Successful Use of Argon Plasma Coagulation in the Treatment of Multiple Recurrent Lower Tract Papillomatosis: A Case Report
Samer El Rayess, Ahmad Doklaigah, Wassim Hamadeh, Behnaz Saadieh, Hani Shahin

TL;DR
A 51-year-old man with rare lower respiratory tract papillomatosis was successfully treated with argon plasma coagulation, remaining symptom-free after 5 months.
Contribution
Demonstrates the successful use of argon plasma coagulation for treating a rare form of papillomatosis with no laryngeal involvement or HPV infection.
Findings
The patient remained lesion-free and symptom-free for 5 months after treatment.
Argon plasma coagulation was effective and safe for multiple lesions in critical lower respiratory tract areas.
Treatment avoided complications like perforation or cartilage damage.
Abstract
Recurrent Respiratory Papillomatosis is a rare, benign papillomatous growth of the bronchial epithelium which occurs in 18 patients in a million. Due to the rareness of the disease, no general treatment consensus exists. Surgical debulking or simple excision via bronchoscopy are the most used therapeutic approaches with adjunct medical therapy, such as intra‐lesional antivirals and interferon therapy, in case of recurring disease. We present the case of a 51‐year‐old man who presented with recurrent respiratory papillomatosis. This case made the approach more challenging as we were dealing with widespread isolated lower respiratory tract involvement (lower trachea and main bronchi) sparing the larynx and vocal cords without evidence of HPV virus infection. A decision was made to intervene with bronchoscopic electro snare and argon plasma coagulation (APC) as few reported cases…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
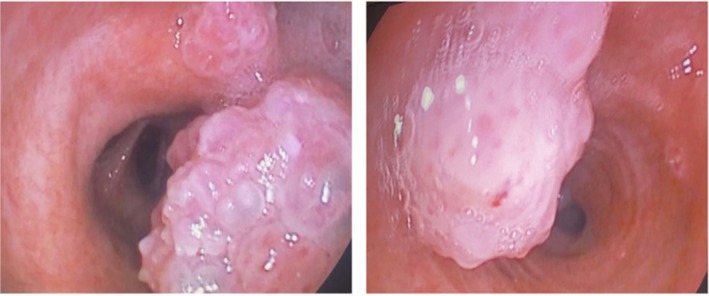 FIGURE 1
FIGURE 1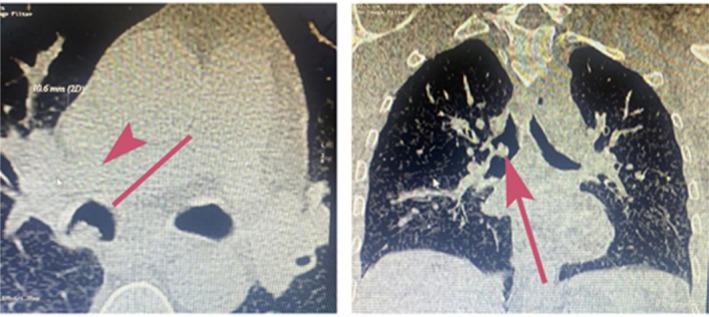 FIGURE 2
FIGURE 2 FIGURE 3
FIGURE 3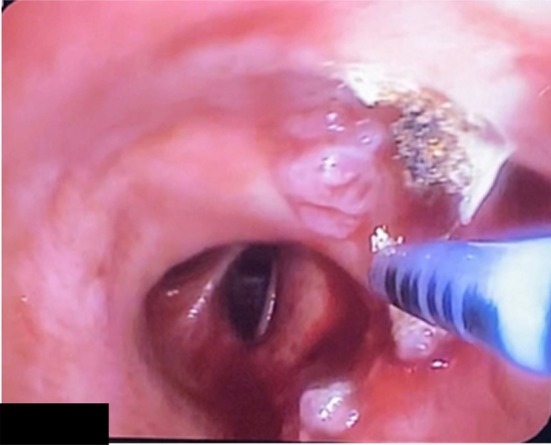 FIGURE 4
FIGURE 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCervical Cancer and HPV Research · Voice and Speech Disorders · Head and Neck Cancer Studies
Introduction
1
Recurrent respiratory papillomatosis (RRP) is a benign papillomatous growth of the bronchial epithelium, rare in adults, with an incidence of 18 patients in a million [1, 2, 3, 4]. It is thought to be due to Human Papilloma Virus (HPV) infection in about 90% of the cases [1]. Isolated lesions in the bronchial tree are not reported as frequently as isolated upper airway papilloma or concomitant laryngeal involvement with tracheal polyps.
Due to its rarity, and up to this date, no treatment guidelines have been established. Herein, we report the successful use of Argon Plasma Coagulation (APC) in treating a patient with recurrent respiratory papillomatosis.
Case Report
2
A 51‐year‐old man, complaining of hemoptysis, presented to our clinic. He is a heavy smoker (30 packs year). He didn't report significant weight loss over the past months, anorexia, or night sweats. His past medical and surgical histories were unremarkable. He mentioned that a bronchoscopy was done 1 year ago to investigate the cause of hemoptysis. At that time, multiple biopsies were taken from endobronchial lesions (Figure 1). Pathology revealed squamous papilloma with moderate dysplasia. No further actions were taken at that time. Bronchoscopy repeated after 1 year when he presented to our clinic showed an increase in the number of lesions. Removal of the polyps was done in a two‐step procedure in the Operation Room (Each intervention lasted approximately 45 min and was performed 1 week apart) under general anaesthesia using the APC technique and thermal ablation. Flexible bronchoscopy was used. The polyps were snared around the peduncle and detached from the bronchial wall; then APC was applied in a continuous manner onto the tissue with around 40–50 watts of energy escalating depending on the lesion, until clearance of the airway from any visualised polyps (Figures 2, 3, 4). No adverse effect occurred after 5 months.
The Intra‐bronchial lesions visualised by flexible bronchoscopy.
Computed tomography (CT scan) showing a lesion in the right bronchus (red arrow).
Hot snare around the peduncle.
APC probe over the region.
Discussion
3
RRP is a benign progressive growing tumour which affects mainly upper airways being focal or diffuse, with various sites of involvement, sizes and rate of growth [1]. Thus, it has an unpredictable course and non‐specific symptoms and signs. Despite the benign nature of the tumours, it carries a high morbidity when it comes to malignant transformation in 3%–4% within 10 years of diagnosis, or when it complicates recurrent respiratory infections owing to mechanical obstructions or bronchiectasis and spread throughout the respiratory tract [1]. Though only a few are idiopathic, it is believed that most respiratory papilloma are attributed to HPV, a virus known not only for driving recurrent disease but also for its potential to undergo malignant transformation in a subset of patients. Hence, they tend to occur with bimodal age distribution; in paediatrics age its transmission is via vertical and in adults via reactivation of latent HPV carriers or sexual transmission, as thought to be in our case. So far, there is no conventional treatment for RRP, with debulking or excision via bronchoscopy being the mainstay therapy and diagnostic tool. Adjunct medical options are required in around 20% of the cases when the disease tends to recur rapidly, spread distantly, causing airway obstructive symptoms or when frequent bronchoscopies are required [5]. Aside from the absence of definitive cure of the disease, what made our case more challenging is the unusual widespread of multiple isolated lower respiratory tract involvement (lower trachea and main bronchi) sparing the larynx and vocal cords without evidence of HPV virus infection. Secondly, our patient was already in a relapse with more spread given he had undergone bronchoscopic resection 1 year prior to presentation. This, in turn, rendered him a candidate for the use of adjunct therapies (rapid recurrence with airway compromise) like antiviral and interferon. However, a decision was made to intervene with bronchoscopic electrocauterization and APC due to the unavailability of the adjunctive therapies. This decision was supported firstly in the literature, by a few reported cases emphasising the effectiveness of RRPs treated with APCs and secondly, owing to the wish of our patient who refused to take the quadrivalent vaccine of HPV, which was proven to decrease papilloma growth rate and consequently the number of bronchoscopies. All in all, multiple factors made APC an optimal therapy option for our patient. First, its safety and low risk of perforation/cartilage damage (no contact) along with efficiency when it comes to multiple lesions with critical sites through the bronchi. Second, avoidance of systemic side effects of the anti‐viral and bevacizumab beside the cost effectiveness. Third, APC, when compared to other modalities of bronchoscopy like laser, brachytherapy or cryotherapy, was found to be of the most evidence according to similar published case reports. Finally, APC use in RRP, which was first described in the literature in a few reports, shows promises for a cure, as it has shown success in preventing relapse of the disease [1, 2, 3, 4, 5].
In conclusion, bronchoscopic Argon Plasma Coagulation shows promising success as a treatment option for Reccurent Respiratory papillomatosis, with minimal post‐operative complication and a 5 month symptom‐free period in our patient. Furthermore, when compared to other modalities such as bronchoscopic laser, brachytherapy or cryotherapy, APC was found to be the most effective at reducing the rate of relapse according to similarly published case reports [1, 2, 3, 4, 5].
Consent
The patient provided written informed consent for his case to be published using the form provided by the journal.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1K. Harris and M. Chalhoub , “Tracheal Papillomatosis: What Do We Know So Far?,” Chronic Respiratory Disease 8, no. 4 (2011): 233–235, 10.1177/1479972311416381.21971565 · doi ↗ · pubmed ↗
- 2J. L. Wong , S. T. Tie , J. Lee , et al., “A Case of Recurrent Respiratory Papillomatosis Successfully Removed via Endoscopic Argon Plasma Coagulation (APC) With no Evidence of Recurrence,” Pub Med 69, no. 4 (2014): 195–196.25500852 · pubmed ↗
- 3M. L. Ramos , R. Ueha , T. Goto , N. Matsumoto , and K. Kondo , “Pathogenesis of Recurrent Respiratory Papillomatosis and Potential Novel Treatment Strategies,” Auris Nasus Larynx 52, no. 4 (2025): 381–387, 10.1016/j.anl.2025.05.011.40516276 · doi ↗ · pubmed ↗
- 4S. Murono , “Current Treatment Options for Recurrent Respiratory Papillomatosis: A Narrative Review,” Auris Nasus Larynx 52, no. 4 (2025): 307–313, 10.1016/j.anl.2025.04.014.40339519 · doi ↗ · pubmed ↗
- 5W. Bergler , M. Hönig , K. Götte , G. Petroianu , and K. Hörmann , “Treatment of Recurrent Respiratory Papillomatosis With Argon Plasma Coagulation,” Journal of Laryngology and Otology 111, no. 4 (1997): 381–384, 10.1017/s 0022215100137387.9176627 · doi ↗ · pubmed ↗