A bibliometric and visual analysis of colorectal cancer-diabetes comorbidity
Junyu Long, Xuewei Shi, Yandong Huang, Qingyang Bai, Kai Feng

TL;DR
This paper analyzes global research trends on colorectal cancer and diabetes comorbidity, identifying growth in studies and key research themes like metformin's potential and molecular mechanisms.
Contribution
The study provides a bibliometric and visual analysis of CRC-DM comorbidity research, highlighting emerging thematic foci and collaborative networks.
Findings
Annual publications on CRC-DM comorbidity increased significantly after 2005.
The U.S. and China are leading contributors, with institutions like Harvard and Birmingham Women’s Hospital being prominent.
Key research clusters include metformin’s therapeutic potential and diabetes-associated centrosome amplification.
Abstract
Colorectal cancer (CRC), a leading cause of global cancer-related mortality, exhibits a complex bidirectional relationship with diabetes mellitus (DM). Epidemiological evidence indicates that DM significantly increases the risk of CRC, while CRC progression may exacerbate diabetic complications; however, the underlying mechanisms remain incompletely understood. This study aimed to conduct a bibliometric analysis of the literature on COLORECTAL CANCER-DIABETES comorbidity to identify research trends, collaborative networks, and emerging thematic foci. We performed a comprehensive search in the Web of Science Core Collection (WoSCC) database to retrieve relevant literature. Using analytical and visualization tools, including CiteSpace and VOSviewer, we examined publication trends, major contributing countries and institutions, collaboration networks, and keyword evolution to map the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
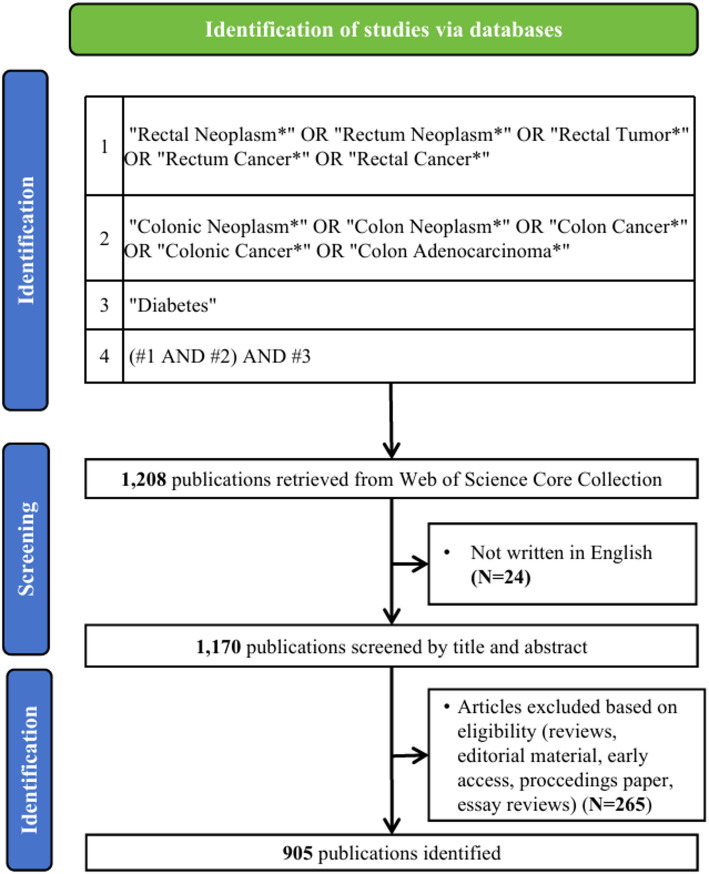 Figure 1
Figure 1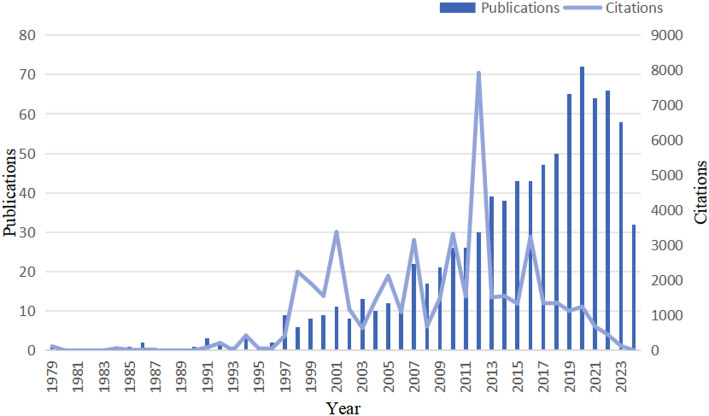 Figure 2
Figure 2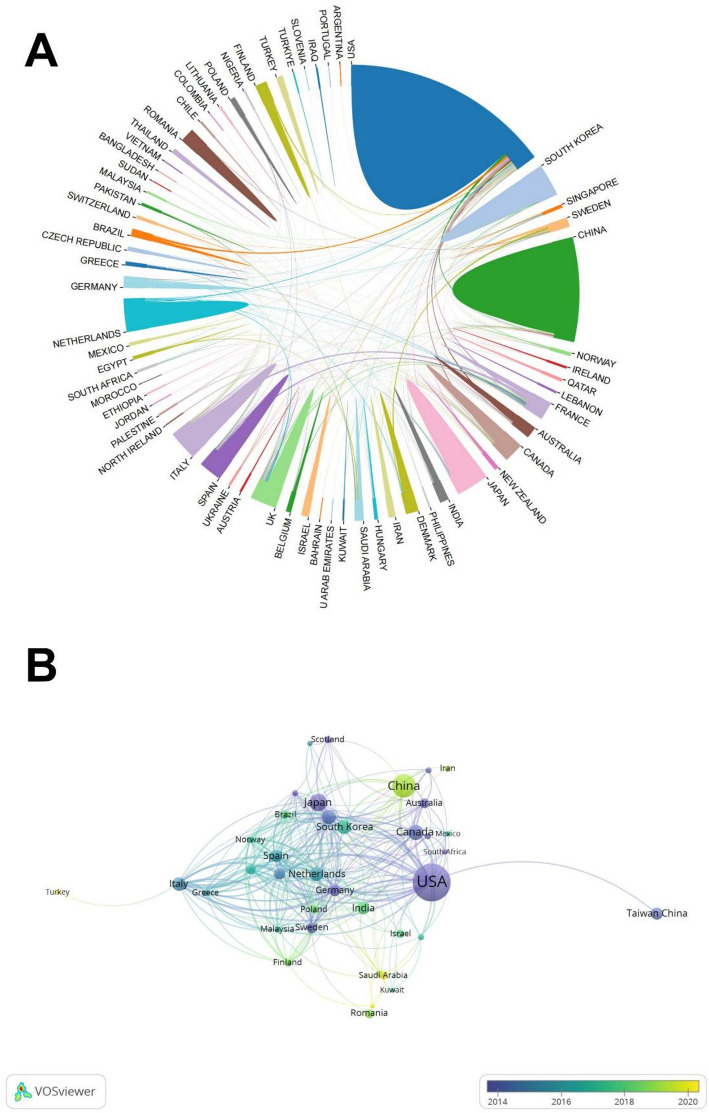 Figure 3
Figure 3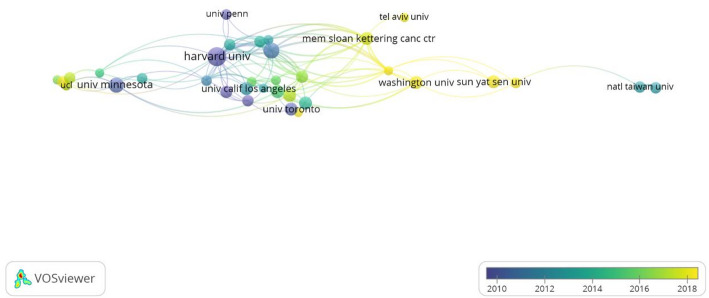 Figure 4
Figure 4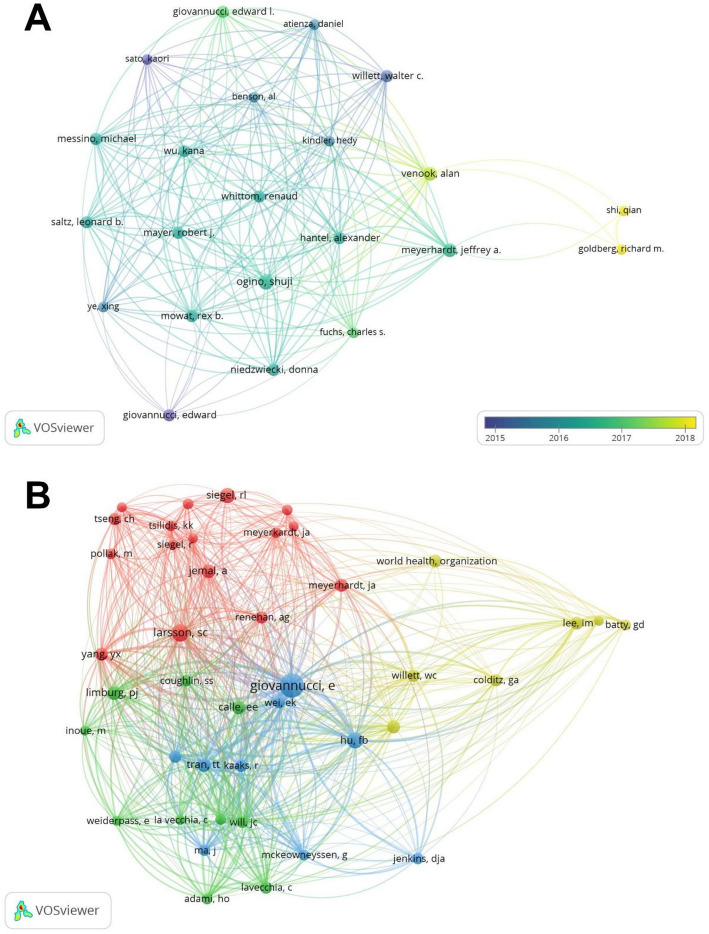 Figure 5
Figure 5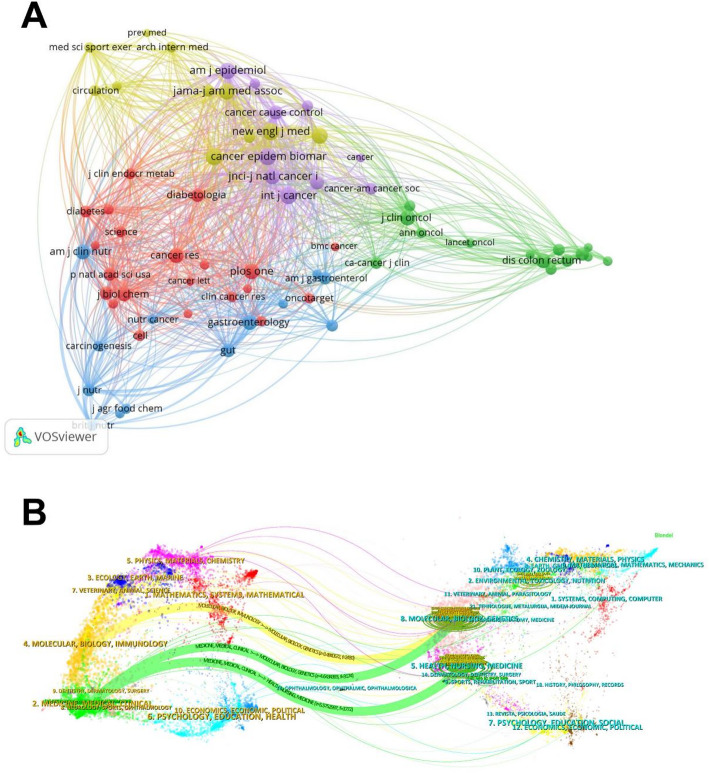 Figure 6
Figure 6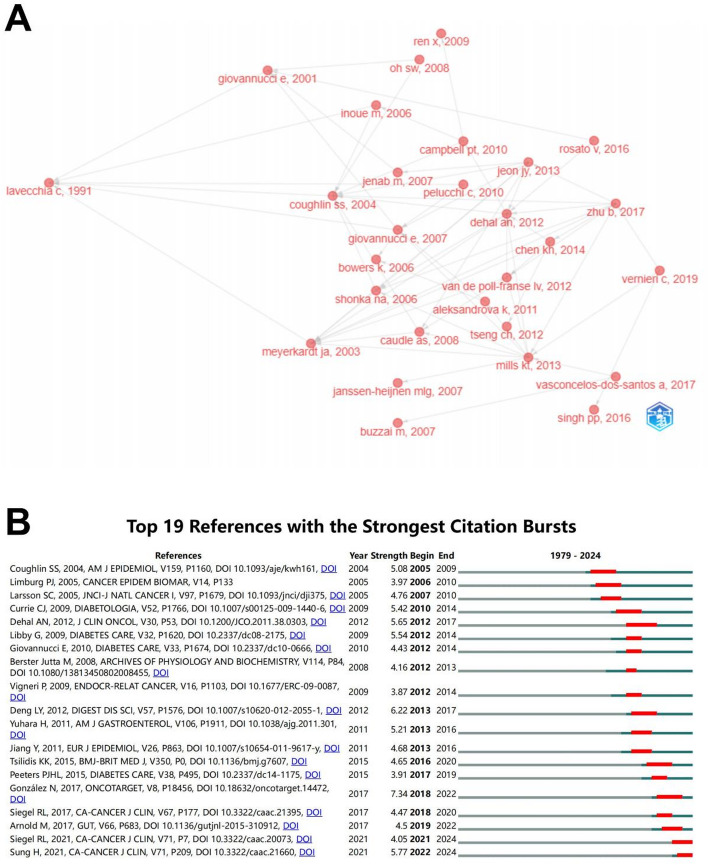 Figure 7
Figure 7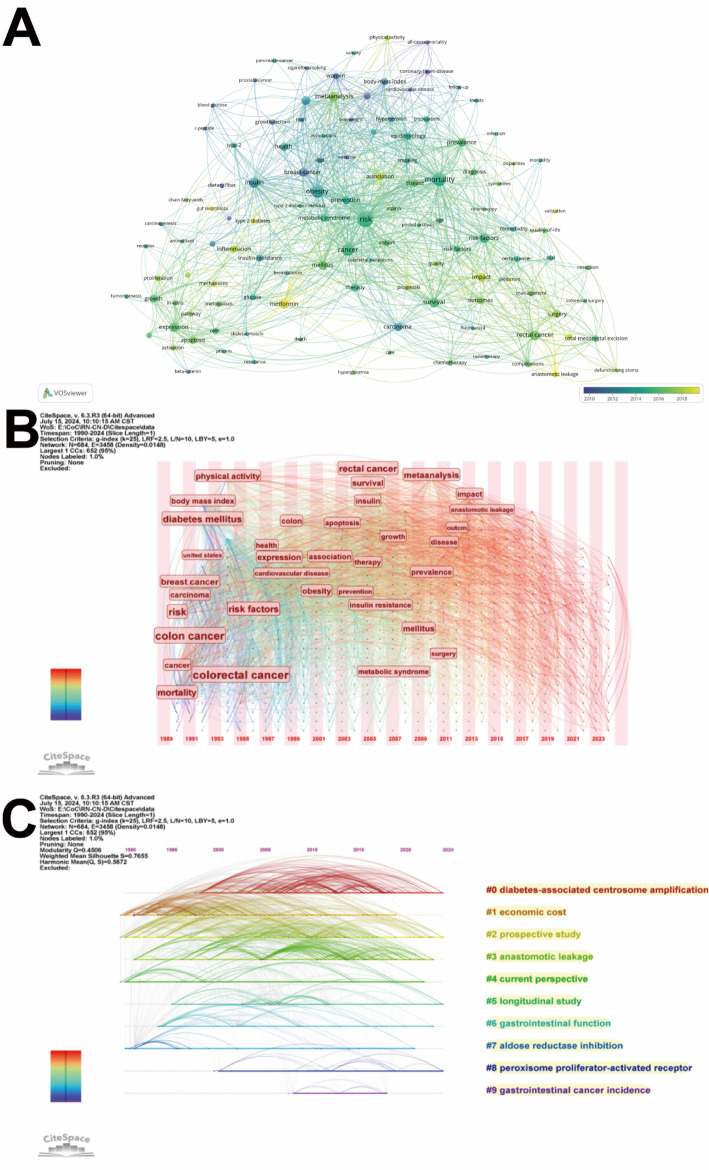 Figure 8
Figure 8Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMetabolism, Diabetes, and Cancer · Cancer, Hypoxia, and Metabolism · Pancreatic and Hepatic Oncology Research
Introduction
Diabetes mellitus (DM) and colorectal cancer (CRC) are both diseases with high treatment costs that place a heavy financial burden on individuals, society, and the nation [1, 2]. Diabetes is a common chronic disease in the population, mainly characterised by insulin secretion disorders, insulin utilisation disorders or a combination of both deficiencies, and is mainly classified into type 1 diabetes, type 2 diabetes mellitus (T2DM) and gestational diabetes, with T2DM accounting for 90% of the total number of people suffering from the disease [3]. Worldwide, diabetes is one of the leading causes of death among adults, and its prevalence and incidence continue to rise. The 9th edition of the International Diabetes Federation (IDF) Atlas shows that the number of people with diabetes is expected to increase to 700 million globally by 2045 [4]. Most CRC cases evolve from adenomatous polyps [5]. Previous studies have suggested that adenomatous polyps may evolve as neoplastic precursor lesions from cancer stem cells or stem cell-like cells located at the base of the colonic crypts [6]. CRC was estimated to be the third most common cause of morbidity (9.6 per cent) and the second most common cause of mortality (9.3 per cent) globally in 2022 [7]. The 8th edition of the American Joint Committee on Cancer (AJCC) cancer staging manual suggests that the relative survival rate for patients with stage IV CRC is only about 40% [8]. Previous EUROCARE studies on cancer survival analysis in European countries have shown that CRC patients aged 60–69 had an average five-year cumulative relative survival rate of 40% and that the prognosis becomes poorer with increasing age at diagnosis [9].
A complex bidirectional relationship exists between diabetes and CRC. Diabetes is one of the risk factors for CRC, and CRC may also contribute to the progression of diabetes. Most diabetic patients are associated with an increased incidence of various solid tumours, such as pancreatic cancer, breast cancer, cancers of the hepatobiliary system and CRC. There is a positive correlation between the risk of CRC in patients with diabetes compared to those without diabetes [10, 11]. In addition, studies have shown that CRC patients have a significantly higher risk of developing DM within 5 years of diagnosis compared to non-CRC patients [12]. Shared risk factors for both disorders include insulin resistance (IR), hyperglycemia, and hyperinsulinemia [11, 13, 14]. Prolonged hyperglycemia can seriously damage the function of human organs, and the worse the daily glycaemic control, the more serious the damage to the target organs [15].
Currently, there is limited bibliometric research output focusing on CRC from the perspective of diabetes, with a notable lack of targeted studies in this area, which warrants further investigation. In 1969, Alan Pritchard defined bibliometrics as a discipline that employs mathematical and statistical methods to analyse scholarly publications [16]. As an emerging discipline with extensive application potential, particularly in the field of medical science, the use of CiteSpace enables quantitative analysis of research progress in target domains, thereby providing robust data support for future studies and policy formulation.
This study conducted a bibliometric analysis of research outputs on colorectal cancer-diabetes comorbidity from 1990 to 2024, identified key research hotspots in the field, and provided novel perspectives for subsequent investigations.
Materials and methods
Data sources
In the literature search, initially, we selected one of the three major databases, the Web of Science Core Collection (WoSCC), Scopus and Google Scholar, which are the main sources of citation data. Google Scholar provides richer citation results among the three, but its data sources are not all specialised academic journals. Scopus is a newcomer in the field of bibliometric research, but its data content is relatively new. Although WoSCC is not perfect, it is still regarded as the gold standard in the field of bibliometrics [16]. Meanwhile, the data analysed by CiteSpace is based on WoSCC data, and the data from other databases need to be converted to WoS data format before they can be analysed, so we finally chose the WoS database as the retrieval source.
On July 10, 2024, we performed a comprehensive literature search in WoSCC database. The primary search terms were “Rectal Neoplasm”, “Colonic Neoplasm” and “Diabetes”, with language restricted to English and publication type limited to Articles. The detailed search strategy is provided in Supplementary Table S1. To avoid the impact of database updates, all search results were downloaded within the same day in multiple formats, including plain text, Excel, BibTex, and tab-delimited files. Ultimately, 905 records were identified for analysis. The overall research workflow is schematically illustrated in Fig. 1.
Fig. 1. Publications screening flowchart
Data analysis and visualization
The retrieved data were imported into CiteSpace (version 6.3.R3), VOSviewer (version 1.6.20), the bibliometrix package in R (version 4.4.0), Scimago Graphica, and the Bibliometric Analysis Online Platform (https://bibliometric.com/) to perform analysis of published studies and create visual mapping diagrams. VOSviewer enables knowledge mapping visualisation of large-scale literature data through co-authorship analysis, co-occurrence analysis, and co-citation analysis, representing authors, journals, and related entities [17–19]. CiteSpace was employed to conduct country collaboration mapping, journal co-authorship analysis, reference co-citation analysis, and keyword clustering, thereby identifying developmental trajectories and emerging trends within the research domain [19, 20]. We conducted burst detection analysis [21] on the references to identify emerging academic trends and novel disciplinary developments, enabling the projection of frontier research directions and potential hotspots [22]. The keyword timelines [23] delineated temporal ranges of clustered research hotspots, revealing interconnections between distinct thematic concentrations, thereby mapping the evolutionary trajectory of research focuses since the inception of CRC comorbidity studies. Subsequent time-zone maps of keywords demonstrated their chronological distribution patterns, with keyword emergence and evolution elucidating shifts in research themes and trends. An international collaboration network was constructed using the Bibliometric Analysis Online Platform. The historiograph mapping of references was generated using the bibliometrix package in R, which visualizes inter-citation relationships among publications and delineates knowledge dissemination trajectories within the research domain.
Results
Analysis of annual publications and trends
This study conducted a comprehensive analysis of 905 publications meeting predefined inclusion criteria. Figure 2 displays their annual distribution, revealing a steady increase starting from the late 1990s with accelerated growth after 2005, peaking around 2020. Citation counts peaked in 2012, indicating potential high-impact outputs during this period, followed by a moderate decline in citations after 2018.
Fig. 2. Annual publications and citations
Analysis of the trend of countries/regions
The 905 publications originated from 72 countries/regions and 1,605 institutions. The United States (308 articles; average citations per article 98.98; centrality 0.32) dominated in publication volume, followed by China (122 articles; average citations per article 15.66; centrality 0.06), but the latter demonstrated relatively lower citation impact and centrality. New Zealand (40 articles; average citations per article 114.75) exhibited the highest citations per article among the top 10 productive countries, succeeded by the United States and the United Kingdom (Table 1). In our research, the cooperative relationship between countries reveals that the United States and other countries/regions cooperate most closely (Fig. 3A and B).
Fig. 3A International collaboration network. Automatically removes isolated nodes that do not have cooperative relationships with other countries. B Temporal overlay network map of international co-authorship
Table 1. Top 10 countries/regions in terms of number and centrality of publications related to research on colorectal cancer-diabetes comorbidityRankPublicationsCountry/regionAverage citationsRankCentralityCountry/regionAverage citations1308United States98.9810.32United States98.982122China15.6620.16United Kingdom15.66366Japan29.7930.13Canada57.58452Canada57.5840.10Saudi Arabia11.29546England76.0450.08France116.55645South Korea26.4060.08Malaysia61.22740Netherlands114.7570.07Italy49.85839Italy49.8580.06Germany110.86933Taiwan China35.7690.06China15.661032Spain72.56100.06Spain72.56
Analysis of institutions
The analysis revealed less frequent inter-institutional collaborations compared to international collaborations, with Harvard University and the Brigham & Women’s Hospital occupying central positions in the network (Fig. 4). This phenomenon may be linked to the prominent scholar Edward Giovannucci, who has affiliations with both institutions. The majority of the top 10 institutions by publication volume were located within the United States (Table 2). Notably, Harvard University ranked first with 28 relevant publications, demonstrating leadership in both total citations and average citations per publication.
Fig. 4. Institution collaboration network diagram
Table 2. Top 10 institutions by publication volume related to research on colorectal cancer-diabetes comorbidityRankOrganizationCountryPublicationsTotal citationsAverage citations1Harvard UnivUnited States2812,052430.432Brigham & Womens HospUnited States194643244.373Univ MinnesotaUnited States181883104.614Univ Calif Los AngelesUnited States132061158.545Univ QueenslandAustralia132332179.386Univ UtahUnited States1334326.387Mayo ClinUnited States1249641.338Mem Sloan Kettering Canc CtrUnited States1242535.429Sun Yat Sen UnivChina1225921.5810Univ TorontoCanada121360113.33
Analysis of authors
In past studies, a total of 5389 researchers have contributed in the field of colorectal cancer-diabetes comorbidity. The top three authors with the most publications were Ogino, Shuji (n = 6); Meyerhardt, Jeffrey A. (n = 5); and Venook, Alan (n = 5). The top three most cited authors were Giovannucci, Edward (n = 666); Ogino, Shuji (n = 406); and Willett, Walter C. (n = 262) (Table 3). We used VOSviewer to generate an author collaboration network map in this research field, revealing that Shi, Qian, and Goldberg, Richard M., have maintained active collaborative partnerships in recent years (Fig. 5A). The co-citation network analysis identified Giovannucci, Edward as occupying the central hub position within the author network (Fig. 5B).
Fig. 5A Authors collaboration diagram. B Cited author co-occurrence map, different colours in (B) distinguish different clusters, and the same colour indicates similarity of studies
Table 3. Top 10 authors in terms of publications and citations related to colorectal cancer-diabetes comorbidityRankAuthors (rank by publications)PublicationsAverage citationsRankAuthors (rank by citations)Citations1Ogino, Shuji667.66671Giovannucci, Edward6662Meyerhardt, Jeffrey A.541.42Ogino, Shuji4063Venook, Alan537.43Willett, Walter C.2624Giovannucci, Edward4166.54Giovannucci, Edward L.2415Giovannucci, Edward L.460.255Meyerhardt, Jeffrey A.2076Hantel, Alexander4466Venook, Alan1877Willett, Walter C.465.57Hantel, Alexander1848Messino, Michael4468Mayer, Robert J.1849Mowat, Rex B.4469Messino, Michael18410Niedzwiecki, Donna44610Mowat, Rex B.184
Analysis of journals and subjects
A total of 513 journals have published articles related to A total of 513 journals have published articles related to colorectal cancer-diabetes comorbidity. PLOS ONE demonstrated the highest publication output (25 publications, IF = 2.9), followed by the INTERNATIONAL JOURNAL OF COLORECTAL DISEASE ranking second (14 publications, IF = 2.5). Interestingly, the most prolific journals were not necessarily the most cited, with PLOS ONE at the bottom of the citation rankings. THE LANCET received the highest citation count (6,785 citations, IF = 98.4). Notably, nearly half of the top-cited journals were classified in the Q1 JCR quartile, indicating substantial academic value within this research field (Table 4). The journal co-citation network (Fig. 6A) and dual-map overlay diagram (Fig. 6B) collectively visualise the predominant citation pathways between citing journals and cited journals in this field. The three most prominent coloured paths illustrate citation relationships where journals in the Medicine, Medical, Clinical fields reference publications from both the Health, Nursing, Medicine and Molecular, Biology, Genetics fields, followed by citations from Molecular, Biology, Immunology journals to Molecular, Biology, Genetics literature. This pattern highlights interdisciplinary convergence within the field, demonstrating that modern medical research is increasingly integrating knowledge across multiple specialised disciplines.
Fig. 6A Journal co-citation network. Distinct clusters are differentiated by colour coding, with identical colours indicating similarity in research focus areas. B Journal dual-map overlay diagram
Table 4. Top 10 journals in terms of publications and citations related to colorectal cancer-diabetes comorbidityRankTop 10 most productive journalsTop 10 most–cited journalsJournalsProductionsJCRIF (2023)JournalsAverage citationsCitationsJCRIF (2023)1PloS One25Q32.9Lancet1696.256785Q198.42International Journal Of Colorectal Disease14Q32.5American Journal Of Clinical Nutrition313.51881Q16.53Cancer Epidemiology Biomarkers & Prevention11Q33.7JNCI-Journal Of The National Cancer Institute298.251193Q199.04Diseases Of The Colon & Rectum10Q23.2Journal Of Nutrition248.41242Q33.75Cancer Causes & Control10Q42.2American Journal Of Epidemiology205.42861438Q256Scientific Reports10Q23.8Journal Of Clinical Oncology145.71431020Q142.17Clinical Gastroenterology And Hepatology9Q111.6Clinical Gastroenterology And Hepatology84.1111757Q111.68American Journal Of Epidemiology7Q25.0Cancer Epidemiology Biomarkers & Prevention72792Q33.79Journal Of Clinical Oncology7Q142.1Diseases Of The Colon & Rectum70700Q23.210Cancer7Q26.1Plos One41.241031Q32.9
Analysis of articles and references
To explore changes in the content of relevant studies over time, we analysed the historical direct citation network of colorectal cancer-diabetes comorbidity references (Fig. 7A and Supplementary Table S2). Figure 7B shows the top 19 references with the strongest citation bursts. Among them, Nieves González et al.’s review “2017 update on the relationship between diabetes and CRC: epidemiology, potential molecular mechanisms and therapeutic implications” published in ONCOTARGET (Strength = 7.34) was identified as the reference with the strongest citation burst. And the two most recent high-burst references were both cancer statistical data reports. Table 5 listed the top 10 highly cited references. “Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy”, published in Lancet in 2012, was cited 5,268 times [24].
Fig. 7A Historical direct citation network. B Top 19 references with the strongest citation bursts
Table 5. Top 10 references in terms of citations related to the research on colorectal cancer-diabetes comorbidityRankTitleCitationYearJournalJCRIF (2023)1Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy52682012LancetQ198.42Lack of exercise is a major cause of chronic diseases14682012Compr PhysiolQ24.23Prebiotic effects: metabolic and health benefits14302010Br J NutrQ33.04The economic burden of physical inactivity: a global analysis of major non-communicable diseases12392016LancetQ198.45Impact of overweight on the risk of developing common chronic diseases during a 10-year period11262001Arch Intern Med--6Current estimates of the economic cost of obesity in the United States8441998Obes Res--7The relation between different dimensions of alcohol consumption and burden of disease: an overview7852010AddictionQ15.28Systemic treatment with the antidiabetic drug metformin selectively impairs p53-deficient tumor cell growth7692007Cancer ResQ112.59Diabetes mellitus and risk of colorectal cancer: a meta-analysis7622005J Natl Cancer InstQ19.910Physical activity and risk of breast cancer, colon cancer, diabetes, ischemic heart disease, and ischemic stroke events: systematic review and dose-response meta-analysis for the Global Burden of Disease Study 20137432016BMJQ193.6
Analysis of keywords
The keyword co-occurrence network with temporal overlay, generated using VOSviewer, visualises both high-frequency keywords and newly emerged terms in recent years (Fig. 8A). To mitigate visualization bias caused by excessive frequency dominance, the terms “colon cancer,” “rectal cancer,” and “diabetes” were excluded from this analysis due to their disproportionately high occurrence rates in the dataset. The emergence of new keywords since 2018, including “metformin”, “anastomotic leakage”, “gut microbiota”, and “inflammation”, demonstrates a growing research focus on therapeutic prognosis and molecular biological mechanisms in colorectal cancer-diabetes comorbidity. The keyword time zone map produced by Citespace reveals the variation of high-frequency keywords over time (Fig. 8B). The keyword timeline map clearly shows the changes in each research hotspot over the time horizon (Fig. 8C). The timeline map structure included the X-axis representing the publication year and the Y-axis corresponding to the keyword cluster names. The keyword co-occurrence network analysis employing the Log-Likelihood Ratio (LLR) algorithm yielded a modularity (Q) > 0.3, indicating statistically significant clustering, and a silhouette (S) index > 0.7, confirming robust cluster configuration [25]. Our dataset demonstrated clustering metrics of Q = 0.4506 and S = 0.7655, aggregating 10 thematic clusters. We observe that in the recent studies mainly focusing on “#0 diabetes-associated centrosome amplification” (Cluster 0), while “#1 economic cost” (Cluster 1), “#2 prospective study” (Cluster 2), and “#3 anastomotic leakage” (Cluster 3) have remained prominent research directions since the 1990s.
Fig. 8A Keyword co-occurrence network with temporal overlay. B Keyword time zone map. C Keyword timeline map
Discussion
Research landscape and collaborative networks
To our knowledge, this study represents the first bibliometric analysis in the field of colorectal cancer-diabetes comorbidity, providing essential reference data for researchers intending to explore this field. Since 2005, the number of publications on colorectal cancer-diabetes comorbidity began to trend upward each year, with a peak of about 70 publications in 2020. Citations have likewise been on the rise overall. Beginning in the late 1990s, there were several more significant spikes in citations. In 2010, a consensus report from a joint conference in the field of oncology and diabetes stated that T2DM is a risk factor for breast cancer, CRC, and many other site-specific tumours [26]. The global trend in the quantity and impact of publications and citations on colorectal cancer and diabetes has followed a marked upward trajectory, reflecting growing academic interest and the increasing relevance of this research area.
At the national level, both the United States and China show stronger preferences for international collaboration in colorectal cancer-diabetes comorbidity research. China demonstrates remarkable publication volume and recent research activity in this field, making substantial contributions. Over the past 20 years, China has gradually established chronic disease management frameworks and enhanced its universal health insurance system [27, 28]. Specialized diabetes and cancer surveillance and registration databases have been implemented across all regions. The improvement of these medical systems reveals that China has the basis for evaluating the geographical differences of colorectal cancer diabetes complications, and can carry out multi center research on the mechanism of disease progression in the future.
The top 10 institutions by publication volume - about 80% belong to North America. Harvard University is the most widely published institution in this field, maintaining close collaborations with the Brigham & Women’s Hospital. The cooperation among these global high-level research institutions can effectively promote knowledge exchange and accelerate the output of innovative achievements in this field by sharing their research findings. Therefore, strengthening the cooperation between institutions is very important for the future development of this field. Professor Edward Giovannucci, holding joint appointments at both institutions, has the highest total citations of 666, with an average citation of 166.5, and has pioneered the field of cancer prevention by pointing out that dietary and lifestyle factors greatly influence tumorigenesis. Diet-influenced insulin, insulin-like growth factor-1 (IGF-1) and inflammatory factors can induce tumour development. Insulin is also a mitogen for tumour cell growth in vitro, which induces activation of the proto-oncogene ras and sustained activation of the MAPK pathway, ultimately contributing to colorectal carcinogenesis [29]. This reveals that exploring dietary differences via diabetes to initiate CRC is a valuable direction for future research.
This field demonstrates robust interdisciplinary integration, primarily spanning medicine, molecular biology, and clinical practice while intersecting with computer science, mathematics, physics, socioeconomics, and education sciences. The current research environment encourages participation from non-biomedical disciplines to promote interdisciplinary collaboration to continuously improve the diverse academic framework.
Emerging thematic clusters and their research implications
Keyword clustering analysis identified three prominent and evolving research frontiers, each presenting distinct mechanistic questions and clinical translation opportunities. Diabetes-associated centrosome amplification (CA), anastomotic leakage (AL), and metformin have gained significant attention in recent years and have revealed key areas for future research. Diabetes-associated centrosome amplification has emerged as the most intensively investigated focus in the colorectal cancer–diabetes comorbidity field since 2000, indicating novel mechanistic breakthroughs in pathogenesis elucidation. The sustained academic attention on anastomotic leakage highlights researchers’ extensive clinical trial investigations into postoperative complications among patients with colorectal cancer–diabetes comorbidity. Since 2018, research interest in metformin has increased significantly, reflecting its dual therapeutic potential in glycaemic regulation and modulation of neoplastic pathways.
Diabetes-associated centrosome amplification: a mechanistic frontier
Cluster #0 underscores “diabetes-associated centrosome amplification (CA)” as a novel and intense research focus. Theodor Boveri first postulated the potential tumorigenic effects of CA [30]. Genetic modification in cellular and animal models has provided compelling evidence demonstrating a causal relationship between CA and both tumorigenesis and metastatic progression [31–34]. Taking T2DM as an example, it was found not only to increase the risk of CRC incidence and metastasis rates [26], but also to induce CA in cancer-susceptible epithelial cells (e.g., intestinal polyps) and established colorectal carcinoma cells [35]. In vitro experimentation demonstrates that chronic exposure of non-neoplastic colonic epithelium to advanced glycation end products (AGEs) initiates tumorigenesis in immunocompromised murine models—an oncogenic process effectively abrogated through pharmacological inhibition or genetic silencing of CA-associated signalling pathways [35, 36]. However, critical knowledge gaps persist: the upstream triggers within the diabetic environment (e.g., specific AGEs, oxidative stress species) are not fully defined; the causal role of CA in diabetes-promoted CRC progression in vivo requires further validation; and the translational potential of CA as a biomarker for early detection or as a therapeutic target remains unexplored. Future research should: (i) employ multi-omics approaches to delineate the complete signaling cascade from hyperglycemia to CA; (ii) investigate the clinical utility of CA assessment in polyps or liquid biopsies from diabetic patients for risk stratification.
Anastomotic leakage in colorectal cancer-diabetes patients: a clinical challenge
While chemotherapeutic agents, immunotherapies, and molecular-targeted drugs have demonstrated unprecedented progress in CRC, radical surgical resection maintains its gold-standard status for early-stage CRC cases meeting R0 criteria (tumour-free margin ≥ 1 mm histologically confirmed). Standardised surgical protocols for colorectal malignancies, including radical colectomy (RC), low anterior resection (LAR) for rectal cancer, and intersphincteric resection (ISR), necessarily require the implementation of precision anastomotic techniques - encompassing end-to-end, end-to-side, and side-to-side configurations. AL is one of the serious complications that can occur after gastrointestinal surgery, which can have a significant negative impact on the survival and quality of life of postoperative patients [37, 38]. Prolonged hyperglycemia will result in delayed wound healing, and AL is about three times more likely to occur in patients with T2DM than in those without T2DM [39, 40]. Fibroblasts and endothelial cells constitute the primary cellular components of granulation tissue [41], with fibroblasts mediating wound contraction through matrix deposition [41, 42], while endothelial cells facilitate angiogenesis during the proliferative phase of healing [43, 44]. Hyperglycemia amplifies intracellular oxidative stress by activating the classical AGE-RAGE axis [45] and through atypical interactions between 3-deoxyglucosone (3-DG) and integrins alpha-1/beta-1 (α1β1) [46]. Reactive oxygen species (ROS) generated in mitochondria stimulate multiple downstream signalling pathways, including p38/MAPK, Forkhead box protein O1 (FOXO1), and nuclear factor-kappa B (NF-κB) [47–49]. This cascade triggers inflammatory responses and promotes cellular senescence and apoptosis. The ensuing inflammatory response is accompanied by M1 macrophage polarization, which impairs fibroblasts and inhibits their ability to secrete extracellular matrix (ECM) [50]. Concurrently, the presence of ROS and proinflammatory cytokines coincides with increased expression of matrix metalloproteinases (MMPs)—a family of zinc-dependent proteolytic enzymes capable of degrading protein components within the ECM [51, 52]. When ECM levels persistently fall below the threshold required for wound healing, fibroblast migration, anchorage, and proliferation become significantly impaired [53]. In addition, hyperglycemia impairs the angiogenic function of endothelial cells through ROS-mediated endothelial nitric oxide synthase (e-NOS) inhibition [54–56], activation of the AGE-RAGE axis [57], and release of pro-inflammatory factors [58]. Diabetic wounds are characterized by a chronic low-grade inflammatory state, insufficient ECM deposition, aberrant angiogenesis, and impaired contractile function (reduced α-smooth muscle actin (α-SMA) expression) [59]. Elevated levels of tumour necrosis factor-α (TNF-α) and reduced transforming growth factor-β1 (TGF-β1) contribute to an imbalance in repair signalling, promoting apoptosis and increased protease activity [59]. These complex pathophysiological processes affect the formation of granulation tissue, which is the key factor of AL after colorectal cancer surgery. Despite this understanding, translational gaps hinder clinical improvement: perioperative glycemic management protocols are not standardized for CRC surgery; reliable predictive biomarkers for AL risk in diabetic patients are lacking; and targeted interventions to improve wound healing in this cohort are underdeveloped. Future studies must prioritize: (i) prospective trials to optimize perioperative glucose control strategies; (ii) discovery and validation of immune-metabolic biomarkers—such as specific MMPs and cytokine profiles—predictive of AL; (iii) development of novel adjunctive therapies, including targeted antioxidants and growth factor applications, to enhance anastomotic healing in patients with diabetes.
Metformin in colorectal cancer-diabetes comorbidity: therapeutic promise and uncertainty
Metformin, the first-line oral antihyperglycemic agent for T2DM, exerts its therapeutic effects through mitochondrial respiratory chain complex I/IV inhibition. This bioenergetic interference elevates cellular AMP/ATP ratios, subsequently activating lysosomal AMP-activated protein kinase (AMPK) signalling cascades that coordinate hepatic gluconeogenesis suppression and peripheral glucose uptake enhancement [60]. Moreover, its potential cancer-preventive and anti-neoplastic effects have garnered increasing attention in the field of CRC [61]. Current evidence reveals two interconnected mechanistic aspects: (1) direct regulation through signalling pathways including mTOR, PI3K/AKT/mTOR (PAM), and K-Ras, and (2) indirect metabolic modulation involving insulin sensitivity and glucose metabolism [62, 63]. These dual mechanisms exhibit functional crosstalk rather than operating independently. Buzzai et al. demonstrated that metformin induces energy stress through the AMPK-p53 pathway, forcing tumour cells to undergo metabolic conversion (such as enhanced fatty acid β-oxidation and autophagy), while p53-deficient colon cancer cells undergo apoptosis due to their inability to adapt to this stress [64]. However, some studies have reveals less than satisfactory outcomes regarding its protective effects in diabetic patients with CRC [65]. The 2016 N0147 trial conducted by the North Central Cancer Treatment Group in the United States revealed no significant differences in disease-free survival (DFS), overall survival (OS), or time to recurrence (TTR) between metformin users and non-users among stage III colon cancer patients undergoing radical resection. This lack of benefit persisted regardless of KRAS or BRAF mutation status or mismatch repair (MMR) proficiency [66]. This discrepancy underscores a critical research gap: the lack of predictive biomarkers to identify patient subsets who might benefit from metformin, such as those defined by p53 status, KRAS/BRAF mutations, or metabolic profile. Furthermore, metformin’s interaction with chemotherapy and immunotherapy regimens remains poorly understood. To address these issues, future research directions should include the following: (i) conducting prospective clinical trials stratified by biomarkers (e.g., p53 and MMR status) to resolve efficacy controversies; (ii) performing preclinical and clinical studies evaluating metformin in combination with immunotherapy treatments, given its immunomodulatory potential; (iii) carrying out pharmacokinetic and pharmacodynamic studies to determine whether anticancer effects require doses different from those used for glycemic control.
Shifts in research focus: from epidemiology to mechanisms and translation
The temporal analysis of keywords and references reveals a clear paradigm shift. Early research (pre-2000s) was dominated by establishing epidemiological links. Subsequent decades saw a rise in investigating intermediate mechanisms like hyperinsulinemia and Metabolic Syndrome (MetS). Currently, the frontier is characterized by a focus on molecular mechanisms (e.g., CA, gut microbiota) and therapeutic/clinical outcomes (e.g., AL, metformin, survival). This evolution aligns with the broader movement towards precision oncology. However, a significant translational gap remains: few studies integrate patient-derived multi-omics data to personalize risk prediction or treatment for the colorectal cancer-diabetes comorbidity population. Bridging this gap requires interdisciplinary consortia that combine deep phenotyping, molecular profiling, and clinical trial data.
Limitation
This study performed a bibliometric analysis of literature on colorectal cancer-diabetes comorbidity. Unlike traditional reviews, this approach offers a clearer visualization of research progress. However, several limitations exist. First, relying solely on the WoSCC database may introduce bias due to incomplete coverage, particularly regarding non-English or regional publications, though WoSCC remains a widely authoritative source. Second, using citation metrics to assess impact is inherently biased: highly cited articles are not always the most rigorous, and significant newer work may lack sufficient citations. Third, keyword clustering and thematic mapping depend on algorithmic parameters and thresholds; varying these settings could alter results, underscoring the sensitivity of such unsupervised methods. Finally, bibliometric analysis is descriptive and correlational—it cannot establish causality or evaluate the scientific validity of findings. While it identifies trends, collaborations, and emerging topics, it does not assess evidence quality. Thus, these conclusions should be complemented by systematic reviews and experimental studies.
Conclusion
In this study, we conducted bibliometric and visual analysis with CiteSpace visualisation to map the colorectal cancer-diabetes comorbidity research landscape, which is more intuitively and clearly reflected in the research progress in the target area when compared with traditional narrative reviews. Colorectal cancer-diabetes comorbidity, as an interdisciplinary field of great interest, has research potential in the future.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Giovannucci E, Harlan D M, Archer M C, et al. Diabetes and Cancer: a Consensus Report[J]. CA: A Cancer Journal for Clinicians. 2010;60(4):207-221.10.3322/caac.2007820554718 · doi ↗ · pubmed ↗
- 2Li YF, Shi LJ, Wang P et al. Binding between ROCK 1 and DCTN 2 triggers diabetes‑associated centrosome amplification in colon cancer cells. Oncol Rep. 2021;46(1):151.10.3892/or.2021.8102 PMC 818550334080666 · doi ↗ · pubmed ↗
- 3Xue SN, Lei J, Yang C et al. The biological behaviors of rat dermal fibroblasts can be inhibited by high levels of MMP 9. Exp Diabetes Res. 2012;2012:494579.10.1155/2012/494579 PMC 334698322577368 · doi ↗ · pubmed ↗