Testing to Detect Candida auris Colonisation After Intrahospital Transfer From an Endemic Area, a Prospective Observational Study
Laura Mezzogori, Martina Bavastro, Laura Magnasco, Federica Centorrino, Riccardo Schiavoni, Federica Portunato, Daniele Roberto Giacobbe, Antonio Vena, Vincenzo Di Pilato, Ramona Barbieri, Andrea Orsi, Giancarlo Icardi, Anna Marchese, Matteo Bassetti, Malgorzata Mikulska

TL;DR
This study examines how to detect Candida auris colonization in patients transferred from high-risk areas to other hospital wards, finding that a single test is insufficient and repeated screening is needed.
Contribution
The study provides evidence-based recommendations for the timing and number of screening swabs needed to detect Candida auris colonization after hospital transfer.
Findings
A single negative screening test at discharge is insufficient to exclude Candida auris colonization.
16.3% of sufficiently screened patients tested positive for Candida auris after transfer.
Repeated screening within the first 2 weeks post-transfer is essential to prevent further transmission.
Abstract
Current international guidelines lack clear recommendations on the management of non‐colonised patients undergoing intra‐hospital transfer from the ward in which horizontal transmission of Candida auris is known to occur (defined as endemic for Candida auris) to wards with no horizontal transmission detected (defined as non‐endemic wards), particularly regarding the timing and number of screening swabs needed to exclude colonisation. Single‐center prospective observational study at a tertiary‐care hospital in Genoa, Italy, including adults transferred from the C. auris endemic‐ICU (eICU) to non‐endemic wards between January and December 2024. Patients who tested negative for C. auris colonisation both at eICU admission and at transfer, and who had ≥ 1 screening swab performed post‐transfer, were included. Swabs (bilateral axilla/groin) were performed on Days 0–1, 2–3 after…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
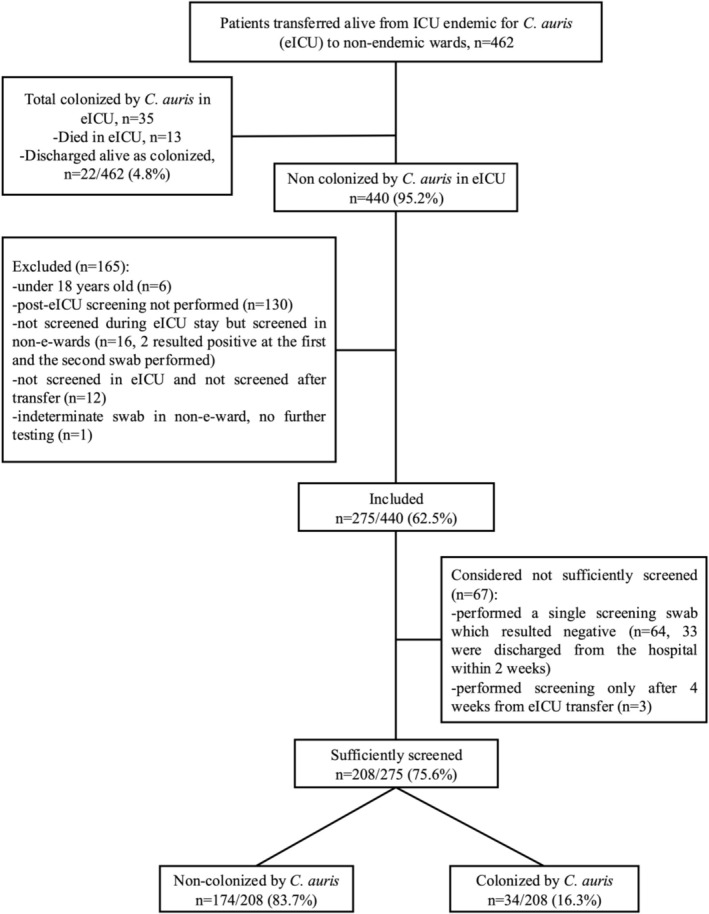 FIGURE 1
FIGURE 1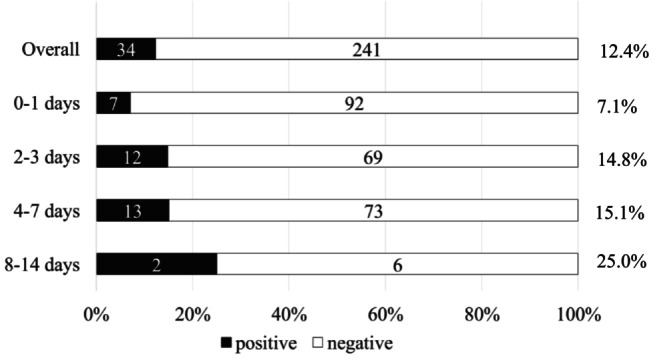 FIGURE 2
FIGURE 2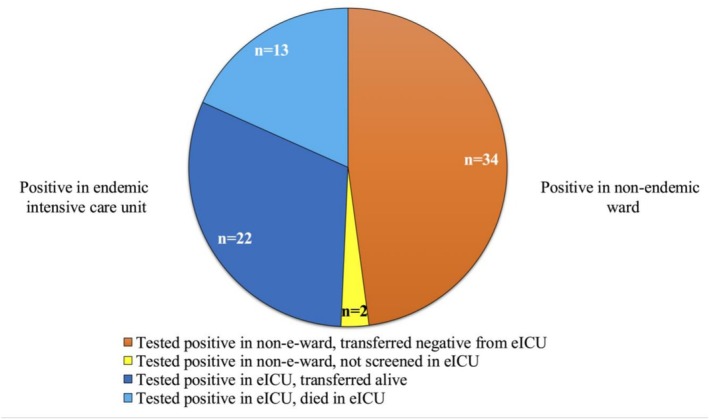 FIGURE 3
FIGURE 3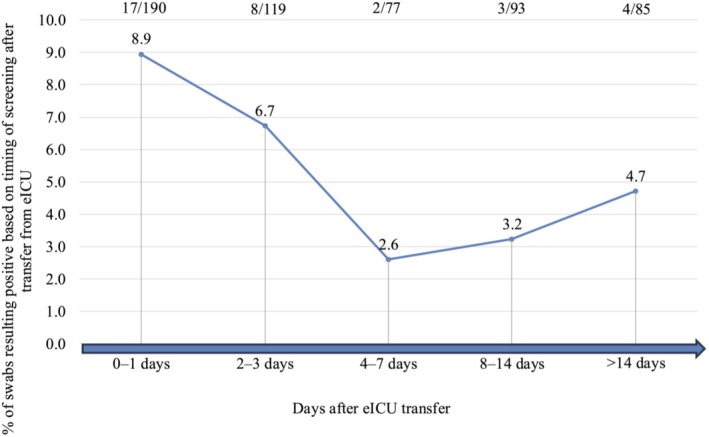 FIGURE 4
FIGURE 4| Overall, | Sufficiently screened, | Negative, | Positive, |
| |
|---|---|---|---|---|---|
|
| |||||
| Male sex, | 155 (56.4) | 127 (61.1) | 103 (59.2) | 24 (70.6) | 0.213 |
| Age (years), median (IQR) | 65 (54.5–75) | 65 (54.8–74.5) | 64.5 (55.3–74) | 65.6 (50.5–73) | 0.893 |
|
| |||||
| eICU length of stay | 5 (2.3–11.8) | 5.5 (2.5–19.1) | 5 (2.2–12.8) | 6 (3.5–14) | 0.309 |
| post eICU length of stay | 20 (12.5–39) | 23 (13.4–43.2) | 22 (13.1–39) | 32 (14.7–52) | 0.116 |
|
| 0.671 | ||||
| Medical | 112 (40.7) | 84 (40.4) | 69 (39.7) | 15 (44.1) | |
| Abdominal surgery | 38 (13.8) | 28 (13.5) | 25 (14.3) | 3 (8.8) | |
| Other surgery | 125 (45.5) | 96 (46.1) | 80 (46.0) | 16 (47.1) | |
|
| 0.414 | ||||
| Neurosurgery | 46 (16.7) | 43 (20.7) | 33 (19.0) | 10 (29.4) | |
| Other surgery | 88 (32.0) | 64 (30.8) | 55 (31.6) | 9 (26.5) | |
| Medicine | 121 (44.0) | 85 (40.8) | 71 (40.8) | 14 (41.2) | |
| Rehabilitation | 12 (4.4) | 11 (5.3) | 11 (6.3) | 0 (0.0) | |
| Other non‐endemic ICU | 8 (2.9) | 5 (2.4) | 4 (2.3) | 1 (2.9) | |
| Number of negative swabs performed in the eICU, median (IQR) | 1 (1–2) | 1 (1–2.5) | 1 (1–3) | 1 (1–3) | 0.825 |
| Last swab performed within 3 days from discharge, | 180 (65.4) | 132 (63.5) | 113 (64.9) | 19 (55.9) | |
| Last swab performed within 2 days from discharge, | 145 (52.7) | 106 (51.0) | 93 (53.4) | 13 (38.2) | |
| Last swab performed within 1 day from discharge, | 99 (36.0) | 73 (35.1) | 66 (37.9) | 7 (20.6) | |
|
| |||||
| Discharged from hospital alive, | 264 (96.0) | 199 (95.7) | 166 (95.4) | 33 (97.1) | 0.664 |
| Variable | Overall, | Positive in eICU, | Positive in non‐e‐ward, |
|
|---|---|---|---|---|
|
| ||||
| Male sex, | 51 (73.9) | 27 (68.6) | 24 (70.6) | 0.535 |
| Age (years), median (IQR) | 65 (56–73) | 63 (56–72) | 65.6 (50.5–73) | 0.778 |
| eICU lengh of stay (days), median (IQR) | 14 (5.9–26) | 21 (14–51.5) | 6 (3.5–14) | < 0.001 |
| Time to colonisation following admission to the eICU (days), median (IQR) | — | 9 (6–20) | — | — |
| Time to colonisation following eICU discharge (days), median (IQR) | — | — | 1.5 (1–6) | — |
| Other colonisation sites, | 13 (18.8) | 9 (25.7) | 4 (11.8) | |
| Urinary tract | 8 (11.5) | 5 (14.3) | 3 (8.8) | 0.506 |
| Respiratory tract | 6 (8.7) | 4 (11.4) | 2 (5.9) | 0.853 |
|
| ||||
| Discharged from hospital alive, | 52 (75.4) | 19 (54.3) | 33 (97.1) | 0.002 |
| Variable | Candidemia in patients colonised in non‐e‐ward | Candidemia in patient colonised in eICU | |||
|---|---|---|---|---|---|
| Patient | 1 | 2 | 3 | 4 | 5 |
| Sex | Male | Male | Female | Male | Male |
| Age, years | 75 | 74 | 88 | 65 | 41 |
| Charlson comorbidity index | 3 | 6 | 6 | 4 | 1 |
| Reason for admission to eICU | Polytrauma with spinal cord injury | Cranial trauma with acute subdural hematoma | Cranial trauma with acute subdural hematoma | Cholecystitis after chemotherapy | Recurrent pulmonary embolism |
| eICU length of stay, days | 8 | 57 | 8 | 5 | 73 |
| Time from eICU discharge to detection of colonisation, days | 1 | 3 | 1 | 3 |
Not applicable Days from eICU admission to colonisation: 11 |
| Time from colonisation to candidemia, days | 2 | 29 | 49 | 50 | 15 |
| Other colonisation sites | None | None | None | Respiratory and urinary tract | Respiratory tract |
| Time from candidemia to death, days | — | 155 | 124 | 42 | — |
| Comments | Repeated ICU and non‐ICU ward transfer; multiple infectious complications and their treatment; second episode of | Repeated hospitalizations due to cardiac, neurological and infectious complications. Death due to | Repeated antibiotic therapies; recurring seizures; transferred alive to long term care facility. | Repeated hospital admissions for treatment of cerebral lymphoma; death due to lymphoma progression | Discharged alive from ICU 47 days after candidemia onset |
- —Gilead Sciences10.13039/100005564
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Antibiotic Use and Resistance · Antibiotic Resistance in Bacteria
Introduction
1
The World Health Organization [1] and the Centers for Disease Control and Prevention [2] have included Candida auris among the highest‐priority fungal pathogens of public health concern.
The ability of C. auris to persist on the skin for prolonged periods [3], combined with its capacity to spread through contact with contaminated surfaces or direct skin‐to‐skin transmission, facilitates its dissemination within healthcare settings [4]. An estimated 5%–25% of colonised individuals progress to invasive infections, which are often associated with high mortality rates [5, 6, 7].
C. auris cases have to date been documented in over 50 countries across six continents [4, 8]. In most countries [9, 10, 11, 12, 13, 14, 15, 16], its dissemination peaked during the COVID‐19 pandemic in 2020. Prolonged hospital stays, underlying comorbidities, use of broad‐spectrum antibiotics, immunosuppressive therapy, mechanical ventilation, and the presence of indwelling urinary and intravenous catheters facilitated the persistence of C. auris specifically in intensive care units (ICU) [17, 18, 19]. Moreover, beyond patient‐related risk factors, the pandemic may have influenced infection prevention and control measures facilitating the spread of the pathogen [19, 20]. Notably, repeated outbreaks of C. auris in long‐term care facilities contribute to its persistence and transmission [21].
In our hospital, an outbreak of C. auris was recorded during the COVID‐19 pandemic [22], with more than 90% of all new C. auris cases occurring in two of five ICUs, where horizontal transmission of C. auris continued despite strict infection control measures, even though the rate of patients acquiring colonisation during ICU stay decreased overtime. We defined these ICUs as endemic for * C. auris
- (eICU), and one of them was closed after the pandemic's resolution [6]. A similar confined distribution of cases of C. auris transmission has been observed in Greece, with a long‐lasting outbreak occurring in selected ICUs within a tertiary care hospital [23].
Although some recommendations exist for C. auris outbreak prevention, current guidelines often lack specific indications regarding screening practices. Most protocols focus on patients admitted from known endemic facilities or with known risk factors for colonisation, but do not clearly address the management of patients transferred within the same hospital from an endemic unit to a non‐endemic one, particularly when a prior negative screening is performed immediately before transfer.
In response to the outbreak in our hospital, an internal screening protocol was introduced in 2020 and subsequently refined to enhance post‐transfer testing from eICU.
While cutaneous swabbing is widely recommended, there is no consensus on the optimal number, anatomical site, or timing for testing. Practices vary significantly: some protocols suggest three swabs taken 24 h apart, others recommend screening with one swab upon admission followed by weekly tests, but in many cases, testing intervals remain undefined [24, 25, 26, 27, 28]. Similarly, the optimal duration of preventive contact precautions after negative screening results remains unclear. Understanding the optimal screening protocols and isolation practices for patients at risk is crucial to minimize undetected colonisation and limit further transmission of C. auris within healthcare facilities.
Our study aimed to investigate the optimal duration and frequency of screening for C. auris colonisation in patients transferred as non‐colonised from eICU.
Materials and Methods
2
Study Design and Objectives
2.1
This was a single‐center, prospective study conducted at a tertiary‐care medical center in Genoa, Italy, from January 1st, 2024, to December 31st, 2024. Follow up of patients transferred in the late months of 2024 was extended up to the end of March 2025.
The primary objective of this study was to investigate the optimal frequency and duration of screening for C. auris colonisation in patients transferred as non‐colonised from the only eICU. Indeed, of two eICUs in our institution, one caring specifically for COVID‐19 patients had been closed after the end of the pandemic and was no longer in use during the study period. The secondary objective was to evaluate the prevalence of C. auris candidemia in colonised patients during the study period.
For the primary objective, inclusion criteria were: age ≥ 18 years, transferred alive from eICU, at least one negative screening performed in the eICU, and at least one screening performed in a non‐endemic ward.
All patients included in this analysis had tested negative for C. auris colonisation at all screenings performed during their eICU admission, allowing the evaluation of new colonisation events occurring after transfer to non‐endemic wards.
For the secondary objective, we identified all colonised patients during the study period who developed C. auris candidemia.
Definitions and Screening Protocols
2.2
Colonisation with Candida auris was defined as its detection in cutaneous swabs performed in axillae and groin bilaterally (with molecular and/or conventional culture techniques), as well as in urine and/or respiratory samples (tracheal aspirates or bronchoalveolar lavage samples for patients undergoing mechanical ventilation). Whenever C. auris was detected from non‐cutaneous sites, molecular cutaneous swabs were also performed to assess skin colonisation.
Screening for cutaneous colonisation was performed using a commercially available real‐time PCR assay (Progenie Molecular, Spain).
C. auris candidemia was defined as the isolation of C. auris from blood cultures (MALDI‐TOF MS—VITEK MS; bioMe'rieux, Marcy‐l'Etoile, France), identified using VITEK MS v4.0 software.
According to local screening protocol, introduced in 2020, patients admitted to all ICUs in our hospital underwent weekly screening to monitor C. auris colonisation status. eICU was the only ICU (among the 4 ICUs serving our hospital during the study period) with ongoing C. auris transmission, characterised by a sustained detection of new cases of colonisation over time. No other wards outside that eICU were considered endemic in our institution. Importantly, this eICU continued to admit all individuals according to clinical needs, but given a possibility of horizontal transmission, all admitted patients were repeatedly screened (at admission, weekly and at discharge) according to the institutional infection control protocol.
Patients were transferred from the eICU to non‐endemic wards when clinically stabile, regardless of their C. auris colonisation status. Upon transfer, those who had tested negative for C. auris colonisation during eICU stay underwent additional screening before eICU discharge and continued screening after admission to other hospital wards, with swabs collected at days 0–1, 2–3, and subsequently on a weekly basis for up to 4 weeks or until hospital discharge. This approach allowed the detection of new colonisation events occurring after transfer to non‐endemic wards (primary endpoint of the study). Contact precautions were also applied until at least 2 negative screening results were obtained.
Screening performed in non‐endemic wards was considered “sufficient” if at least two swabs were collected within the first 4 weeks after eICU transfer or if colonisation was detected at the first control swab.
Data Collected for the Analysis
2.3
Clinical and microbiological data were retrieved from electronic medical records. Transfers from eICU to non‐endemic wards were tracked using locally implemented business intelligence software for data integration and analysis. Screening data were reviewed at least twice weekly throughout the study period.
The Charlson Comorbidity Index [29] was recorded to assess baseline comorbidity.
Non‐endemic wards were contacted by phone by study personnel to improve adherence to the screening schedule.
Statistical Analysis
2.4
Categorical variables were summarised with numbers and percentages, and continuous variables with median and interquartile range. Two‐tailed p values were considered significant if ≤ 0.05. All analyses were performed with SPSS v.21.0 (IBM, Armonk, NY, USA).
Ethic
2.5
The study was conducted in accordance with the principles of the Declaration of Helsinki.
The authors confirm that the ethical policies of the journal, as outlined in the author guidelines, have been followed. The study was approved by the Ethics Committee of the Liguria Region (Protocol No. 575/2023). Informed consent for the use of clinical data for research purposes was obtained from all patients. The requirement for study‐specific informed consent was waived, as all procedures were part of the standard institutional screening protocol.
Results
3
Included Patients
3.1
During the study period 462 patients were transferred from the eICU to other wards. Of these, 440/462 (95.2%) patients were transferred as non‐colonised with C. auris , while 22/462 (4.8%) had tested positive during their eICU stay. Additional 13 * C. auris‐*colonised patients died during their eICU stay; for a total of 35 patients found colonised with C. auris while admitted to eICU during the study period. Overall, 275/440 (62.5%) patients were included in the study (see Figure 1 for reasons for exclusion). Among the 208 sufficiently screened patients (75.6% of included patients), 174/208 (83.7%) tested negative at all screenings performed, whereas 34/208 (16.3%) were found to be colonised with C. auris outside the eICU.
Flow chart of the study. Included: Patients who tested negative for C. auris colonisation both at eICU admission and discharge, and who had ≥ 1 screening swab performed post‐transfer. Sufficiently screened: Patients who underwent ≥ 2 swabs within the first 4 weeks after transfer.
The median duration of stay in the eICU was 5 days (IQR 2.3–11.8) for the overall population, with similar values observed across subgroups. The demographic and clinical characteristics of the study population are summarised in Table 1.
Figure 2 represents the rate of detection of colonisation outside the eICU, stratified according to the timing of last screening performed while admitted to eICU. Even in case of a negative swab performed within 24 h before transfer, post‐transfer colonisation was detected in 7.1% of tested patients (7/99).
Rate of detection of C. auris colonisation after transfer from eICU; overall (among included patients) and stratified according to the number of days elapsing between the last negative screening performed in the eICU and the day of transfer. Denominators refer to all patients tested at each timepoint. One patient was screened on day 16 and was not included in this figure. eICU, endemic intensive care unit.
Overall Detection of
C. auris Colonisation
3.2
During the study period, a total of 71 patients were identified as colonised with C. auris . Of these, 35 (49.3%) patients acquired colonisation in the eICU, while 34 (47.9%) were identified after transfer from the eICU, and additional 2 (2.8%) were identified as colonised after transfer from eICU, but did not perform any screening while in eICU (Figure 3).
Acquisition of Candida auris colonisation among the 71 positive patients during the study period. eICU, endemic ICU; non‐e‐ward, non‐endemic ward.
All patients were colonised at skin level, while 13/69 (18.8%) also showed colonisation at additional sites, including the urinary tract (8/69, 11.5%) and the respiratory tract (6/69, 8.7%). Table 2 summarises the main characteristics of patients colonised with C. auris during the study period.
Time to Detection of Colonisation
3.3
Of the 34 patients who became colonised after transfer from the eICU, 21 (61.8%) tested positive on their first swab (16 within 1 day, 4 between 3–7 days, and 1 after 10 days); 8 (23.5%) on their second swab (7 between 1–3 days, and 1 after 10 days); and 4 (12.9%) on their third swab (on Days 8, 20, 22, and 38). Among the 79 patients who had been screened by Day 8 with 3 swabs, one (1.3%) tested positive on Day 8. Overall, among 30 patients who had been screened with 5 swabs, one tested positive (3.3%) for the first time on the fifth swab performed 40 days after eICU transfer.
Among 17 patients who were excluded due to the absence of an eICU screening swab but were screened after transfer, two resulted positive: one on the first swab performed within 48 h after eICU transfer and the other on Day 7 after an initial negative swab collected on the day of transfer (detected colonisation rate: 2/17, 11.8%).
The detection rate of C. auris colonisation overtime after transfer from the eICU is reported in Figure 4.
Detection of C. auris colonisation rate after endemic intensive care unit (eICU) transfer to non‐endemic ward among included patients and stratified on the basis of days elapsed between transfer and the day of the positive result in a non‐endemic ward. Not all patients underwent screening at all pre‐defined time points.
C. auris
Candidemia
3.4
During the study period, among the 34 patients who became colonised after transfer from the eICU, 4 (11.8%) developed candidemia. The time from colonisation detection to candidemia onset was 2, 24, 49, and 50 days.
Conversely, among the 35 patients who were already colonised during their stay in the eICU, with a median follow‐up of 47 days (IQR 19.5–113.5), only one case of candidemia was observed (2.9%), which occurred 16 days after colonisation detection, when the patient was still admitted to eICU.
No cases of C. auris candidemia occurred in patients who were not colonised with C. auris , with a total number of hospital admissions during the study period of 47,861.
Overall, the proportion of C. auris candidemia among colonised patients during the study period was 7.3%, with lower rate in patients colonised during the eICU stay compared to those with colonisation detected after transfer (2.9% versus 11.8%, p = 0.15).
Interestingly, we observed a notable difference in the prevalence of candidemia between the clinical characteristics of patients with C. auris candidemia are summarised in Table 3.
Discussion
4
Our study is the first one to provide organised data on the screening for Candida auris colonisation in patients transferred from an endemic to a non‐endemic ward within the same hospital.
Current international recommendations suggest screening for C. auris colonisation in individuals at high risk, particularly patients recently admitted to healthcare facilities with known or suspected transmission of C. auris , or who have epidemiological links to other cases [9, 24, 25, 28]. Although defining who should be screened, guidelines provide limited and heterogenous guidance on key operational aspects, namely, the number of swabs to be performed, the type of microbiological test to perform (molecular vs. culture‐based), the need for repeated testing following a negative result, and the optimal frequency of screening. Recent studies have emphasised key aspects to consider in C. auris screening and infection control, including the importance of active surveillance, environmental hygiene, and targeted screening strategies in high‐risk or endemic settings [30, 31]. However, these studies mainly addressed institutional policies and general principles of outbreak containment, without providing standardised recommendations on the timing or repetition of screening.
Our study adds to this evidence by proposing a structured screening schedule and by addressing a specific epidemiological scenario, where within a single institution endemic ICU and non‐endemic wards coexist. Moreover, such intra‐hospital model effectively mirrors inter‐facility transfer dynamics, offering practical insight into colonisation detection and prevention strategies applicable at both hospital‐level and regional containment efforts.
Culture‐based screening remains the reference standard in many settings, but molecular assays offer a faster turnaround time and may enhance sensitivity, particularly in individuals with a low fungal burden or intermittent shedding of C. auris [32]. At our institution, PCR‐based screening was adopted as the standard method due to the aforementioned advantages, as well as to shorten the time length of contact precautions for patients testing negative.
This study provides evidence that screening only during admission and at discharge from endemic units, substantially underestimates the true burden of C. auris colonisation. Indeed, among patients who tested negative for C. auris colonisation at eICU discharge despite repeated weekly re‐testing, an additional 50% of all colonised cases were identified only after transfer. These findings suggest that screening limited to the endemic unit is insufficient and colonisation may become detectable only after eICU discharge, possibly due to acquisition during the final days or even hours of eICU stay or delayed detectability by diagnostic methods due to a progressive increase in skin burden of C. auris. Additionally, we observed that a single screening swab performed outside the eICU was able to detect only 60% of colonised individuals. Performing a second swab within 14 days allowed us to identify almost 90% of colonised patients. Therefore, our data support the implementation of at least twice molecular screening protocol for all patients transferred as non‐colonised from an endemic ward.
A notable aspect highlighted by our findings is the need for pre‐emptive contact isolation for patients transferred from endemic wards or facilities. Similarly, during a C. auris outbreak in the UK, individuals who had contact with a confirmed case were placed in pre‐emptive isolation and only released after three consecutive negative culture‐based screening swabs. Screening was then continued weekly until discharge [5]. However, no data was available on the performance, and thus clinical utility, of the second and third screening swab. Nevertheless, based on that study, national guidelines from the UK and Australia/New Zealand recommended three negative screenings, performed at least 24 h apart, before discontinuing contact isolation in at‐risk patients [24, 25]. Our data demonstrated that when endemic wards exist within the same institution, patients relocated from these areas to non‐endemic wards should be managed with infection prevention and control precautions similar to those applied during inter‐facility transfers, at least until two consecutive negative molecular swabs were obtained.
These findings carry important clinical and public health implications. Incomplete screening and premature discontinuation of isolation measures may lead to silent dissemination of C. auris across wards or institutions, undermining infection control efforts.
All cases of C. auris candidemia occurred in patients previously identified as colonised, consistent with existing literature indicating that colonisation is a prerequisite for invasive disease and further supporting the absence of cases of undetected colonisation [33]. The overall prevalence of C. auris candidemia among colonised patients in our hospital showed a decreasing trend compared to previous years (15%–26% during the period 2020 to 2023) [6, 20]. Interestingly, we observed higher rate of candidemia among patients with colonisation detected after transfer compared to those with colonisation diagnosed during eICU stay (11%–8% versus 2.9%). A possible explanation for such a difference might be a different survival rate among patients acquiring C. auris colonisation early during their ICU stay and possibly dying in ICU due to other complications, prior to candidemia development. However, this finding highlights the importance of post‐transfer screening also to provide prompt effective therapy in case of suspected infection in colonised patients, since no case of C. auris candidemia occurred in our hospital among non‐colonised patients.
Our study has several strengths. To our knowledge, it represents one of the most comprehensive and standardised evaluations of C. auris colonisation management in patients transferred from an endemic to a non‐endemic ward in the same institution. The implementation of serial screening enabled us to identify operational gaps not fully addressed by current protocols and to propose targeted interventions. This hospital organization mirrors the dynamics of patient transfers between endemic and non‐endemic institutions, making our findings relevant to similar real‐world settings.
Additionally, patient identification and data extraction were performed using software‐based selection followed by manual validation to maximise enrolment, although this approach may have missed a small number of eligible cases. The use of molecular screening likely contributed to the timely and sensitive detection of colonisation.
However, we also observed that compliance with the screening protocol was suboptimal, particularly in high‐burden settings, which may have led to underestimation of true colonisation rates. Another limitation of our study is the fact that the generalizability of our findings depends on local epidemiology, type of endemic ward and type of screening method used and may not be directly applicable to other settings without appropriate contextualization. Moreover, cutaneous screening was limited to the axilla and groin, in accordance with current recommendations, while additional anatomical sites (e.g., nasal swabs) were not actively screened. Recent evidence suggest that including these sites could improve detection sensitivity [34, 35].
To conclude, our data suggest that a more tailored approach to screening and isolation, based on local epidemiology and repeated testing, may help to optimise resource utilisation without compromising patient safety. The epidemiological duality at our institution underscores the need for internal risk stratification and unit‐specific protocols and could be a model for other large healthcare facilities facing similar challenges.
Our findings support the need for repeated screening after transfer from endemic to non‐endemic units, ideally within the first 2 weeks post‐transfer, and for maintaining pre‐emptive isolation even in patients transferred as non‐colonised, in order to effectively identify delayed colonisation and prevent further transimission.
Author Contributions
Laura Mezzogori: conceptualization, investigation, validation, visualization, writing – original draft, writing – review and editing. Martina Bavastro: investigation, data curation, writing – review and editing. Laura Magnasco: conceptualization, investigation, formal analysis, visualization, validation, writing – review and editing. Federica Centorrino: investigation, data curation, writing – review and editing. Riccardo Schiavoni: investigation, data curation, writing – review and editing. Federica Portunato: data curation, investigation, writing – review and editing. Daniele Roberto Giacobbe: data curation, investigation, writing – review and editing. Antonio Vena: data curation, investigation, writing – review and editing. Vincenzo Di Pilato: data curation, investigation, writing – review and editing. Ramona Barbieri: investigation, data curation, writing – review and editing. Andrea Orsi: investigation, writing – review and editing, software. Giancarlo Icardi: software, investigation, writing – review and editing. Anna Marchese: investigation, resources, writing – review and editing. Matteo Bassetti: data curation, investigation, writing – review and editing. Malgorzata Mikulska: conceptualization, investigation, methodology, formal analysis, software, resources, visualization, supervision, writing – review and editing, writing – original draft.
Funding
This is a non‐profit project supported by an unconditional grant awarded within the framework of the Gilead Fellowship Program 2023 [grant number N375A]. The company had no role in the design of the study, data collection or analysis, interpretation of results, or in the writing or approval of the manuscript.
Conflicts of Interest
Outside the submitted work, Matteo Bassetti has received funding for scientific advisory boards, travel, and speaker honoraria from Cidara, Gilead, Menarini, MSD, Mundipharma, Pfizer, and Shionogi. Outside the submitted work, Daniele Roberto Giacobbe reports investigator‐initiated grants from Pfizer, Shionogi, BioMérieux, Menarini, Tillotts Pharma, and Gilead Italia, travel support from Pfizer, and speaker/advisor fees from Pfizer, Menarini, BioMérieux, Advanz Pharma, and Tillotts Pharma. Outside the submitted work, Antonio Vena reports personal fees for speaker/advisor from Pfizer Inc., Shionogi, Tillotts Pharma, Menarini, Gilead Italia, Mundipharma, Advanz pharma and MSD. Outside the submitted work, Vincenzo Di Pilato reports travel support and speaker honoraria from Arrow Diagnostics. Outside the submitted work, Anna Marchese has received research grants for the laboratory from DiaSorin. Outside the submitted work, Laura Mezzogori received an honorarium from HealthData Consulting S.r.l. for acting as a Discussant at an educational event The remaining authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization (WHO) , WHO Fungal Priority Pathogens List to Guide Research, Development and Public Health Action (World Health Organization (WHO), 2022), https://www.who.int/publications/i/item/9789240060241.
- 2CDC , Antibiotic Resistance Threats in the United States, 2019 (U.S. Department of Health and Human Services, CDC, 2019), https://www.cdc.gov/antimicrobial‐resistance/data‐research/threats/index.html.
- 3B. R. Jackson , N. Chow , K. Forsberg , et al., “On the Origins of a Species: What Might Explain the Rise of Candida auris?,” Journal of Fungi 5, no. 3 (2019): 58, 10.3390/jof 5030058.31284576 PMC 6787658 · doi ↗ · pubmed ↗
- 4S. Ahmad and M. Asadzadeh , “Strategies to Prevent Transmission of Candida auris in Healthcare Settings,” Current Fungal Infection Reports 17, no. 1 (2023): 36–48, 10.1007/s 12281-023-00451-7.36718372 PMC 9878498 · doi ↗ · pubmed ↗
- 5S. Schelenz , F. Hagen , J. L. Rhodes , et al., “First Hospital Outbreak of the Globally Emerging Candida auris in a European Hospital,” Antimicrobial Resistance and Infection Control 5 (2016): 35, 10.1186/s 13756-016-0132-5.27777756 PMC 5069812 · doi ↗ · pubmed ↗
- 6F. Briano , L. Magnasco , C. Sepulcri , et al., “ Candida auris Candidemia in Critically Ill, Colonized Patients: Cumulative Incidence and Risk Factors,” Infectious Disease and Therapy 11, no. 3 (2022): 1149–1160, 10.1007/s 40121-022-00625-9.PMC 899591835404010 · doi ↗ · pubmed ↗
- 7K. Southwick , B. Ostrowsky , J. Greenko , et al., “A Description of the First Candida auris‐Colonized Individuals in New York State, 2016–2017,” American Journal of Infection Control 50, no. 3 (2022): 358–360, 10.1016/j.ajic.2021.10.037.34793894 PMC 9853438 · doi ↗ · pubmed ↗
- 8K. Satoh , K. Makimura , Y. Hasumi , Y. Nishiyama , K. Uchida , and H. Yamaguchi , “ Candida auris sp. Nov., a Novel Ascomycetous Yeast Isolated From the External Ear Canal of an Inpatient in a Japanese Hospital,” Microbiology and Immunology 53, no. 1 (2009): 41–44, 10.1111/j.1348-0421.2008.00083.x.19161556 · doi ↗ · pubmed ↗