Right | NA | NA | Intermittent swelling | NR |
| Kulinich [ | 1979 | 50/F | Right | NA | NA | Enlarged submandibular glands | NR |
| Elidan et al. [ | 1980 | 25/F | Right | 5.2 g | 2.5 ∗ 1.8 ∗ 1.5 cm | Recurrent throat infection, pain radiating to right ear | NR |
| Marshall and Irwin [ | 1981 | NA | Left | NA | NA | Incidental finding | NR |
| Cooper et al. [ | 1983 | 77/F | Left | 8 g | 4 ∗ 2 ∗ 2 cm | Chronic oral infection, multiple episodes of pneumonia, right tonsillectomy and recurrent intermittent infection of left submandibular gland with abscess formation and Wharton’s duct calculi | Enucleation (prior tonsillectomy) |
| Padmanathan et al. [ | 1984 | 40/M | Left | Large stone: 22.6 g, small stone: 300 mg | 4 ∗ 3 cm | History of recurrent swelling in the left submandibular region, throat pain | |
| Gadgil [ | 1984 | 28/M | Right | NA | NA | Throat pain, dysphagia and recurrent pharyngitis | NR |
| Hadi and Samara [ | 1985 | 28/M | Left | 8 g | 2 ∗ 1.5 ∗ 1 cm | Odynophagia and foreign body sensation in the throat | |
| Westmore and Hupp [ | 1988 | 63/M | Left | NA | 1.5 ∗ 1.5 ∗ 3 cm | Emphysema and general ill health; died of pulmonary embolus 2 days after examination | Enucleation |
| Heppt [ | 1989 | 77/M | Right | 7 g | NA | Mass in right tonsillar fossa | NR |
| Cerny and Bekarak [ | 1990 | 10/F | Tonsillar fossa | 0.84 g | 2.6 ∗ 0.4 cm | Asymptomatic | NR |
| Kimura et al. [ | 1993 | 27/M | Left | 8.5 g | 3 ∗ 2.6 ∗ 1.6 cm | Recurrent pharyngitis, tonsillitis, tonsillar abscess | Spontaneous expulsion and tonsillectomy |
| Vera Llao et al. [ | 1995 | 43/F | Right | NA | NA | Odynophagia | |
| Castellano and Marcolli [ | 1996 | 68/F | Left | 14 g | 2.8 ∗ 2.3 ∗ 2.1 cm | Lymphadenopathy left mandible | Enucleation under LA |
| Jones [ | 1996 | 70/M | Right | NA | 1‐2 mm | Mass in right tonsillar fossa | Enucleation |
| el‐Sherif and Shembesh [ | 1997 | 24/M | Right | 8.2 g | 3.2 ∗ 2 ∗ 1.5 cm | History of recurrent throat infections (4 years duration) and throat pain | |
| Revel et al. [ | 1998 | 68/M | Right | NA | NA | Odynophagia and right otalgia | Right tonsillectomy |
| Modrzynski et al. [ | 2001 | 70/M | Right | NA | 4.1 ∗ 2.1 ∗ 1.9 cm | Pharyngitis and recurrent tonsillitis, recurrent throat infection | |
| Neshat et al. [ | 2001 | 69/M | Left | NA | 1.2 ∗ 1.6 cm | Asymptomatic | Enucleation under LA |
| Cogolludo Perez et al. [ | 2002 | 69/F | Right | NA | 3 ∗ 2 ∗ 2.3 cm | Dysphagia | Tonsillectomy |
| Sezer et al. [ | 2003 | 31/F | Left | NA | 1.5 ∗ 1.5 ∗ 1.3 cm | Right pericoronitis with pain and swelling; incidental X‐ray finding | |
| Ram et al. [ | 2003 | 57/F | Right | NA | NA | Asymptomatic; incidental X‐ray finding; squamous cell carcinoma of right buccal mucosa with pain | |
| Silvestre‐Donat et al. [ | 2005 | 55/F | Right | NA | 2.5 ∗ 1.5 cm | Dysphagia | Enucleation |
| Thakur et al. [ | 2008 | 12/F | Left | NA | 4.2 ∗ 3.6 ∗ 2.1 cm | Odynophagia, recurrent sore throat | Enucleation with tonsillectomy under GA |
| Gangaraj and Maruthi [ | 2013 | 56/F | Right | NA | 2 ∗ 1.5 cm | Foreign body sensation in throat, halitosis | Enucleation |
| Neha Salaria et al. [ | 2016 | 35/F | Right | NA | 2.6 ∗ 2.5 ∗ 2.3 cm | Recurrent episodes of tonsillitis since 1 year. There was associated difficulty in swallowing, along with a history of halitosis | Enucleation |
| Alfayez A et al. [ | 2018 | 45/M | Left | NA | 3.1 ∗ 2.3 cm | Recurrent sore throat and tonsillitis | Enucleation with tonsillectomy |
| Khetani et al. [ | 2020 | 24/F | Left | NA | 2 ∗ 1.17 cm | Foreign body sensation in throat, ear pain | Enucleation |
| Vijayan et al. [ | 2020 | 7/M | Bilateral | NA | 1 ∗ 2 ∗ 2.3 cm on right Small on left | Sore throat, odynophagia and foreign body sensation in throat, recurrent tonsillitis | Tonsillectomy |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOropharyngeal Anatomy and Pathologies · Head and Neck Anomalies · Oral and Maxillofacial Pathology
1. Introduction
Tonsil stones or tonsilloliths are calcifications of the debris in the tonsils, almost exclusively affecting palatine tonsils. Palatine tonsils have crypts and clefts which often entrap food particles, dead cells and bacteria. Over time, this debris can get mineralised into whitish concretions and is called as tonsil stones or tonsilloliths.
Tonsilloliths are usually small and recurrent and can be unilateral or bilateral. These are often asymptomatic. Symptoms, if present, can be one or more of the following:
- -Throat irritation/discomfort.
- -Foreign body sensation in throat.
- -Mild pain or heaviness in throat with mild difficulty in swallowing food.
- -Halitosis.
Tonsilloliths usually do not require any treatment except routine warm saline gargles and maintaining oral hygiene. In some cases, surgery in the form of tonsillectomy and/or enucleation of tonsil stone may be required where symptoms are persistent and troublesome to the patient.
As mentioned earlier, tonsil stones are small in size (less than 0.5 cm). Rarely, these tonsil stones may present as large masses of size > 1 cm. Various authors, all over the world, have reported tonsilloliths of sizes ranging from 1 to 4 cm [1–44].
We also present a case of a large unilateral tonsillolith of size 5.2 × 2.5 × 2.5 cm which was surgically removed. On reviewing the literature, we found it to be the largest tonsil stone ever to be surgically removed till date.
2. Case Report
We present a case of a 48‐year‐old male patient who presented with complaints of mild pain and heaviness in the left side of throat. It was accompanied by mild dysphagia and some foreign body sensation. On examining the oral cavity, a bulge was seen in the left peritonsillar region. A preliminary diagnosis of peritonsillitis was made, and the patient was prescribed a short course of antibiotics and follow‐up. The patient did not show up on his scheduled follow‐up date, only to revisit after 4 months with persisting complaints of mild pain, heaviness and dysphagia. Oral cavity examination again revealed a left peritonsillar bulge, but this time, it was accompanied by an apparent pus point over it (Figure 1). Although there were no constitutional symptoms, a working diagnosis of peritonsillar abscess was made and antibiotics were started. Transoral aspiration was attempted, but the needle could not penetrate into the so thought abscess pocket and was instead encountering a stony‐hard lesion. Computed tomography (CT) scan was advised to further ascertain the pathology. To our surprise, CT revealed a large calcified mass lesion in the peritonsillar region (Figure 2). A final diagnosis of a large tonsillolith was made. Retrospectively, it fitted all the symptoms and examination findings. After counselling the patient, he was taken into the operating room. Tonsillolith was successfully removed in toto through transoral route using a peritonsillar incision (Figures 3 and 4). The removed specimen was sent for histopathology. The healthy tonsil was left undisturbed as it was the first episode, and the authors considered it prudent to give the tonsils a chance to heal in the most physiological manner. The incision site was sutured with absorbable sutures, and oral diet was started the next day, much to the symptomatic relief of the patient. Histopathology revealed bacterial colonies with entrapped neutrophils and dystrophic calcification (Figures 5(a) and 5(b)). A microbial culture was not performed during histopathological examination. The patient is under our regular follow‐up and disease free for 1 year now.
Bulge in the left peritonsillar region with an apparent ‘pus point’. In reality, the tonsillolith is mimicking a peritonsillar abscess.
CT scan showing a large tonsillolith.
Intraoperative images. Tonsillolith being delivered out (A, B). Healthy underlying cavity where tonsillolith was situated (C). Sutured peritonsillar incision using absorbable sutures (D).
Excised tonsillolith specimen.
FIGURE FIGURE 5Histopathology of the removed tonsillolith specimen. (a) Histopathology of calcification (marked with green arrow). (b) Histopathology of bacterial colonies (green arrow) and neutrophils (orange arrow).(a)(b)
3. Discussion
Tonsil stones or tonsilloliths are mineralised concretions in the crypts of palatine tonsils. Small tonsilloliths usually do not require any surgical intervention. Warm saline gargles, especially done post‐meals, are enough to wash away small stones. For larger tonsilloliths, or, when the symptoms are persistent, a surgical option can alleviate the disease [8–10, 19, 23, 26, 28, 29, 31, 33, 34, 37–43]. Our patient had an enormous tonsillolith which needed a transoral enucleation procedure.
Tonsilloliths are usually asymptomatic and may be diagnosed as an incidental finding [18, 23, 25, 33, 35, 36]. Rarely, they can present with one or more of the following symptoms: foreign body sensation in throat, mild pain, mild dysphagia, throat heaviness, sore throat and halitosis [1–14, 17, 19–22, 24, 26, 27, 30, 31, 34, 37–43]. Most of these symptoms are recurrent. Our patient presented with similar complaints of mild throat pain and heaviness, mild dysphagia and foreign body sensation. Multiple symptoms could be owing to the large size of the tonsillolith (5.2 × 2.5 × 2.5 cm).
Over the years, various authors have described large tonsil stones. We did an extensive review of literature and have enumerated the large tonsilloliths in Table 1.
It was evident from the review of literature that this was the largest tonsillolith to be ever removed successfully till date.
A few articles have (incorrectly) mentioned a tonsillolith of size 14.5 cm by Rubin in 1936 [44]. But the original publication by Rubin mentions a tonsillolith of size 1.5 inch × 1 inch only [4]. It was clear that the size was mistakenly cited by subsequent articles.
Funding
No external funding was received for this article.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Swain H. I. , Recurrent Calculus of the Tonsil—Report of a Case, Annals of Otology, Rhinology & Laryngology. (1920) 29, no. 1, 73–78, 10.1177/000348942002900107, 2-s 2.0-3242690909. · doi ↗
- 2Woodman G. S. , A Case of Tonsillar Calculus of Unusual Size, British Journal of Surgery. (1920) 8, no. 31, 375–376, 10.1002/bjs.1800083117, 2-s 2.0-84979103184. · doi ↗
- 3Goodman H. S. , Case Report—a Large Tonsillolith, The Laryngoscope. (1930) 40, no. 4, 10.1288/00005537-193004000-00007, 2-s 2.0-84978545856. · doi ↗
- 4Rubin H. , An Unusually Large Calculus of the Tonsil, The Laryngoscope. (1936) 46, no. 21, 376–379, 10.1288/00005537-193605000-00003. · doi ↗
- 5Bugge S. and Gjessing O. R. , Kjemisk Og Strukturell Undersokelse Av to Tifelle Tonsillesten, Med Sammenlignende Kjemisk Og Strukturell Undersokelse Av Tonsillesten og Tansten, Nor Tannlaegegoren Tid. (1949) 59, 53–56.
- 6Clarke P. R. , Tonsillar Calculi, The Lancet. (May 1954) 263, no. 6822, 10.1016/s 0140-6736(54)92159-5, 2-s 2.0-3242656644.13164339 · doi ↗ · pubmed ↗
- 7Harding J. A. , Tonsilloliths, Practitioner. (1962) 188.
- 8Nv M. and Al S. , Kamni Nebnykh Mindalin I Prichiny Ikh Obrazovaniia [Calculi of Palatine Tonsils and Causes of Their Formation], Vestnik Otorinolaringologii. (March-April 1965) 27, 110–112, Russian. PMID: 14307957.14307957 · pubmed ↗