Candida guilliermondii endocarditis in a patient with prosthetic mitral valve: a case report
Saravana Priya J K, Gomathi Manju Balasubramaniam, Ramani C P

TL;DR
A rare case of Candida guilliermondii endocarditis in a patient with a prosthetic mitral valve is reported, emphasizing the need for early diagnosis and targeted treatment.
Contribution
This case report adds to the limited clinical literature on C. guilliermondii endocarditis in prosthetic valve patients.
Findings
Candida guilliermondii was identified as the causative agent through blood cultures.
Echocardiography revealed prosthetic valve vegetation and aortic regurgitation.
The case underscores the importance of prompt antifungal therapy and multidisciplinary care.
Abstract
Candida endocarditis, though rare, presents significant risks, especially in prosthetic valve recipients. Candida guilliermondii is an uncommon causative pathogen, necessitating a high index of suspicion, advanced diagnostics, and prompt antifungal therapy to improve patient outcomes. A 57-year-old male with a history of rheumatic heart disease and prior mitral valve replacement presented with fever, chills, and generalized body aches for 10 days. Laboratory investigations revealed microcytic hypochromic anemia, while echocardiography demonstrated prosthetic valve vegetation with mild to moderate aortic regurgitation. Blood cultures confirmed C. guilliermondii infection. Early recognition, multidisciplinary collaboration, and tailored antifungal therapy are pivotal for favorable outcomes in C. guilliermondii prosthetic valve endocarditis. This case highlights the importance of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
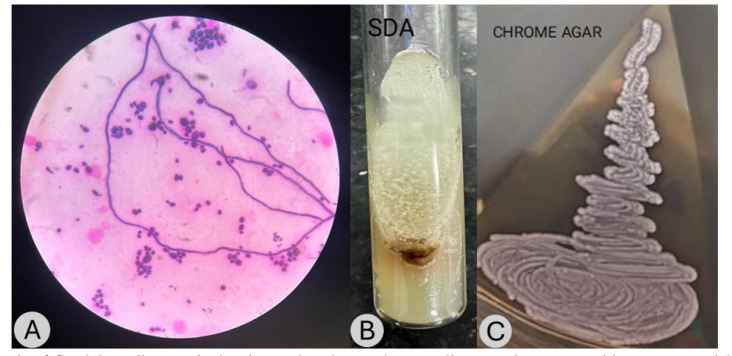 Figure 1
Figure 1| Date (approximate) | Event |
|---|---|
| 15 years ago | Diagnosis of rheumatic heart disease with mitral stenosis |
| 1 year ago | Performance of mitral valve replacement surgery |
| 10 days ago | Onset of fever and intermittent chills, Development of intermittent body aches |
| Day 1 | Blood cultures drawn, revealing |
| Day 3 | VITEK identification confirmed |
| Day 4 to Day 46 | Start of caspofungin and fluconazole therapy. Continued for 6 weeks |
| Follow-up (6 weeks post-treatment) | Repeat echocardiography showing no residual vegetations, confirming infection resolution; continuation of fluconazole suppression therapy |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Fungal Infections and Studies · Infective Endocarditis Diagnosis and Management
Introduction
Infective endocarditis (IE) remains a formidable clinical challenge, characterized by the microbial colonization of the endocardial surface of the heart, frequently resulting in grave morbidity and mortality. While bacterial etiologies predominate, fungal endocarditis–though relatively infrequent–presents significant therapeutic complexities owing to its notoriously high mortality rates and the intricacies of antifungal treatment regimens. Among fungal pathogens, Candida species hold particular clinical relevance, with C. guilliermondii emerging as a rare but increasingly reported causative agent of IE [ 1 ].
Candida guilliermondii, a non-albicans Candida species, is predominantly recognized in immunocompromised individuals and those with prosthetic heart valves or intravascular medical devices. Fungal endocarditis, albeit constituting only 1–6% of all IE cases, has dire prognostic implications, with Candida species accounting for approximately 2% of these infections. The associated mortality rates remain alarmingly high, ranging from 30% to 80% [ 2 ].
The diagnostic conundrum of fungal IE stems from its nonspecific clinical manifestations, necessitating advanced imaging modalities, such as echocardiography, and rigorous microbiological assessments to ensure precise identification. Current therapeutic paradigms underscore the indispensability of surgical intervention in tandem with prolonged antifungal administration. Echinocandins and amphotericin B have demonstrated superior efficacy in the management of fungal IE, yielding improved clinical outcomes [ 3 ].
This particular case is noteworthy due to the convergence of predisposing cardiac pathology -rheumatic heart disease with mitral stenosis- a prior mitral valve replacement, and the subsequent development of C. guilliermondii endocarditis, thereby posing substantial diagnostic and therapeutic hurdles [ 4 ].
Case Presentation
A 57-year-old male, diagnosed 15 years prior with rheumatic heart disease and mitral stenosis, underwent mitral valve replacement a year ago. The patient presented with a 10-day history of persistent fever, intermittent chills, and generalized body aches. Informed verbal consent was obtained from him before disclosing patient details.
Upon examination, the patient exhibited signs of systemic illness. Cardiovascular auscultation revealed an ejection click, indicative of valvular pathology. Hematological analysis demonstrated microcytic hypochromic anemia, reinforcing underlying systemic inflammation.
A normally functioning prosthetic valve in the mitral position was observed. Myocardial velocity gradients measured 19 mm Hg (peak) and 15 mm Hg (mean). A highly mobile vegetation with a size of 7 mm was detected. Mild to moderate aortic regurgitation was present, with no tricuspid regurgitation or evidence of abnormal pressure half-time. Left ventricular systolic function was preserved.
Further infectious disease workup ruled out bacterial etiologies, with negative Widal and dengue tests. The blood specimen was processed using the BACTEC and VITEK 2 Compact automated system, a widely recognized tool for microbial identification. Following incubation and analysis, the system confirmed the presence of C. guilliermondii, enabling precise species-level identification and guiding targeted antifungal therapy. Gram staining of C. guilliermondii revealed oval to elongated yeast-like cells (Figure 1A). Pseudohyphae were observed, though they exhibited limited and sparse branching. On Sabouraud dextrose agar, the isolate formed flat, moist, and smooth colonies with a cream to pale yellow pigmentation (Figure 1B). When cultured on CHROMagar Candida, C. guilliermondii developed distinctive pink to beige colonies (Figure 1C). Antifungal susceptibility testing performed by the system provided crucial insights into the sensitivity profile of the pathogen. The minimum inhibitory concentrations for voriconazole, caspofungin, fluconazole, micafungin, amphotericin B, and flucytosine were < 0.12 µg/mL, 0.5 µg/mL, 1 µg/mL, 0.5 µg/mL, 0.5 µg/mL, and < 1 µg/mL, respectively. All tested antifungal agents showed sensitivity, guiding the selection of an appropriate therapeutic regimen. Based on these results, a tailored antifungal treatment strategy was initiated, ensuring optimal management of C. guilliermondii endocarditis and improving patient prognosis.
(A) Gram stain of Candida guilliermondii showing oval to elongated yeast cells, appearing gram-positive to gram-variable. Pseudohyphae were present but typically sparsely branched. (B) Sabouraud dextrose agar culture of Candida guilliermondii showing flat, moist, smooth colonies with a cream to yellow coloration. (C) CHROMagar Candida culture of Candida guilliermondii showing pink to beige colonies, distinguishing it from other Candida species
The patient underwent a two-week regimen of combination antifungal therapy, incorporating caspofungin and fluconazole, to target the infection effectively. Caspofungin was administered at 70 mg on the first day, followed by 50 mg daily, while fluconazole was administered at 400 mg (6 mg/kg) daily. A repeat blood culture subsequently returned negative, confirming microbial clearance. Given the high recurrence risk associated with prosthetic valve infections, fluconazole (400 mg/day) was extended for an additional six weeks as a suppressive regimen to prevent relapse and ensure sustained eradication of the pathogen. Surgical intervention was not performed in this case. While fungal endocarditis, especially on prosthetic valves, often requires surgery, the non-surgical approach was selected due to clinical stability, response to antifungal therapy, and comorbidities. The patient showed a favorable response to caspofungin and fluconazole therapy without signs of worsening infection.
Follow-up echocardiography, which was performed for six weeks post-treatment, showed no residual vegetations, confirming infection resolution. The patient remained clinically stable, with no signs of recurrent fungemia or valvular dysfunction. Long-term monitoring continued with fluconazole suppression therapy to prevent relapse. Timeline of symptoms is demonstrated in Table 1.
Discussion
Fungal IE, particularly Candida species-associated infections, remains a formidable clinical challenge due to its high morbidity and mortality rates. While Candida albicans is the most frequently implicated species, C. guilliermondii has been increasingly documented in prosthetic valve recipients and immunocompromised individuals. Rarity of C. guilliermondii in endocarditis necessitates heightened diagnostic awareness and a tailored therapeutic approach.
Clinical literature underscores the necessity of a multimodal treatment strategy, integrating surgical valve replacement with prolonged antifungal therapy. Echinocandins, such as caspofungin, and polyenes, notably amphotericin B, have demonstrated superior efficacy in eradicating fungal endocarditis. However, fluconazole remains a viable option for susceptible strains, particularly in cases where long-term suppressive therapy is required [ 5 ].
Clinical presentations of the patient, diagnostic findings, and microbiological confirmation of C. guilliermondii emphasized the urgency of an expedited and methodical treatment approach. Successful resolution of infections following targeted antifungal therapy highlights the critical need for early fungal pathogen consideration in prosthetic valve recipients presenting with infective endocarditis [ 6 ].
Given the diagnostic challenges, standard blood cultures may be insufficient, necessitating advanced methods, such as VITEK, Matrix-Assisted Laser Desorption/Ionization Time-of-Flight, and polymerase chain reaction for precise identification. Prior antimicrobial exposure further complicates fungal detection, while biomarkers, such as β-D-glucan, enhance diagnostic accuracy [ 7 ].
A combination of caspofungin and fluconazole is effective in infective endocarditis caused by Candida species, as it targets both cell wall and membrane integrity. Studies suggest that combination therapy improves fungal clearance and reduces resistance risk [ 8 , 9 ].
Recent case reports reinforce the importance of early recognition and aggressive management. A documented case of C. guilliermondii native left-sided valve endocarditis demonstrated the efficacy of surgical intervention combined with fluconazole therapy, leading to sustained patient recovery. Similarly, reports of prosthetic valve C. parapsilosis endocarditis highlight the necessity of both antifungal treatment and timely surgical intervention.
One of the strengths of this study was a meticulous diagnostic approach integrating echocardiography and blood cultures that facilitated timely identification of the causative pathogen. Prompt initiation of targeted antifungal therapy proved instrumental in mitigating disease progression. A collaborative effort among cardiologists, infectious disease specialists, and laboratory experts ensured holistic patient management.
Among the limitations of this study was the initially nonspecific symptomatology that rendered early clinical suspicion challenging. Moreover, the rarity of C. guilliermondii infections may have contributed to diagnostic delays. Limited access to advanced molecular diagnostics may constrain timely pathogen identification in certain clinical settings.
Conclusion
This case underscored the complexity of fungal infective endocarditis, particularly with rare pathogens, like C. guilliermondii, in prosthetic valve recipients. Early detection, advanced diagnostics, and a targeted antifungal regimen were crucial in achieving a favorable outcome. Given the high mortality rates, a vigilant, multidisciplinary approach is essential for optimizing patient recovery and ensuring effective management of such infections.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wilcock JN Gallagher AJ Wengenack NL Noyes CD Klick JC Wojewoda CM Candida guilliermondii / Kodamaea ohmeri endocarditis Mycopathologia 2023188690783753729510.1007/s 11046-023-00767-5 · doi ↗ · pubmed ↗
- 2Arnold CJ Johnson M Bayer AS Bradley S Giannitsioti E MiróJ Metal Candida infective endocarditis: an observational cohort study with a focus on therapy Antimicrob Agents Chemother 20155942365732564585510.1128/AAC.04867-14PMC 4356766 · doi ↗ · pubmed ↗
- 3Falcone M Barzaghi N Carosi G Grossi P Minoli L Ravasio Vetal Candida infective endocarditis: report of 15 cases from a prospective multicenter study Medicine 200988316081944011910.1097/MD.0b 013e 3181 a 693f 8 · doi ↗ · pubmed ↗
- 4Sankar NP Thakarar K Rokas KE Candida infective endocarditis during the infectious diseases and substance use disorder syndemic: a six-year case series Open Forum Infect Dis 202075 ofaa 1423249457910.1093/ofid/ofaa 142PMC 7252282 · doi ↗ · pubmed ↗
- 5Zheng Z Tu X Jiang C Liu F Fan C First case report of Candida guilliermondii native left-sided valve endocarditis Front Cardiovasc Med 2023 1012732553811188810.3389/fcvm.2023.1273255 PMC 10725942 · doi ↗ · pubmed ↗
- 6Mandal A Prosthetic valve endocarditis due to Candida parapsilosis: a rare disease with high mortality- A case report J Clin Case Rep Clin Study 202395
- 7El Nouwar R Larranaga Lapique E Vanden Eynden F Martiny D Remmelink M Roussoulières Aetal Heart transplantation for refractory Candida tropicalis endocarditis: a case report and literature review Microorganisms 20251335804014247210.3390/microorganisms 13030580 PMC 11945179 · doi ↗ · pubmed ↗
- 8Thompson GR III Jenks JD Baddley JW Lewis JS 2nd Egger M Schwartz I Setal Fungal endocarditis: pathophysiology, epidemiology, clinical presentation, diagnosis, and management Clin Microbiol Rev 2023363 e 00019233743968510.1128/cmr.00019-23PMC 10512793 · doi ↗ · pubmed ↗