Contextualisation of the safeTALK™ Suicide Prevention Program: A Descriptive Qualitative Study
Rita Pokharel Poudel, Diana Jefferies, Sheeja Perumbil Pathrose, Peter M. Gutierrez, Lucie M. Ramjan

TL;DR
This study adapts the safeTALK™ suicide prevention program for use in Nepal by incorporating local cultural and socioeconomic factors.
Contribution
The study provides a culturally contextualized adaptation of a suicide prevention program for Nepalese adolescents using community-based participatory research.
Findings
Participants emphasized the high need for adolescent suicide prevention in Nepal due to cultural and socioeconomic factors.
Stigma around suicide was identified as a barrier preventing adolescents from seeking help.
Modifications such as translating the program into Nepali and incorporating local cultural practices were suggested.
Abstract
Suicide prevention programmes have effectively reduced suicidal behaviours, increased knowledge and fostered help‐seeking. However, suicide is a complex phenomenon, and its risk and protective factors differ across cultures. To contextualise the LivingWorks safeTALK™ suicide prevention programme for secondary school students in Nepal. A qualitative descriptive approach using focus groups informed by the Socio‐Ecological Model and guided by Community‐Based Participatory Research (CBPR) was used. The study was conducted in Nepal via Zoom™ from Australia, from September 15–30, 2024. Five focus groups were conducted with 18 participants, including adolescents, schoolteachers, parents, healthcare providers, and policymakers. Data were transcribed, translated to English and uploaded to NVivo v.14. A hybrid content analysis approach was used. Data were presented across seven categories: 1.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
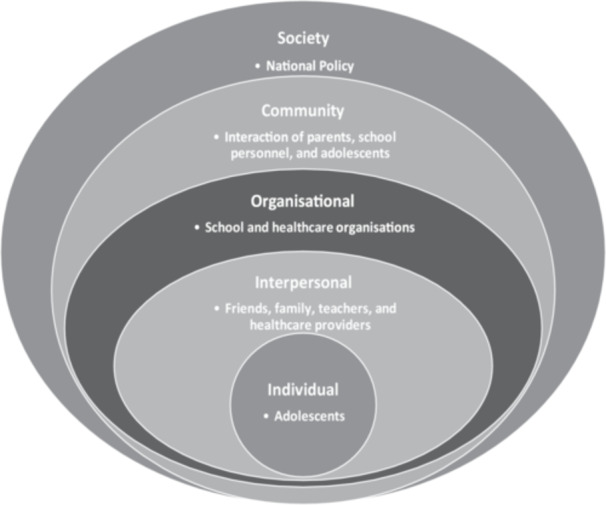 FIGURE 1
FIGURE 1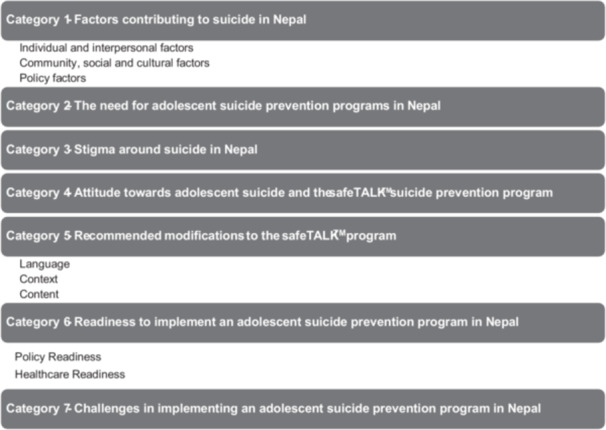 FIGURE 2
FIGURE 2| Characteristics | Adolescents ( | Parents ( | Teachers ( | Healthcare providers ( | Policymakers ( | Total ( |
|---|---|---|---|---|---|---|
|
| 16–17 years | — | — | — | — | — |
|
| ||||||
| Female | 5 | — | 1 | 2 | 2 | 10 (55.55%) |
| Male | 2 | 3 | 1 | 1 | 1 | 8 (44.45%) |
|
| ||||||
| Janajati | 5 | — | — | 1 | — | 6 (33.33%) |
| Bramhin/Chhetri | 2 | 1 | — | 1 | 3 | 7 (38.89%) |
| Madheshi | — | 2 | 2 | — | — | 4 (22.22%) |
| Dalit | — | — | 1 | — | 1 (5.56%) | |
|
| NA | NA | 8–12 years | 2–5 years | 5–18 years | NA |
| Category | Sub‐category | Exemplar quotes |
|---|---|---|
| Factors contributing to suicide in Nepal | Individual and interpersonal factors |
|
| Community, social and cultural factors |
| |
| Policy factors |
| |
| The need for adolescent suicide prevention programmes in Nepal |
| |
| Stigma around suicide in Nepal |
| |
| Attitude towards adolescent suicide and the safeTALK™ suicide prevention programme |
| |
| Recommended modifications to the safeTALK™ programme | Language |
|
| Context |
| |
| Content |
| |
| Readiness to implement an adolescent suicide prevention programme in Nepal | Policy readiness |
|
| Healthcare readiness |
| |
| Challenges in implementing an adolescent suicide prevention programme in Nepal |
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSuicide and Self-Harm Studies · Mental Health Treatment and Access · COVID-19 and Mental Health
Background
1
The population suicide rate in Nepal was reported to be 23.56/100,000 in 2023 [1]. However, a school‐based survey in Nepal found that over 10% of adolescents aged 11 to 18 years had attempted suicide. The same study highlighted a lack of culturally appropriate prevention programmes [2]. Countries that have implemented school‐based suicide prevention programmes have effectively reduced suicidal behaviour [3, 4, 5, 6], increased knowledge about suicide, and fostered help‐seeking behaviour [7, 8, 9, 10, 11]. These programmes have instilled confidence in students to offer help to others who may be considering suicide [12, 13]. The safeTALK™ programme, developed by LivingWorks, is one of the prevention programmes that has been reported to be effective in increasing knowledge about suicide, a willingness to talk about suicide and help‐seeking intentions among school students in many countries, such as Canada, Australia, and the United Kingdom [7, 14, 15, 16, 17, 18].
While many school‐based interventions are prepared by experts, when the programmes are implemented in schools, there has been no evidence that stakeholders were involved as co‐researchers during the programme development. Furthermore, the programmes are not adapted for other cultures. As the theoretical models providing guidelines for suicide prevention research are derived from data obtained in Western cultures, many programmes are less likely to work in Low‐ and Middle‐Income Countries (LMICs) without contextualisation based on local cultures. This is because there are substantial differences in terms of gender roles and other sociocultural beliefs and practices from one culture to another [19]. To ensure that the prevention strategy is compatible in a different culture and context, the process of contextualisation can be employed to modify or adapt an existing evidence‐based programme to a different culture and context [20]. This is a crucial step as suicide is a complex phenomenon and its risk factors, protective factors, and preventive approaches differ across diverse cultures [2]. Lakshmi and Michale highlight a need to modify and adapt programmes implemented in High‐Income Countries before they are implemented in LMICs [19]. However, there are currently no contextualised suicide prevention programmes available to adolescents in LMICs [21]. Therefore, this study reports on the contextualisation of an existing suicide prevention programme— LivingWorks safeTALK™—for secondary school students in Nepal.
Aim
2
The aim of this study was to explore the socio‐cultural adaptations necessary to contextualise the safeTALK™ suicide prevention programme for use among secondary school students in Nepal.
Methods
3
Study Design
3.1
A qualitative descriptive approach was used to understand the needs and views of local people regarding adolescent suicide prevention in Nepal. This approach provided a comprehensive understanding of the needs of adolescents in Nepal, their risk factors for suicide, and the required approach for prevention. The qualitative descriptive design is typically selected when direct accounts of phenomena are required, and little is known about the topic. This is a flexible approach which provides a rich and comprehensive understanding of the phenomenon that stays close to the participants' own words [22, 23]. This study adhered to the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist [24] (Supporting File 1).
Theoretical Framework
3.2
Understanding that suicide is a complex, multilayered sociocultural phenomenon, this study was informed by the Socio‐Ecological Model [25] as the guiding framework (Figure 1). The core principles of the model are that multiple factors influence human behaviour and it requires a coordinated multilevel approach to modify such behaviours [25, 26, 27]. Suicide is a public health problem that requires a multilevel approach to prevent it. Through collaboration with the service provider LivingWorks Australia, adolescents, parents, teachers, school nurses, healthcare providers, and policymakers participated in this study to co‐develop a culturally appropriate version of the existing safeTALK™ suicide prevention programme.
Socio‐ecological model (SEM).
Sociocultural Adaptation of the Programme
3.3
The Programme
3.3.1
safeTALK™ is an educational programme (a half‐day workshop) designed to assist learners, aged 15 years or above, to recognise when another person is giving invitations, that is, inviting the person to explore their experience of suicidal thoughts. The person can then respond to the other person by applying basic TALK steps and connecting the other person to resources that can keep them safe. The name safe TALK is made up of two acronyms “safe” stands for suicide alertness for everyone and “TALK” stands for Tell Ask Listen and Keep Safe. The programme includes presentations, videos, discussions, questions, and role‐plays to ensure that participants can provide safe and effective assistance to someone experiencing suicidal thoughts [28]. The programme has been shown to increase helpers' knowledge about suicide, belief that suicide is preventable, and willingness to help in several studies in Australia [7, 15, 17]. This study did not involve delivering the full programme. Instead, it focused on identifying the socio‐cultural adaptations needed to contextualise the programme for future use among secondary school students in Nepal.
Research Team
3.4
The research team consisted of a novice to expert qualitative researchers. The interviewer holds a Master of Science in Psychiatric Nursing degree and is a PhD candidate. She had prior experience of working as a Registered Psychiatric Nurse in Nepal, and undertook LivingWorks safeTALK™ [28], LivingWorks Applied Suicide Intervention Skills Training (ASIST) [29], and safeTALK™ training for trainers [30] prior to conducting the study. She also had some prior experience in research with young people and qualitative data collection. The PhD candidate was supported by more experienced qualitative researchers (DJ and LR) during the initial focus groups, data categorisation and writing up of the results (DJ, SPP and LR). All research team members (RP, DJ, SPP and LR) received safeTALK™ and ASIST training [28, 29].
The PhD candidate belongs to the same culture, and is a bilingual Nepali speaker; however, she did not have a relationship with the participants prior to the study. She was known to the participants as a Registered Psychiatric Nurse of Nepal and a PhD candidate at Western Sydney University, Australia.
Setting
3.5
This study was conducted in a public school in the Sunsari district of Koshi Province in Nepal. The school was conveniently selected for this study as per the study protocol [31]. This school is regarded as one of the region's most respected public schools and is the second largest in the province. It also attracts students from neighbouring districts and cities of the region, with more than 100 students studying in 1 year. There were 641 students studying in grade 11 at the time of this study. Nepal is a low‐income South Asian country and ranks 110th on the Legatum Prosperity Index [32]. The country is in the central Himalayan region, enjoys five seasons, and receives monsoons from June to September, with 2500 mm of rain each year. Nepal is a culturally diverse country with 50 different religious festivals celebrated with a fixed date marked in the Nepalese calendar. However, festivals are not confined to these dates; there are other festivals celebrated locally by ethnic groups. Public holidays are held on the most important days of those festivals, and they can be either local or national holidays. Dashain, Tihar, and Chhath Parva are the biggest festivals in Nepal, and at this time of the year (October to November), there is a long national holiday season, and most of the schools are closed during these festivals.
In this study, the researcher considered how to best plan travel to Nepal, considering the tourist season, weather, students' curricular activities, the school calendar, including the national board exam for school level, and festival closures in Nepal prior to data collection.
Sampling
3.6
Purposive, convenience, and snowball sampling techniques were used to recruit participants for this study. Students studying in grade 11 in a public school in Sunsari district, their parents, teachers, school nurses, mental health professionals, and representative health policymakers were the participants in this study. Grade 11 students were selected, as recommended by the school principal, to prevent disruptions to the academic schedules of students preparing for national‐level board examinations. The sample size was informed by Malterud's concept of information power, which suggests that the level of information power is influenced by five key factors: (1) study aim, (2) sample specificity, (3) use of established theory, (4) dialogue quality, and 5) analysis strategy [33]. This study's aim was narrow and focused on the phenomenon of interest, sample specificity was high, a theoretical model (SEM) informed the analysis, dialogue quality varied but overall focus group discussions were robust, and an exploratory cross‐case analysis was employed.
Recruitment
3.7
Participants were recruited across five different groups (adolescents, teachers, parents, healthcare providers, and policymakers).
To recruit the adolescents and teachers, the researcher visited the school (research site) and met with the school principal. The principal allocated one of the teachers to support the coordination of the focus group. Participant information sheets (PIS) and consent forms for parents, along with recruitment flyers, were distributed in the classroom. If the parents agreed to allow their child to participate and signed a consent form, a second process of consent was undertaken for the students themselves. The recruitment process was completed by the research support person. The research team also obtained consent from the teachers and the school nurse to be part of a second focus group.
A snowball technique was used to recruit parents of adolescents, and they were contacted via telephone and given further information at a face‐to‐face meeting. The researcher distributed the PIS and received consent from the parents after explaining the study.
Healthcare providers and policymakers were recruited through professional contacts via telephone, email, Facebook Messenger, and WhatsApp to inform them about the study. A PIS and consent form were sent to each participant, and focus groups were conducted in a group. However, one healthcare provider and one policymaker were interviewed one‐on‐one as they were unable to attend their focus group because of their busy schedules. Focus groups Open‐ended questions were informed by the adapted Community‐Based Participatory Research (CBPR) model developed by Belone et al. [34]. Consumers' participation in research improves sustainability by promoting ownership of the programmes by local people. In the context of the CBPR model, this study examined the socio‐economic, cultural, community, and readiness context. This model has been implemented and recommended by previous research in developing sustainable mental health programs [35, 36]. Furthermore, this model aligns with the concept of connectedness and the SEM model, which is a guiding framework for this study. To facilitate discussion, a booklet was prepared outlining the main elements of the safeTALK™ programme, and a guide for the questions and topics to be discussed and sent to the participants as pre‐reading 2 weeks before the focus group's date (Supporting File 2). Focus groups lasted from 17 to 98 min (about 1.5 h) depending on the number of participants in the group (mean duration of 49 min).
Data Collection
3.8
The researcher travelled to the research site to arrange logistics for the data collection, and to recruit participants from 29 August to 13 September 2024.
Focus groups over Zoom™ were conducted in the Nepali language from Australia after the researcher returned from Nepal. A total of five focus groups were conducted from 15 September to 30 September 2024. Two experienced researchers (LR and DJ) were present to guide the novice researcher during the initial three focus groups.
To commence the focus groups, the researcher introduced herself and other research team members to the participants, welcomed them to the session, opened with icebreaker questions, and explained the ground rules. Then the researcher provided an overview of the LivingWorks safeTALK™ programme, paused in between the presentation, discussed questions, and moved forward with the presentation.
The focus group with adolescents was conducted via Zoom™ in the computer classroom of the school. All students were in the same location on a single call. There was a research support person present in‐person throughout the session to ensure the safety of adolescents if they experienced any distress. The research support person is a registered nurse in Nepal, who is competent in providing basic mental health support. The adolescents were informed they could have the choice of any preferred adult in the room during the focus group. However, they were comfortable in the focus group with the research support person. None of the adolescents required any kind of support throughout and after the session. One schoolteacher was also present for technical support and coordinated the session with students in a computer classroom at the school.
Ethics
3.9
This research is registered in the Australia New Zealand Clinical Trial Registry (ACTRN 12624000634572). Ethical approval was obtained from the Human Research Committee of Western Sydney University (H15955), and Nepal Health Research Council (372_2024). The focus groups were audio recorded, and all recordings were de‐identified before analysis to ensure confidentiality.
Data Analysis
3.10
Focus groups were transcribed manually, translated into English and checked by two independent bilingual persons. After transcribing and translating the data into the English language, the two independent bilingual persons checked the data for accuracy, cultural appropriateness and conceptual equivalence. Then data transcription files were uploaded to NVivo v.15 for analysis. A hybrid content analysis approach was used to analyse the data [37]. The process of analysis included audio recordings being listened to several times by the researcher before transcribing the data to allow familiarisation. Researchers read and re‐read the data independently. Initial coding was done line by line, considering both the SEM and the adapted CBPR model, allowing the deductive creation of pre‐determined categories within existing frameworks and inductive categories generated from the data. Final categories were then reviewed by all team members (RP, DJ, SPP and LR) before writing the results.
The analysis of participants' perspectives on the recommended socio‐cultural adaptations, informed the contextualisation and refinement of the LivingWorks safeTALK™ programme for future use among secondary school students in Nepal. All recommended modifications identified in this study were discussed with the Chief Executive Officer of LivingWorks Australia for approval.
Research Rigour
3.11
Four‐dimension criteria were followed to ensure the rigour of this study [38]. The four dimensions were credibility, dependability, confirmability, and transferability.
To maintain credibility, the interviewer was familiar with the setting, the interviewer was trained by expert researchers, and more than two team members with prior experience in conducting focus groups were present during the focus groups. All the focus groups were conducted by the same person using a predetermined guide developed by the team of experts. Dependability was ensured by maintaining an audit trail of the study methods, and confirmability was enhanced through the use of a reflexive journal and peer review of analytical decisions by the research team. To achieve transferability, researchers have provided detailed descriptions of the study context, data collection and data analysis process, with illustrative quotes reporting the study findings.
Findings
3.12
A total of 18 participants from the five groups participated in the focus groups (n = 7 adolescents, n = 2 teachers, n = 3 parents, n = 3 healthcare providers and n = 3 policymakers). The majority (55.55%) were female (Table 1). Data were analysed and presented as seven different categories and sub‐categories (Figure 2). Categories were based on the questions asked during focus groups (Supporting File 3). Exemplar quotes are presented in Table 2.
Categories and sub‐categories.
Categories
3.13
Category 1 Factors contributing to suicide in Nepal
Some participants expressed that there are many sociocultural factors and cultural practices in Nepal which can lead to an increased rate of suicide.
Individual and interpersonal factors: Participants discussed the following factors that could lead to suicide: Poverty and unemployment; romantic relationships, which are not accepted by their families; different types of violence faced by individuals; hormonal and bodily changes among adolescents; and academic pressures.
Community, social and cultural factors: There are prevailing superstitious beliefs among the community based around the hierarchal caste systems and gender bias at home, including child marriage and a preference for male children in some families. These problems could be exacerbated by dowry traditions and menstruation taboos. A few participants also identified excessive mobile phone use and changes to the traditional family structure as factors that could lead to experiences of suicidal thoughts.
Policy factors: Some policy factors regarding sexual and reproductive health contribute to stress and can be a risk factor for suicide. For example, there are challenges for young people obtaining contraceptives, such as condoms, oral contraceptive pills or injections and intrauterine devices, because they may be afraid that they will be judged by staff in the health centres. One policymaker explained that adolescents are commonly engaged in romantic relationships, which are hidden due to social stigma and are not accepted by families. If they become pregnant outside of marriage, society will not accept them, and for this reason, adolescents may attempt suicide due to shame. If policies could be changed to allow access to contraceptives, through adolescent‐friendly health services, regardless of their marital status, suicide could be prevented to some extent.
Category 2 The need for adolescent suicide prevention programmes in Nepal
All participants expressed that there is a need for a structured programme for adolescent suicide prevention, as many participants reported that suicide among adolescents is on the increase. Adolescent girls are attempting suicide at a higher rate, and if a preventive approach can be implemented, adolescents will be more aware about what to do and how to access appropriate help for suicidal thoughts early. This could potentially prevent many suicides in the future.
Category 3 Stigma around suicide in Nepal
Participants described how stigma surrounding mental health and suicide manifests in Nepalese society and how this stigma and shame are a barrier to timely help‐seeking and effective prevention.
Category 4 Attitude towards adolescent suicide and the safeTALK™ suicide prevention programme
The majority of participants discussed general community attitudes and perceptions towards suicide as not being positive. They stated that many people in the community say suicide is the act of a cowardly person who is incapable of doing anything productive with their life. They also explained their own and the community's perspectives on asking direct questions about suicidal ideation. A few participants expressed hesitation in asking someone direct questions about suicidal ideation, and one participant believed asking direct questions could increase the risk of suicide. Despite this, all participants had a positive attitude towards the safeTALK™ suicide prevention programme.
Category 5 Recommended modifications to the safeTALK™ programme
Most participants suggested modifications to three areas of the existing safeTALK™ programme before implementing it in Nepal‐Language, Context and Content. The required modifications were discussed with LivingWorks Australia, and the final approved modifications are presented in Supporting File 4. For example, Nepali subtitles were added to the videos and cartoon animations were created based on participants' suggestions.
Language: Most participants expressed that the current videos would be more effective in the Nepali language, and a few participants suggested that at least Nepali subtitles would be better than not having any Nepali language in the videos. Nepali subtitles were added with the help of an expert to the main videos, which conveyed the key messages.
Context: Some of the participants suggested producing videos that depict Nepali characters/people and settings in Nepal that show the sociocultural context of Nepal and would enhance the effective delivery of the programme. Two short animations were developed based on the cultural practices of Nepal (Supporting File 5).
Content: Although none of the participants suggested reducing or removing any of the existing content, they suggested adding some content related to the sociocultural risk factors for suicide in Nepal. For example, discussion of cultural practices specific to the local community, like menstruation taboos and hierarchical caste systems, were included in appropriate sections of the safeTALK™ programme and presented to LivingWorks Australia as a proposed and approved modification either to the content or during delivery. A few important minor modifications to the content were made during delivery, such as explaining the word “ * Invitations * ” during translation into the Nepali language. This was important because a few participants perceived the word as an invitation for suicide rather than for prevention, and participants felt it may be interpreted by adolescents in this way. A few participants also suggested that one should be careful in maintaining eye contact in conversations because it can be considered disrespectful and could be a barrier to effective communication in some cultures. One participant mentioned that the trainer's gender could influence the effectiveness of the training in certain communities. For example, if the suicide helper is male and is asking questions to a female, the participant may not be open to the helper. So, this factor was important to discuss during the delivery of the training (Supporting File 4).
Category 6 Readiness to implement an adolescent suicide prevention programme in Nepal
All participants stated that there was a need for a suicide prevention programme in Nepal, demonstrating the readiness of people from both the individual and community levels. Some participants expressed the need for strong policy recommendations to implement an adolescent suicide prevention programme.
Policy readiness: Participants discussed how the government of Nepal has set a target to reduce the suicide rate, but currently, there are no structured adolescent suicide prevention programmes in Nepal. All policymakers reported that an adolescent suicide prevention programme is required in Nepal. A strong policy recommendation from researchers could provide positive attitudes among all policymakers and related government agencies for developing national‐level guidelines and implementation of a suicide prevention programme.
Healthcare readiness: A few participants reported that training is required for healthcare providers and that healthcare infrastructure must improve to implement any innovative programmes. However, if there is strong evidence, recommendations can be incorporated into existing programmes.
Category 7 Challenges in implementing an adolescent suicide prevention programme in Nepal
All policymakers highlighted gaps in collaboration among different government sectors and agencies, emphasising the need for coordinated efforts from health, education, financial and social sectors to effectively prevent suicide. They also reported that the sustainability of the programme was another challenge due to poor intersectoral collaboration, financial constraints, human resources, and limited infrastructure. A few participants also identified individual beliefs and stigma as challenges to overcome in the implementation of any suicide prevention programme.
Discussion
4
This study aimed to contextualise the existing safeTALK™ programme for use among secondary school students in Nepal. Sociocultural adaptations necessary to reflect the local context prior to implementation of the programme were identified in relation to three areas: language, context and content. In the contextualisation of a programme, suicidal issues such as risk factors and attitudes can vary across different sociocultural contexts. Cultural factors need to be considered in adolescent suicide [39, 40]. For example, Eastern Asian adolescents may attempt suicide due to shame in not meeting expectations of family or others, and acculturative stress is associated with high suicides among Latin American adolescents when they are living outside their home countries [39]. Additionally, cultural considerations may affect help‐seeking [41]. Therefore, some modifications seem important to consider before implementing a suicide prevention programme, such as safeTALK™, in a new setting to make it culturally appropriate for Nepal.
Suicide is a public health issue, and it requires a multi‐sectoral approach to its prevention. Therefore, this study used the Socio Ecological Model (SEM) as a guiding framework [25]. Guided by the SEM, this study involved stakeholders across multiple levels to contextualise the programme. Adolescents were intentionally positioned as the core stakeholders at the individual level through to policy level officers. This multi‐layered approach provided a rich understanding of diverse viewpoints.
The Lancet reported that there are multiple examples of the successes and challenges of using a public health model in preventing suicide globally [42]. Our study also reported different social and cultural perspectives, particularly in the Nepalese and South Asian context. For instance, non‐mainstream topics related to Nepali context in our study including the hierarchal caste system, untouchability, dowry tradition, and Chhaupadi or other forms of menstrual taboo (which all contribute to suicide in Nepal) can be learning opportunities for people with a limited understanding of the cultural nuances of Nepal and other South Asian countries and can also can be beneficial to future researchers or programme developers in South Asia to understand the importance of contextualisation.
For many people in South Asia, particularly in Nepal and India, the caste system plays a significant role in social exclusion [43]. The system consists of four main categories: “Brahmins,” priests; “Kshatriyas,” warriors; “Vaishyas,” merchants; and “Sudras,” servants. Below these groups are the Dalits, often referred to as the “untouchables.” Caste‐based discrimination remains a highly sensitive and politically charged issue in Asia. Nepal has attempted to combat caste discrimination by enacting laws that declare caste‐based discrimination a crime. However, discrimination persists in Nepali society, especially in rural areas, and includes behaviours such as refusing to enter Dalits' houses or allowing them to enter your house. Also, sharing food and water and refusing to touch people who are Dalits are common [43]. People who face daily discrimination can also experience mental stress, sometimes leading to suicide. These factors must be taken into account when adapting or tailoring a programme for use in another country to ensure contextual relevance and effectiveness.
Another significant factor contributing to suicide among South Asian girls and women is the dowry dispute [44], which was identified in the focus groups as a possible reason for girls and women to consider suicide. Participants in our study highlighted this issue to be discussed in the safeTALK™ prevention programme. Provision of a dowry is a common cultural practice in some communities of South Asian countries, where the groom's family expects money and valuable items from the bride's side, and this expectation brings the bride's family under extreme pressure. If expectations are unmet, different types of family violence against the woman may continue for many years after the marriage [44]. This can be a significant contributor to poor mental health and a higher rate of suicide among females in the South Asian context [44]. Therefore, gender‐based prevention strategies are recommended in Nepal.
A typical cultural practice observed in Western Nepal is Chhaupadi or menstrual exclusion [45]. However, different forms of menstruation taboo exist among Hindu communities throughout Nepal [45, 46]. Menstrual exclusion, such as ‘Chhaupadi’, is an extreme form of ‘untouchability’ in far‐western Nepal. Women and girls who are menstruating are forbidden from touching other people and objects, and are required to live away from the community, typically in cattle sheds, during menstruation. Despite being a crime under Nepali law, this tradition continues due to community‐based values, social beliefs and religious practices. Similar practices are common across many countries of South Asia, and they have multidimensional negative effects on the lives of girls and women and affects their mental health [45, 46]. This practice not only prevents them from participating in normal daily activities but also increases their risk of robbery and sexual assault during this period of menstrual exclusion. Therefore, suicide prevention programmes developed for such communities should also consider these issues.
Additionally, other cultural practices and superstitions need to be considered in the design and delivery of suicide prevention programmes for Nepalese society. Participants cited factors such as community preference to a male child and pressure on women to give birth to males. There are also superstitious beliefs among the community, including witchcraft practices. An accusation of witchcraft is one of the serious forms of violence in Nepal, especially with females [47]. Many experience serious physical injury and die due to physical abuse received by the people in the community. Such types of practices subject the victims and their families to profound distress, and they are often at high risk of suicide. Therefore, minor modifications were made to the existing safeTALK™ programme, so that typical Nepalese practices could be discussed during programme delivery and during group activities. However, further contextualisation may be required for the Nepalese context to address the diverse needs of the population.
In addition to cultural adaptation, language and contextual issues were raised by the participants. Language and nonverbal communication are also linked to culture. Language provides a strong sense of self‐identity, and of being connected to the community. Presenting suicide prevention programmes in the local language may promote connectiveness for young people to the programme. This should increase the acceptability and effectiveness of suicide prevention strategies [48]. To address language issues in the existing programme, the research team added Nepali subtitles to the English videos and planned for the trainer to translate and deliver all the training in the Nepali language. Furthermore, to address the contextual issues, we prepared two animations based on the cultural and contextual practices in Nepal. In addition, we included an explanation of the meaning of the word INVITATION used in the training package so that it delivered the intended message of the programme, as participants were concerned that adolescents might interpret the word in a way that is opposite to the intended meaning. During translation, the literal translation may not always deliver the intended message. We also incorporated an explanation of how to adjust the context of the programme to consider specific gender issues when asking questions in certain communities in Nepal. In some communities of Nepal, if the suicide helper belongs to the same gender of the person experiencing the problem, they can be more open to communication and feel more comfortable with the helper, leading to positive outcomes.
One participant also expressed that asking direct suicide questions can increase suicide; however, a previous study did not report any iatrogenic effects of direct questions [49]. This is an example of the prevalent myths around suicide in the community. The LivingWorks safeTALK™ programme has provided guidelines about asking direct questions when an invitation suggests someone is reaching out for support because they are experiencing suicidal thoughts.
Other adjustments included accommodating cultural differences, such as minimising eye contact during active listening to avoid feelings of being threatened in certain communities. In Nepal, maintaining too much eye contact is considered rude, while this is generally considered an active listening technique in Western cultures [50]. In addition, we replaced the existing list of numbers in the KeepSafe™ connections to local numbers for Nepal.
While participants expressed a clear and evident need for an adolescent suicide prevention programme in Nepal, there are a variety of challenges to overcome. The first challenge is working in a country where there are no policies and definite guidelines for suicide prevention. This makes it challenging to gain the trust of the community and service consumers to implement or test a new programme. National policies can be associated with accountability, and accountability is associated with public trust [51]. Other factors include stigma, or a negative attitude towards prevention programmes due to inadequate awareness and the prevalence of myths around suicide. Stigma is also associated with decreased help‐seeking [52]. Another major challenge is financial constraints in resource‐poor settings, especially when there is negligible government expenditure on health, and where the emphasis is on a curative rather than a preventive approach. Other challenges are the disparity between awareness levels of people from various parts of the country, huge economic variability, poverty and geographical difficulties to reach certain population groups. Despite various challenges, there are many opportunities for researchers and policymakers to work in this space. While previous studies implemented and evaluated the effectiveness of this programme, it was not contextualised to the Nepalese context [7, 15, 17, 21]. Although further work is needed before full implementation, piloting the contextualised version in the Nepalese community provides an important first step.
Strengths and Limitations of the Study
5
This study is the first to explore the needs of a community and to contextualise the safeTALK™ programme for use among secondary school students in Nepal and the first documented study to contextualise an existing programme for adolescent suicide prevention in LMICs. By involving multiple stakeholders, including adolescents, the robustness of this study and acceptance within the local community was enhanced. This study gives voice to the community, and led to dialogue and learning, and participatory decision‐making, reflected in the recommendations for the contextualised version of the safeTALK™ programme. However, limitations include that the study was based on the urban area of eastern Nepal, and therefore, it may not address the cultural complexities of suicide affecting populations in other areas and indigenous communities. Furthermore, a larger and more diverse participant pool, combined with extended time for deeper focus group interaction, could have enhanced the analytic breadth of the findings. Another limitation was not being able to modify certain parts of the safeTALK™ programme for future implementation because of resources constraints and copyright issues. For example, while participants recommended changes to the people featured and the contextual scenarios depicted in the existing videos, these modifications were not possible. As an alternative, in addition to the existing videos, we produced two short animations for future implementation (Supporting File 5).
Implications for Policy and Practice
6
This study has highlighted the need for adolescent suicide prevention policy guidelines and programmes in Nepal and other LMICs. More importantly, this study has highlighted the importance of contextualisation of programmes before implementation, to promote equity and relevance at the policy level, and the potential for improved engagement, uptake and sustainability within the local culture. To date, there are no national‐level adolescent suicide prevention strategies or policies documented in Nepal. Implementation of this programme in schools, as part of a broader suicide prevention strategy, teaches people to be alert and supports the connection of people experiencing suicidal thoughts to helping resources. It is an important part of a community's efforts to reduce suicide and should contribute to a national policy for adolescent suicide prevention in Nepal.
Recommendations for Further Research
7
Using a rigorous programme development methodology, the contextualised version should first be tested against the standard version and the learning outcomes compared. If, as hypothesised, it demonstrates better outcomes, implementation would be warranted, followed by evaluation of programme effectiveness. Although significant work is needed before recommending full implementation, piloting the contextualised version presents an opportunity to generate baseline evidence in Nepal.
Conclusion
8
This study is the first to gather stakeholder perspectives to contextualise an existing structured suicide prevention programme for adolescents in Nepal. While all factors in the existing LivingWorks safeTALK™ programme remained the same, minor additions were made based on this study's findings prior to implementing and pilot testing the programme in a public school in Eastern Nepal. Suicide prevention is a major issue and requires further research to develop a culturally appropriate suicide prevention programme, especially among at‐risk adolescents in Nepal. This early evidence provides a critical foundation for subsequent, larger‐scale qualitative and mixed methods studies that can further refine, challenge, or extend the themes identified in this exploratory study.
Author Contributions
Rita Pokharel Poudel: conceptualisation, methodology, data collection, data analysis, writing – original draft. Diana Jefferies: conceptualisation, methodology, focus groups, validation, writing – review and editing. Sheeja Perumbil Pathrose: conceptualisation, methodology, data analysis, writing – review and editing. Peter M. Gutierrez: writing – review and editing. Lucie M. Ramjan: conceptualisation, methodology, focus groups, validation, data analysis, writing – review and editing, supervision. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no specific funding for this work.
Ethics Statement
This study was approved by the Western Sydney University Human Research Ethics Committee (H15955) and Nepal Health Research Council (372_2024).
Conflicts of Interest
Peter M. Gutierrez is an Executive at LivingWorks, but did not participate in the design, implementation, data analysis, or interpretation of the study. Their only involvement was in providing critical revisions to the final manuscript. The other authors declare no conflicts of interest
Supporting information
Supplementary_file_1_COREQ_Checklist.
Supplementary_file_2_Booklet.
Supplementary_file_3_Focus_group_questions.
Supplementary_file_4_Approved_modifications.
Supplementary_file_5_Animation_videos.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1G. Bhandari , L. Nath , P. R. Bhatt , R. Mishra , and A. Bhatt , “Exploring Trends: Five‐Year Analysis of Suicide Rates in Nepal,” Mental Illness 2024, no. 1 (2024): 5396303, 10.1155/2024/5396303. · doi ↗
- 2A. R. Pandey , B. Bista , R. R. Dhungana , K. K. Aryal , B. Chalise , and M. Dhimal , “Factors Associated With Suicidal Ideation and Suicidal Attempts Among Adolescent Students in Nepal: Findings From Global School‐Based Students Health Survey,” P Lo S One 14, no. 4 (2019): e 0210383, 10.1371/journal.pone.0210383.31002715 PMC 6474648 · doi ↗ · pubmed ↗
- 3R. H. Aseltine, Jr. , A. James , E. A. Schilling , and J. Glanovsky , “Evaluating the SOS Suicide Prevention Program: A Replication and Extension,” BMC Public Health 7 (2007): 161, https://ezproxy.uws.edu.au/login?url=http://ovidsp.ovid.com/ovidweb.cgi?T=JS&CSC=Y&NEWS=N&PAGE=fulltext&D=med 6&AN=17640366.17640366 10.1186/1471-2458-7-161PMC 1941734 · doi ↗ · pubmed ↗
- 4E. A. Schilling , R. H. Aseltine , and A. James , “The SOS Suicide Prevention Program: Further Evidence of Efficacy and Effectiveness,” Prevention Science 17, no. 2 (2016): 157–166, 10.1007/s 11121-015-0594-3.26314868 · doi ↗ · pubmed ↗
- 5E. A. Schilling , M. Lawless , L. Buchanan , and R. H. Aseltine, Jr. , “Signs of Suicide’ Shows Promise as a Middle School Suicide Prevention Program,” Suicide and Life‐Threatening Behavior 44, no. 6 (2014): 653–667, 10.1111/sltb.12097.24796660 · doi ↗ · pubmed ↗
- 6D. Wasserman , C. W. Hoven , C. Wasserman , et al., “School‐Based Suicide Prevention Programmes: The SEYLE Cluster‐Randomised, Controlled Trial,” Lancet 385, no. 9977 (2015): 1536–1544, 10.1016/S 0140-6736(14)61213-7.25579833 · doi ↗ · pubmed ↗
- 7E. Bailey , M. J. Spittal , J. Pirkis , M. Gould , and J. Robinson , “Universal Suicide Prevention in Young People: An Evaluation of the safe TALK Program in Australian High Schools,” Crisis 38, no. 5 (2017): 300–308, 10.1027/0227-5910/a 000465.29098895 · doi ↗ · pubmed ↗
- 8A. L. Calear , M. Banfield , P. J. Batterham , et al., “Silence Is Deadly: A Cluster‐Randomised Controlled Trial of a Mental Health Help‐Seeking Intervention for Young Men,” BMC Public Health 17, no. 1 (2017): 834, https://ezproxy.uws.edu.au/login?url=http://ovidsp.ovid.com/ovidweb.cgi?T=JS&CSC=Y&NEWS=N&PAGE=fulltext&D=med 14&AN=29061168.29061168 10.1186/s 12889-017-4845-z PMC 5653993 · doi ↗ · pubmed ↗