Safety and efficacy of triple combination therapy in hypertension and dyslipidemia: a systematic review and meta-analysis of randomized controlled trials
Ahmed Yasser Shaban, Ahmed Hassan, Sherif Eltawansy, Malak A. Hassan, Mariam Tarek Desouki, Nourhan Ahmed, Salem Badr, Akram Y. Elgendy, Mahmoud Nassar, Diaa Hakim

TL;DR
This study finds that triple combination therapy is more effective than dual therapy in lowering blood pressure and improving lipid profiles in patients with hypertension and dyslipidemia.
Contribution
The study introduces and evaluates a novel triple therapy combining ARBs, amlodipine, and rosuvastatin for managing hypertension and dyslipidemia.
Findings
Triple therapy significantly reduced systolic and diastolic blood pressure compared to dual therapy.
Triple therapy improved LDL cholesterol levels more effectively than ARB/amlodipine combinations.
No significant differences were observed in adverse events between treatment groups.
Abstract
Hypertension (HTN) and dyslipidemia are major risk factors for cardiovascular diseases. Recently, researchers have investigated the potential benefits of combining multiple medications in one bill to improve their metabolic and cardiovascular efficacy. We investigated a treatment approach that combines two antihypertensive medications with one statin. We aim to assess the safety and effectiveness of a triple therapy regimen consisting of angiotensin receptor blockers (ARBs) combined with amlodipine/rosuvastatin. We compared this triple therapy to dual therapy involving either ARBs/amlodipine or ARBs/rosuvastatin in patients with HTN and dyslipidemia. We conducted systematic search in the following databases: Medline, Web of Science, Scopus, and Cochrane Library until August 2024. The main outcomes assessed were the variations in mean systolic blood pressure (mSBP), mean diastolic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
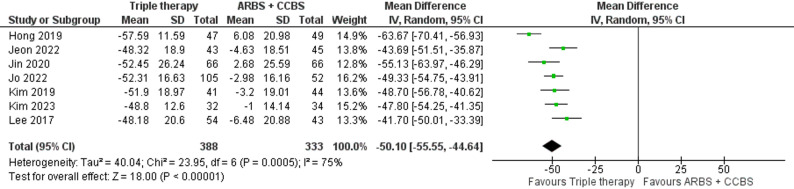 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4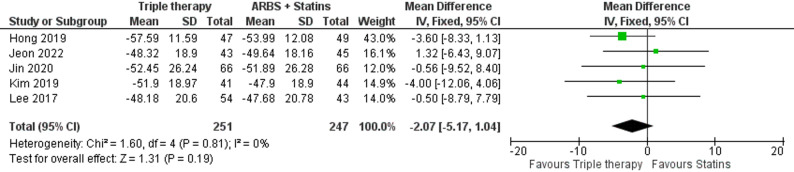 Figure 5
Figure 5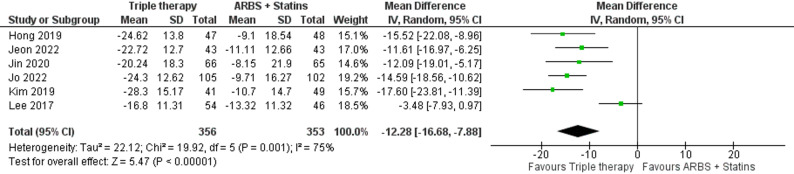 Figure 6
Figure 6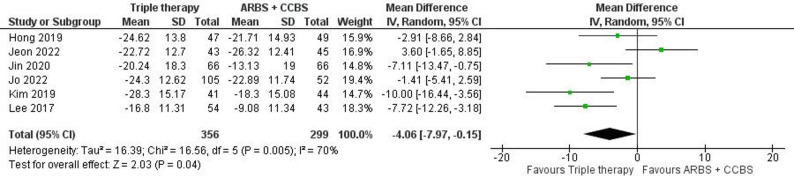 Figure 7
Figure 7 Figure 8
Figure 8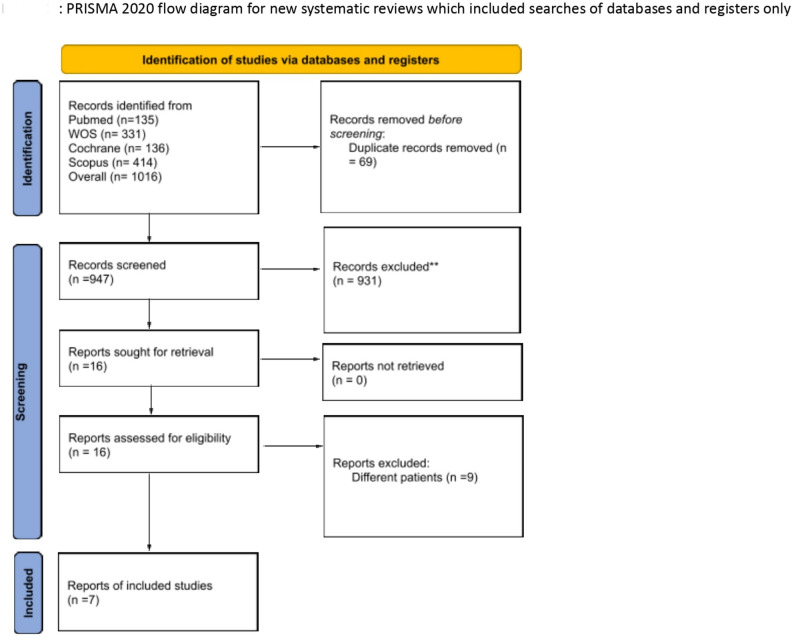 Figure 9
Figure 9Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBlood Pressure and Hypertension Studies · Renin-Angiotensin System Studies · Lipoproteins and Cardiovascular Health
Introduction
Cardiovascular disease (CVD) is considered one of the most common causes of morbidity and mortality worldwide [1]. A significant percentage of patients diagnosed with hypertension (HTN) concurrently exhibit dyslipidemia [2, 3]. Piepoli et al. have highlighted a direct correlation between blood cholesterol and CVD, emphasizing the importance of reducing cholesterol to effectively lower CVD risk [4]. As a result, recent HTN management has focused not only on lowering blood pressure but also on reducing overall CVD risk and this can be achieved by lifestyle modification and optimizing medication regimens to improve patient compliance and improve clinical outcomes [3, 5]. In 2017, the American College of Cardiology and American Heart Association published guidelines on hypertension treatment in adults which recommend combining two antihypertensive drugs from different classes for managing second-stage hypertension, defined as a blood pressure (BP) > = 140/90 mmHg [6]. The guidelines recommend ARBs combined with calcium channel blockers (CCBs) as a first-line treatment among the various available drug combinations.
Rosuvastatin is an effective and safe option for treating dyslipidemia [7]. However, many patients continue to experience uncontrolled dyslipidemia, which further increases their cardiovascular risk. While previous meta-analyses have focused on comparing the efficacy of various pharmacological interventions for HTN, they have given limited attention to the coexistence of dyslipidemia [8, 9].
The optimal treatment strategy should tackle all these factors simultaneously, once-daily dosing and fixed-dose combination therapy can maintain good control of both BP and cholesterol levels.
Hence, we perform this systematic review and meta-analysis to assess the safety and efficacy of triple combination therapy with ARBs/amlodipine plus rosuvastatin compared with ARBs/amlodipine or ARBs/rosuvastatin in patients with HTN and dyslipidemia.
Method
Search strategy and data collection
We systematically searched PubMed/Medline, Web of Science, Scopus, and the Cochrane Library for relevant studies up to August 2024 using the following search terms: (“Telmisartan” OR “Pritor” OR “BIBR” OR “Micardis” OR “Kinzalmono” OR “Semintra” OR “Tolura”) OR (“Amlodipine” OR “Amlodis” OR “Norvasc” OR “Istin” OR “Amlor”) OR (“Rosuvastati” OR “Crestor” OR “Ezallor”) AND (“Dyslipidemia” OR “Dyslipoproteinemia*” OR “Hyperlipidemia*” OR “Hypercholesterolemia*” OR “Hyperlipoproteinemia*” OR “Hypertriglyceridemia*” OR “Atherosclerosis”) AND (“Hypertension” OR “High Blood Pressure”) (Supplementary Table 1). To ensure comprehensiveness, manual searches were also performed by the first four authors using alternative terms, including “losartan,” “valsartan,” and “olmesartan,” while focusing the strategy to minimize irrelevant studies.
We used Endnote software (Clarivate Analytics, PA, USA) for duplicate removal. The screening of the retrieved studies was conducted in 2 stages: First, AH, MTD, HMA, and NA independently screened the titles and abstracts to evaluate their relevance. Next, the full text of the selected abstracts was screened to determine if they fulfilled the inclusion and exclusion criteria. We used the Rayyan website [10] to facilitate the screening process.
Studies including the following inclusion criteria were included: (1) Studies that enrolled patients with both HTN and dyslipidemia or hypercholesterolemia; (2) Studies comparing triple therapy with ARBs/amlodipine plus rosuvastatin versus dual therapies with ARBs/amlodipine or ARBs with rosuvastatin; and (3) Studies that reported our search outcomes and were published in international peer-reviewed journals. We excluded non-English studies, abstracts without available data, Literature reviews, preclinical studies, and pharmacokinetics/pharmacodynamics studies.
A fourth co-author independently extracted the data to MS excel sheet, with any conflicts regarding study inclusion resolved by a fifth co-author. We organized the extracted data into three domains: (1) summary of study characteristics, (2) baseline characteristics of the study population, and (3) study outcomes.
Outcomes
Primary outcome measures were the differences in mean systolic and diastolic blood pressure (mSBP, mDBP) and the relative changes in LDL and HDL cholesterol (LDL-C, HDL-C) after eight weeks of treatment. Secondary outcomes included overall adverse events, cerebrovascular adverse events, and adverse drug reactions.
Risk of bias assessment
The revised Cochrane risk-of-bias tool (RoB2) was used to evaluate the risk of bias in the included randomized controlled trials (RCTs) [11]. It included the process of randomization, concealment, deviations from intended interventions, use of appropriate analysis to assess the intervention, outcome measurement, selection of reported overall risk of bias and results. The methodological quality of the studies was categorized as either low risk, some concerns, or high risk of bias. Two independent authors assessed the risk of bias, and disagreements were resolved through discussion with a third author.
Statistical analysis
We used RevMan v5.3 for statistical analysis [12]. Continuous outcomes were presented as mean difference (MD) with corresponding 95% confidence intervals (C.I.), while categorical outcomes were presented as risk ratios (R.R) with corresponding 95% C.I., which describe the ratio of the risk of an outcome event between the two groups. A fixed-effect model was applied for homogeneous outcomes; however, a random-effect model was utilized when significant heterogeneity was detected. I² and Chi-square tests were used to assess heterogeneity, where Chi-square determines the presence and degree of heterogeneity. I² values were interpreted according to the Cochrane Handbook (Chap. 9) [13] as follows: 0–40% (not significant), 30–60% (moderate), 50–90% (substantial), and 75–100% (considerable). A significance level (α) below 0.1 in the Chi-square test was considered indicative of significant heterogeneity, as per the Cochrane Handbook (Part 2, Chap. 9) [13]. Heterogeneity in some outcomes was resolved using a random-effect model and conducting a sensitivity analysis. We excluded one study at a time and generated forest plots for the remaining studies to achieve the lowest possible heterogeneity. For dealing with missing data, when the standard deviation (SD) of change in outcomes was not provided, we calculated it from the standard error (SE) or 95% CI, as per Altman’s methods [14].
Publication bias
A test for publication bias was not conducted, as tests for funnel plot asymmetry are recommended only for the outcome reported in at least ten studies, according to Cochrane guidelines [13].
Results
We screened 1,016 articles through our search, with 947 remaining after removing duplicates. Following the title and abstract screening, we selected 16 articles for full-text screening. Out of these, seven studies were finally included [5, 15–20]. The PRISMA flow diagram illustrates the selection process in Fig. 1, and the study is registered on PROSPERO (CRD42024570094). Six studies were assessed as having a low risk of bias, while one study showed some concerns, particularly related to selection bias (Supplementary Fig. 1). The characteristics of the included studies are detailed in Supplementary Table 2.
Fig. 1PRISMA flow diagram of the included studies
Baseline characteristics
We included 1,074 patients, 67.6% of them were male. The group receiving triple therapy had a mean age of 64.50 ± 9.58 years, with a mean SBP of 152.15 ± 12.72 mmHg and a mean LDL-C level of 154.97 ± 1.39 mg/dL. In comparison, the cohort treated with ARBs/amlodipine had a mean age of 63.75 ± 9.91 years, a mean SBP of 150.70 ± 11.87 mmHg, and a mean LDL-C of 154.91 ± 31.20 mg/dL. Meanwhile, the group receiving ARBs with rosuvastatin had a mean age of 63.25 ± 9.30 years, a mean SBP of 151.62 ± 12.52 mmHg, and a mean LDL-C of 156.85 ± 32.66 mg/dL. Four studies administered triple combination therapy in the form of three tablets, while two studies used two tablets—one combining ARBs/amlodipine and the other containing rosuvastatin. In contrast, one study (Kim et al., 2023) used a single tablet for triple therapy.
Additional baseline characteristics are described in Table 1.
Table 1. Baseline characteristics of included studies (T1)Study IDArms N Patient demographicsRisk factorLaboratory parametersAge (y) mean ± SDMale N (%)BMI (kg/m2)mean ± SDDM, N (%)Smoking Status N (%)Total Cholesterol (mg/dL) Mean ± SDLDL-C (mg/dL) Mean ± SDHDL-C (mg/dL) Mean ± SDSBP (mmHg) Mean ± SDCurrentFormerKim 2023[15]Olmesartan/ Amlodipine/ Rosuvastatin 20/5/5 mg3259.2 ± 9.820 (62.5)25.7 ± 2.3-3 (12.5)-----Amlodipine / Olmesartan20/5 mg3460.9 ± 11.823 (67.6)25.6 ± 2.6-10 (32.3)-----Jeon 2022[16]fmasartan/ Amlodipine + Rosuvastatin 60/10/20 mg4359.6 ± 7.432 (74.4)--30 (57.7)15 (34.9)221.8 ± 28.4157.21 ± 27.4548.4 ± 13.7154 ± 10.3fmasartan /Amlodipine60/10 mg4560.8 ± 6.336 (8)--12 (26.7)16 (35.6)213.5 ± 35.6151.22 ± 32.8645.9 ± 12.1152.9 ± 8.7fmasartan + Rosuvastatin 60/20 mg4360.7 ± 6.830 (69.8)--12 (27.9)9 (20.9)223.8 ± 40.1157.95 ± 36.4348.8 ± 10.6152.5 ± 8.6Jo 2022[17]Olmesartan/Amlodipine (SPC) + Rosuvastatin 40/10/20 mg10565.18 ± 9.3459 (56.2)26.75 ± 3.3-21 (20)27 (25.7)216.98 ± 34.8154.52 ± 30.8449.23 ± 11.9153.58 ± 10.9Olmesartan /Amlodipine 40/10 mg5264.06 ± 8.931 (59.6)26.67 ± 3.3-10 (19.2)12 (23.1)223.48 ± 37.2-48.65 ± 10.7151.30 ± 8.9Olmesartan + Rosuvastatin 40/20 mg10263.49 ± 9.858 (56.9)26.60 ± 3-26 (25.5)20 (19.6)220.63 ± 35.2160.42 ± 32.0546.87 ± 11.5153.71 ± 11.1Jin 2020[18]Telmisartan/ Amlodipine+ Rosuvastatin 80/5/20 mg6668.33 ± 8.345 (68.2)26.26 ± 3.428 (42.42)10 (15.15)-225.55 ± 34.3160.12 ± 32.3446.38 ± 10.9155.40 ± 12.1Telmisartan/Amlodipine 80/5 mg6666.01 ± 10.4348 (72.7)26.67 ± 2.829 (43.94)15 (22.73)-218.17 ± 36.9153.41 ± 31.3047.80 ± 12155 ± 12.1Telmisartan+ Rosuvastatin 80/20 mg6564.9 ± 9.1146 (70.8)26.60 ± 3.232 (49.23)11 (16.92)-221.20 ± 38.7153.88 ± 36.7347.89 ± 12.9154.42 ± 12.9Hong 2019[19]Telmisartan/ Amlodipine+Rosuvastatin 80/10/20 mg4767.96 ± 9.4433 (70.21)26.52 ± 3.1215 (31.91)--216.38 ± 31.68150.51 ± 31.7846.17 ± 12.36149.49 ± 12.09Telmisartan/Amlodipine 80mg/10 mg4966.63 ± 10.2231 (63.27)26.55 ± 2.9216 (32.65)--219.84 ± 37.88153.12 ± 35.1849.76 ± 13.60144.29 ± 11.09Telmisartan + Rosuvastatin 80/20 mg4865.88 ± 9.1334 (70.83)27.67 ± 3.4113 (27.08)--225.69 ± 32.84158.92 ± 30.6247.44 ± 11.98147.08 ± 13.69Kim 2019[20]Telmisartan/Amlodipine+ Rosuvastatin 80/10/20 mg4167.4 ± 10.029 (72.5)-15 (37.5)--223.5 ± 36.1155 ± 29.250.2 ± 14.5156.8 ± 13.7Telmisartan/Amlodipine 80/10 mg4466.4 ± 11.027 (62.8)-16 (37.2)--221.6 ± 28.9155.7 ± 23.146.3 ± 10.7154.8 ± 10.6Telmisartan+ Rosuvastatin 80/20 mg4963.4 ± 9.737 (75.5)-15 (30.6)--228.5 ± 36.5160 ± 3246.9 ± 10.3154.8 ± 10.6Lee 2017[21]Amlodipine/ Losartan Potassium/ Rosuvastatin 5/100/ 20 mg5460.33 ± 8.4837 (68.52)26.36 ± 3.08---219.91 ± 38.20151.63 ± 35.5946.72 ± 11.43142.74 ± 13.64Amlodipine/ Losartan Potassium 5/100 mg.4359.28 ± 7.4435 (81.40)26.47 ± 2.85---215.49 ± 29.75162.33 ± 31.8645.33 ± 11.29144.15 ± 14.04Losartan Potassium/ Rosuvastatin 100/20 mg4659.83 ± 9.0935 (76.09)27.50 ± 3.88---235.11 ± 38.62146.58 ± 25.3646.26 ± 10.53143.54 ± 14.39Data are presented as mean ± SD or n (%).Body mass index, (BMI); Diabetes mellitus, (DM); High-density lipoprotein-cholesterol, (HDL-C); Low-density lipoprotein-cholesterol (LDL-C); Systolic blood pressure, (SBP); Single pill combination, (SPC).
Clinical outcomes
Triple therapy vs. ARBs/Amlodipine
Change in mSBP
Our analysis included six studies with 356 patients in the triple therapy group and 299 in the ARBs/amlodipine group. The results showed a significant difference in favor of the triple therapy group (MD: -4.06, 95% C.I. [-7.97: -0.15], p-value = 0.04) (Fig. 2). However, we observed considerable heterogeneity (P = 0.005, I² = 70%), which was resolved by excluding the study by Jeon et al., 2022 (Figure S2).
Fig. 2. Forest plot of change in mean systolic blood pressure (mSBP) (Triple therapy vs. ARBs/amlodipine)
Change in mDBP
The triple therapy group (181 participants) showed a significant reduction in mDBP (MD: -5.45, 95% C.I. [ -7.96: -2.93], p-value < 0.0001) compared with the ARBs/amlodipine group (Fig. 3). Moderate heterogeneity was found (P = 0.10, I² = 52%), which was addressed by removing the Hong, 2019 study (Figure S3).
Fig. 3. Forest plot of change in mean diastolic blood pressure (mDBP) (Triple therapy vs. ARBs/amlodipine)
Change in LDL-C
This outcome was reported in seven studies with 388 participants in the triple therapy group and 333 in the ARBs/amlodipine group. A significant reduction in LDL-C was reported in the triple therapy group (MD: -50.10, 95% C.I. [-55.55: -44.64], p-value < 0.00001) (Fig. 4). Heterogeneity was significant (I² = 75%), but resolved by excluding Hong, 2019 (Figure S4).
Fig. 4. Forest plot of mean percentage change in LDL-C (Triple therapy vs. ARBs/ amlodipine)
Change in HDL-C and triglycerides (TGs)
Three studies with 137 participants in the triple therapy group and 134 in the ARBs/amlodipine group found a significant increase in HDL-C but no significant difference in triglyceride levels (MD: 8.7, 95% C.I. [4.67: 12.74], p-value < 0.0001), (MD: -6.89, 95% C.I. [-15.75 to 1.96], p-value = 0.13), respectively (Fig. 5, S5).
Fig. 5. Forest plot of mean percentage change in HDL-C (Triple therapy vs. ARBs/ amlodipine)
Safety outcomes
The two groups showed no statistically significant differences regarding total adverse events and adverse drug reactions (R.R: 1. 09, 95% C.I. [0.73: 1.63], p-value = 0.66) and (R.R: 1.03, 95% C.I. [0.59: 1.78], p-value = 0.93), respectively (Figure S6, S7). For CNS adverse events, data from four studies also showed no significant differences (R.R: 1.18, 95% C.I. [0.34, 4.09], p-value = 0.79), (Figure S8).
All clinical outcomes were assessed over a duration of 8 weeks with no heterogeneity in the change in HDL-C, change in TG, or any of the safety outcomes between the two groups.
Triple therapy vs. ARBs with Rosuvastatin
Change in mSBP
In a comparison of six studies with 356 patients in the triple therapy group and 353 in the ARBs with rosuvastatin group, the triple therapy showed a significant reduction in mSBP (MD: -12.28, 95% C.I. [-16.68: -7.88], p-value < 0.00001) (Fig. 6, though there was significant heterogeneity resolved by excluding the study by Lee, 2017 (Figure S9).
Fig. 6. Forest plot of change in mean systolic blood pressure (mSBP) (Triple therapy vs. ARBs with rosuvastatin)
Change in mDBP
There was a significant reduction in mDBP when comparing 185 participants in the triple therapy group with 186 in the ARBs with rosuvastatin group that favores the triple therapy (MD: -6.48, 95% C.I. [-10.95: -2.01], p-value = 0.005) (Fig. 7). However, removing the Kim, 2019 study reduced the heterogeneity (P = 0.0002, I² = 85%), though it did not resolve it completely (Figure S10).
Fig. 7. Forest plot of change in mean diastolic blood pressure (mDBP) (Triple therapy vs. ARBs with rosuvastatin)
Change in LDL-C
We did not notice any significant difference in LDL-C reduction between the two groups in the included Five studies with 251 participants in the triple therapy group and 247 in the ARBs with rosuvastatin (MD: -2.07, 95% C.I. [-5.17: 1.04], p-value = 0.19) (Fig. 8).
Fig. 8. Forest plot of mean percentage change in LDL-C (Triple therapy vs. ARBs with rosuvastatin)
Change in HDL-C and triglycerides (TGs)
The analysis of three studies with 137 patients in the triple therapy group and 135 in the ARBs with rosuvastatin group found no significant difference in HDL-C levels and TGs levels (MD: -2.58, 95% C.I. [-11.65: 6.49], p-value = 0.58), (MD: 1.91, 95% C.I. [-6.64: 10.47], p-value = 0.66), respectively. (Fig. 9, S12). Heterogeneity was notable in HDL-C change, which was resolved by excluding the study by Young, 2017 (Figure S11).
Fig. 9. Forest plot of mean percentage change in HDL-C (Triple therapy vs. ARBs with rosuvastatin)
Safety outcomes
In our analysis, five studies reported total adverse events, showing no difference between the groups (R.R: 1. 06, 95% C.I. [0.71: 1.58], p-value = 0.79) (Figure S13). Similarly, there were no differences in adverse drug reactions (R.R: 1.41, 95% C.I. [0.77: 2.58], p-value = 0.27) (Figure S14) or CNS adverse events (R.R: 0.82, 95% C.I. [0.28: 2.40], p-value = 0.72) (Figure S15).
All clinical outcomes were evaluated over 8 weeks, with no heterogeneity observed in the changes in LDL-C, triglycerides, or any safety outcomes between the two groups.
Discussion
Our meta-analysis included 1,074 patients from seven RCTs and evaluated the effects of triple therapy (ARBs/amlodipine plus rosuvastatin) compared with double therapy (ARBs/amlodipine or ARBs plus rosuvastatin) on blood pressure, lipid profiles, and safety outcomes. Triple therapy significantly reduced mSBP and mDBP compared to both double therapy groups and was associated with notable improvements in LDL-C and HDL-C levels, particularly compared to the ARB/amlodipine group. Importantly, our study also assessed the safety of triple therapy versus double therapy, revealing promising results suggesting that both approaches are similarly safe. No significant differences were observed in TG levels across the comparisons, and triple therapy showed comparable lipid effects to ARBs plus rosuvastatin.
The prevalence of HTN is rising alongside dyslipidemia, with up to 80% of patients experiencing both conditions simultaneously [21, 22]. Antihypertensive therapy can effectively reduce cardiovascular events—such as myocardial infarction, and heart failure—by 20% to 50% [23]. Clinical guidelines strongly recommend statins for lowering LDL-C in CVD prevention [24]. However, significant treatment gaps persist in clinical practice. Only half of hypertensive patients receive treatment, with just 34% achieving adequate blood pressure control [25]. Similarly, statins and lipid-modifying agents remain underutilized in high-risk populations, contributing to preventable cardiovascular events [26, 27]. Compliance with statin therapy is also suboptimal, with 60% of patients ceasing treatment within the initial year and only 25% reaching their LDL-C targets [28, 29]. Non-compliance with prescribed medications significantly contributes to these outcomes, leading to treatment failures and widening the disparity between clinical recommendations and actual results [30]. The complexity of managing multiple medications often overwhelms patients, especially those dealing with several health conditions or older individuals, resulting in poor adherence rates.
Previous studies have shown that statin therapy can lower blood pressure which might be attributed to its pleotropic effect or other mechanisms [31–34]. For instance, a large meta-analysis involving around 50,000 patients from 46 clinical trials [32] found that statins, regardless of type or dosage, effectively reduce blood pressure, especially in younger individuals. These findings support the use of statins in combination with blood pressure medications, as seen in our study, where a statin was administered alongside two blood pressure medications. It’s worth noting that our study also assessed the safety of triple therapy versus double therapy, revealing promising results that suggest both approaches are similarly safe. However, a major drawback of triple therapy is its higher cost compared to monotherapy, along with potential challenges from drug interactions, which may complicate the interpretation of reported side effects.
Considering the close association between HTN and dyslipidemia—both are major risk factors for CVD—earlier investigations have explored the efficacy of integrating antihypertensive agents with lipid-lowering medications, such as statins [35, 36]. A prior meta-analysis [37] encompassing six RCTs demonstrated favorable outcomes for a triple therapeutic regimen comprising ACE inhibitors, diuretics, and calcium channel blockers, resulting in enhanced blood pressure regulation without compromising safety. Furthermore, a recent meta-analysis [38] underscored the critical role of triple antihypertensive treatment in individuals with high-risk hypertension. Consequently, we advocate for a novel therapeutic strategy that combines two antihypertensive drugs with a single statin. This approach is potentially beneficial for the proper treatment of both elevated blood pressure and dyslipidemia. While previous studies have investigated triple therapy, our analysis uniquely focuses on evaluating the efficacy of the combination of two antihypertensive medications alongside one statin.
Although the included studies vary in the number of pills administered, our hypothesis suggests that reducing tablet quantity could significantly boost patient compliance with prescribed medications, potentially leading to improved cardiovascular metrics. As such, we emphasize additional RCTs that evaluate the efficacy of triple therapy, consolidated into one pill, compared to dual therapy in patients diagnosed with hypertension and dyslipidemia. This approach aligns with the current trend of combining multiple classes of antihypertensive drugs into a single tablet [39, 40].
Strength and limitations
Our study stands as the first systematic review and meta-analysis assessing the efficacy and safety of triple therapy combining ARBs, amlodipine, and rosuvastatin in patients with hypertension and dyslipidemia, providing robust evidence on both blood pressure reduction and lipid profile improvement. All included studies were multicenter RCTs with no patient overlap; most were double-blind, except Kim et al. (2023), which was open label.
However, several limitations should be noted. All studies were conducted in Korea, potentially limiting generalizability to other populations. There was variability in drug dosages and formulations across trials, and sample sizes were relatively small. Additionally, patient adherence and compliance were not reported, which may affect real-world applicability.
Conclusion
Our meta-analysis highlights that triple combination therapy with ARBs/amlodipine and rosuvastatin significantly lowers blood pressure, improves lipid profiles, and is similarly safe compared to double therapy in patients with hypertension and dyslipidemia. Future studies should focus on developing a single-pill triple-combination therapy and evaluating its impact on adherence and clinical outcomes.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Piepoli MF, Hoes AW, Agewall S et al (2016) European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts)Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J. 2016;37(29):2315–2381. 10. · doi ↗ · pubmed ↗
- 2Kones R. Rosuvastatin, inflammation, C-reactive protein, JUPITER, and primary prevention of cardiovascular disease – a perspective. DDDT. Published online December 2010:383. doi:10.2147/DDDT.S 1081210.2147/DDDT.S 10812 PMC 302326921267417 · doi ↗ · pubmed ↗
- 3Ro B 2: A revised Cochrane risk-of-bias tool for randomized trials | Cochrane Bias. Accessed August 3 (2023) https://methods.cochrane.org/bias/resources/rob-2-revised-cochrane-risk-bias-tool-randomized-trials
- 4Rev Man, Web (2024) Cochrane’s systematic-review production software, is now available to the wider academic community | Cochrane. November 30, Accessed November 30, 2024. https://www.cochrane.org/news/revman-web-cochranes-systematic-review-production-software-now-available-wider-academic
- 5Cochrane Handbook for Systematic Reviews of Interventions | Cochrane Training. Accessed November 21 (2024) https://training.cochrane.org/handbook/current
- 6Strazzullo P, D’Elia L, Versiero M (2007) Response to upregulation of nitric Oxide, Inhibition of oxidative Stress, and antihypertensive effects of Statins. Hypertension 49(6). 10.1161/HYPERTENSIONAHA.107.09021710.1161/HYPERTENSIONAHA.107.09015917404175 · doi ↗ · pubmed ↗
- 7Zaman MA, Awais N, Satnarine T et al (2023) Comparing Triple Combination Drug Therapy and Traditional Monotherapy for Better Survival in Patients With High-Risk Hypertension: A Systematic Review. Cureus. Published online July 5. 10.7759/cureus.4139810.7759/cureus.41398 PMC 1040189737546040 · doi ↗ · pubmed ↗