The Subtle Pattern of Sinoatrial Wenckebach
Laith Alomari, Olayinka Adebolu, Abiodun Idowu, Ola Khraisha

TL;DR
This paper presents a case of rare SA Wenckebach arrhythmia, highlighting its ECG pattern and clinical management.
Contribution
The case emphasizes the importance of distinguishing SA Wenckebach from other arrhythmias for accurate diagnosis.
Findings
SA Wenckebach showed grouped beating on ECG with noncompensatory pauses.
Discontinuing nodal blockers resolved the arrhythmia without pacemaker implantation.
The case highlights the need for careful ECG interpretation to avoid misdiagnosis.
Abstract
Second-degree sinoatrial (SA) exit block type I, or SA Wenckebach, is a rare arrhythmia marked by progressively shortening P–P intervals followed by a dropped P wave and a noncompensatory pause, producing a grouped beating pattern on electrocardiogram (ECG). A 64-year-old male with multiple comorbidities presented after a mechanical fall with bradycardia. ECG revealed a new SA exit block type I. Echocardiography showed preserved ejection fraction and grade II diastolic dysfunction. Nodal blockers were discontinued, and pacemaker implantation was deemed unnecessary. Recognizing SA exit block is important, as it can mimic atrioventricular block or sinus arrhythmia on ECG.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
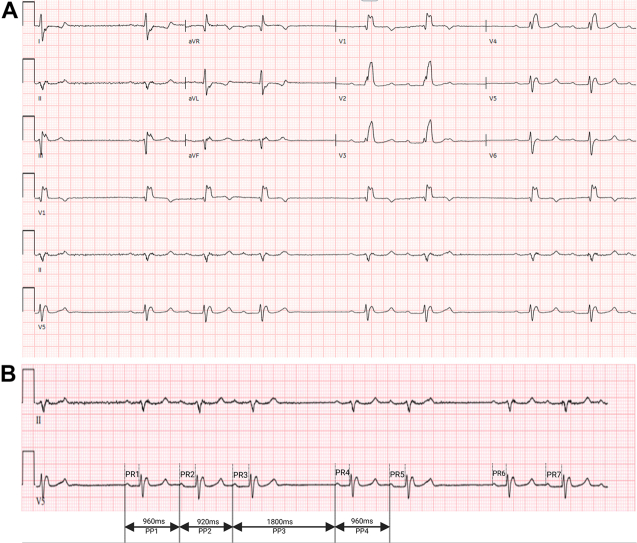 Figure 1
Figure 1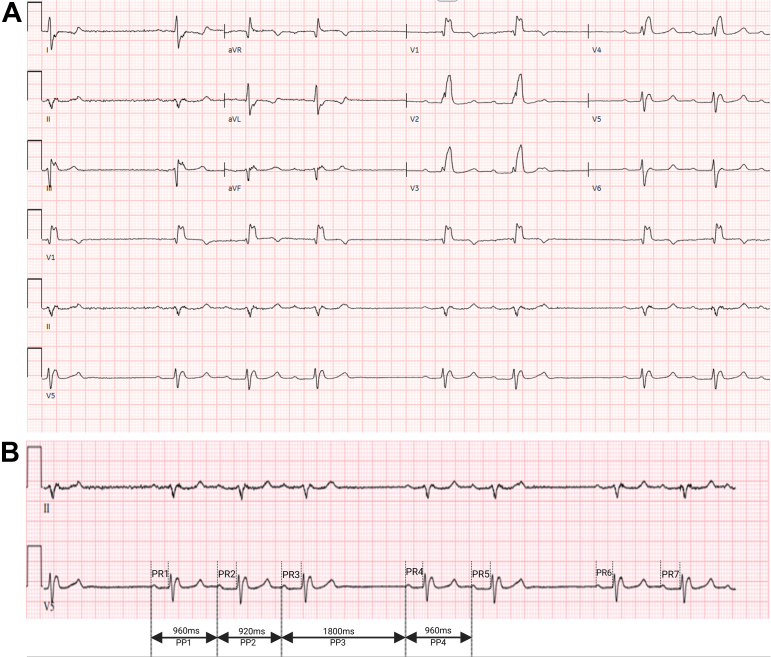 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Arrhythmias and Treatments · Cardiac pacing and defibrillation studies · Cardiac electrophysiology and arrhythmias
History of Presentation
A 64-year-old male presented to the emergency department following a mechanical fall. His medical history included type 2 diabetes mellitus, end-stage renal disease status post kidney transplant, coronary artery disease with prior coronary artery bypass grafting (left internal mammary artery–left anterior descending artery, saphenous vein graft–first obtuse marginal artery, saphenous vein graft–posterior descending artery), heart failure with preserved ejection fraction, chronic right bundle branch block, and first-degree atrioventricular (AV) block. On examination, his heart rate was 45 beats/minute, blood pressure 150/90 mm Hg, and oxygen saturation 100% on room air. The remainder of the physical exam was unremarkable. An electrocardiogram (ECG) was obtained (Figure 1).Take-Home Messages
- •Second-degree sinoatrial exit block type I presents with progressively shortening P–P intervals, a dropped P-wave, and a noncompensatory pause.
- •It may mimic atrioventricular block or sinus arrhythmia; accurate diagnosis requires close attention to P–P interval.
- •Conservative management is appropriate for asymptomatic patients, with medication review and electrophysiology follow-up. Figure 1ECG on Presentation(A) ECG on presentation. (B) Rhythm strip showing progressively shortening P–P intervals, followed by a dropped P-wave and a resulting noncompensatory pause.
Current medications included metoprolol tartrate 50 mg twice daily, atorvastatin, ezetimibe, tacrolimus, prednisone, mycophenolate mofetil, patiromer, and insulin. Laboratory results showed hemoglobin 13.3 g/dL, potassium 5.2 mmol/L, creatinine 1.8 mg/dL, blood urea nitrogen 48 mg/dL, thyroid-stimulating hormone 2 mIU/L, high-sensitivity troponin I 128 ng/dL, and brain natriuretic peptide 388.8 pg/mL.
Question
In addition to the baseline right bundle branch block, what is the most likely cardiac rhythm on the ECG?
- A.Second-degree atrioventricular block, Mobitz type I
- B.Second-degree atrioventricular block, Mobitz type II
- C.Second-degree sinoatrial exit block type I
- D.Second-degree sinoatrial exit block type II
Discussion and Rationale
Choice A is incorrect. Mobitz type I AV block shows progressive PR interval prolongation before a dropped QRS complex. In this ECG, the PR intervals after the pause (PR1, PR4, and PR6) are 242 ms, while the other PR intervals (PR2, PR3, PR5, and PR7) are 272 ms. However, dropped P wave (not a QRS complex), grouped beating pattern, progressive PP interval shortening, and noncompensatory pause are inconsistent with AV Wenckebach.
Choice B is incorrect. Mobitz type II AV block presents with unexpected QRS drops after normal P waves. This ECG shows dropped P waves, indicating failure of impulse exit from the sinoatrial (SA) node.
Choice C is correct. The ECG displays a grouped P–QRS pattern, progressively shortening P–P intervals, and a dropped P-wave, followed by a noncompensatory pause (pause following the dropped P wave is not a multiple of the basic P–P interval). The postpause P–P interval is longer than the preceding one, consistent with second-degree SA exit block type I (SA Wenckebach).
Choice D is incorrect. SA exit block type II features fixed P–P intervals with sudden, dropped P waves. The pause is typically an exact multiple of the basic P–P interval, which is not observed here.
The SA node contains pacemaker (P) cells and transitional (T) cells. SA exit block occurs when impulses generated by P cells fail to exit through T cells.1 There are 3 degrees of SA exit block. First-degree SA block is not detectable on surface ECG. Second-degree SA block type I (SA Wenckebach): conduction delay progressively increases until an impulse fails to exit, producing the classic grouped beating. Second-degree SA block type II: impulses fail intermittently without prior P–P interval changes. Third-degree SA block results in complete conduction failure and is indistinguishable from sinus arrest on ECG. SA Wenckebach also contrasts with sinus arrhythmia, which features irregular but nonprogressive P–P variability and no dropped P waves.
Clinically, second-degree SA exit block type I is often benign and asymptomatic. In such cases, pacemaker implantation is not indicated. Management should focus on identifying reversible contributors, such as beta-blocker use, and arranging electrophysiology follow-up.2
Funding Support and Author Disclosures
Publication made possible in part by support from the Thomas Jefferson University Open Access Fund. The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Manoj P.Kim J.A.Kim S.Sinus node dysfunction: current understanding and future directions Am J Physiol Heart Circ Physiol 32432023 H 259H 27810.1152/ajpheart.00618.202236563014 PMC 9886352 · doi ↗ · pubmed ↗
- 2Petzl A.M.Epstein A.E.Guandalini G.S.Less obvious than one might think: why is there grouped beating?Circulation 1496202448148310.1161/CIRCULATIONAHA.123.06825238315765 · doi ↗ · pubmed ↗