Scedosporium apiospermum-induced brain abscess leading to rapid mortality in an immunocompetent adult male from Uttarakhand, India
Minakshi Singh, Priyal Anand, Sowjanya Perumalla, Amber Prasad

TL;DR
A healthy adult in India died from a rare brain infection caused by a soil fungus after a sewer fall, highlighting the need for quick diagnosis and treatment.
Contribution
This case report highlights the rare and fatal progression of Scedosporium apiospermum brain abscess in an immunocompetent individual.
Findings
Scedosporium apiospermum can cause fatal brain abscesses in immunocompetent individuals following environmental exposure.
Aggressive treatment, including surgery and antifungal therapy, failed to prevent mortality in this case.
Early diagnosis and multidisciplinary management are crucial for improving outcomes in such rare infections.
Abstract
Scedosporium apiospermum, a soil-dwelling fungus, is typically associated with localized infections, such as skin infections and osteomyelitis. However, it can also cause invasive central nervous system infections, including brain abscesses, particularly in immunocompromised individuals. Such infections are rare in immunocompetent individuals and often occur following trauma or environmental exposure. This report aimed to present a case of a fatal S. apiospermum brain abscess in an immunocompetent adult male, highlighting diagnostic and management challenges. A 48-year-old immunocompetent male presented with a three-day history of persistent holo-cranial headache and left-sided weakness. Twenty days earlier, the patient had fallen into a sewer, likely exposing him to fungal pathogens. Initial imaging revealed a large right frontal intracranial lesion. Surgical resection of the abscess…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
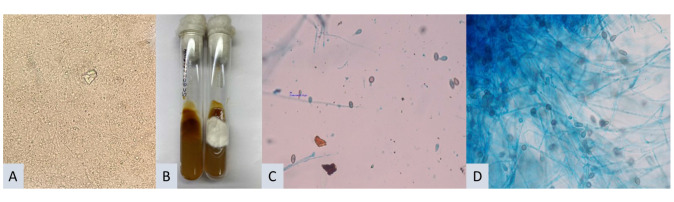 Figure 1
Figure 1| Test | Day 1 Results | Day 2 Results | Comments |
|---|---|---|---|
| Contrast-enhanced MRI of the brain | T2 hyperintense mass (6.3×4.1×4.1 cm) with peripheral enhancement | Not done | Suggestive of cerebral abscess |
| Hemoglobin | 13.7 g/dL | 11.3 g/dL | Decreased over 24 h |
| Total leukocyte count | 19.1×103 cells/µL | 18.8×103 cells/µL | Slight decrease |
| Platelet count | 173×103/µL | 125×103/µL | Decreased over 24 h |
| Blood urea | 74 mg/dL | 57 mg/dL | Improvement noted |
| Serum creatinine | 1.28 mg/dL | 0.9 mg/dL | Improvement noted |
| Serum sodium | 141 mmol/L | 154 mmol/L | Increased |
| Serum potassium | Within normal limits | Within normal limits | Within normal limits |
| Liver function tests (SGPT/SGOT) | SGPT: 58 U/L, SGOT: 31 U/L | Not done | Within normal limits |
| Gram stain (pus from the brain) | No microorganisms observed, abundant pus cells seen | Not done | No bacterial microorganism observed |
| KOH examination (pus from the brain) | N/A | Hyaline septate hyphae | Indicated fungal presence |
| Fungal culture (pus from the brain) | N/A | Confirmed fungal pathogen | |
| ZN Stain and CBNAAT for | Negative | Negative | No evidence of tuberculosis infection |
| Viral Markers (HCV, HBV, HIV) | Negative | N/A | Confirmed absence of Hepatitis B, Hepatitis C, and HIV infections |
| Year | Country | Age/Gender | Possible predisposing condition | Clinical picture | Treatment given | Outcome | References |
|---|---|---|---|---|---|---|---|
| 2008 | Turkey | Not specified | Trauma | Rapid progression of neurological symptoms, brain abscess confirmed via imaging and microbiology | Surgical drainage, voriconazole therapy | Worsened | [ |
| 2008 | Multiple countries | 107 patients (varied) | Immunocompromised and some immunocompetent individuals | Fever, headache, focal neurological signs, worsening despite antifungal therapy, often with poor outcomes | Voriconazole therapy (some cases also had surgical intervention) | Often fatal | [ |
| 2013 | Australia (Sydney) | 69 years/male | Exposure to contaminated soil, silicosis | Headache, fever, focal neurological deficits, imaging revealing a large frontal brain abscess | Surgical intervention, voriconazole therapy | Death | [ |
| 2012 | Multiple countries | Multiple patients | Environmental exposures, such as trauma, soil exposure, and near-drowning | CNS symptoms, including headache, fever, focal neurological deficits, and positive imaging findings | Surgical drainage, voriconazole therapy | Variable | [ |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Bacterial Infections and Vaccines · Fungal Infections and Studies
Introduction
At least 5 species of Scedosporium (S. apiospermum, S. boydii, S. aurantiacum, S. dehoogii, and S. minutisporum) can cause human infections [ 1 ]. Scedosporium is a genus of fungi that includes S. apiospermum and S. prolificans. These fungi are commonly found in soil, polluted water, and sewage, and infections caused by them are collectively referred to as Scedosporiosis [ 2 ]. Although S. apiospermum, formerly known as Monosporium apiospermum, is typically associated with various clinical manifestations such as skin infections and osteomyelitis, it has a predilection for causing central nervous system (CNS) infections, particularly brain abscesses [ 3 , 4 ].
Brain abscesses are generally more frequent in immunocompromised individuals; however, they can also occur in otherwise healthy individuals, particularly those with a history of environmental exposure, such as trauma or immersion in contaminated water [ 5 ]. CNS infections caused by S. apiospermum are known for their severe progression and high mortality rate, which has been reported to be as high as 74% [ 6 ]. A systematic review by Firoozeh Kerman et al. evaluated thirty-eight studies involving 41 patients from January 1, 2007, to April 20, 2022, and found an overall mortality rate of 51.2% due to Scedosporium infections [ 7 ]. Previous studies have shown that the mortality rate can reach up to 65%-100%, once Scedosporium disseminates systematically or invades the brain [ 8 ].
The diagnosis of Scedosporiosis presents significant challenges due to its clinical and microbiological similarities with other fungal infections. Accurate identification relies heavily on microbiological culture and histopathological examination, making early and precise diagnosis crucial for effective treatment. Treatment typically involves a combination of surgical intervention and antifungal therapy, with voriconazole being the preferred drug [ 8 , 9 ]. This report describes a case of a rapidly fatal brain abscess caused by S. apiospermum in an immunocompetent adult male, emphasizing the urgent need for prompt diagnosis and intervention.
Case Presentation
A 45-year-old male presented with a 3-day history of moderate holocranial headache, which showed mild relief with medication, accompanied by left-sided weakness. He had no episodes of vomiting, seizures, or loss of consciousness. There was no history of diabetes, hypertension, smoking habit, or any other metabolic disease. The patient had fallen into a sewer 20 days prior and was initially managed at another facility before being transferred to the All India Institute of Medical Sciences, Rishikesh, India, for further treatment. Although he could respond to commands by opening his eyes, he was unable to speak. Physical examinations of the pulmonary, cardiovascular, and abdominal systems were unremarkable.
Initial investigations on day 1 of hospitalization included complete blood count, blood urea, serum sodium, serum potassium, creatinine, liver function tests, and a contrast-enhanced magnetic resonance imaging (MRI) of the brain. The MRI revealed a T2 hyperintense right frontal mass measuring 6.3 × 4.1 × 4.1 cm with post-contrast peripheral enhancement, suggesting a cerebral abscess. Surgical intervention was planned for the following day, and viral markers were tested, and all results were negative.
During the surgery, a right fronto-temporo-parietal craniotomy was performed. The tense dura was opened, revealing a significant brain bulge. Cortisectomy of the right middle frontal gyrus exposed an abscess cavity with a thick, non-vascular capsule containing pale yellow pus. Gross total resection was achieved, and the abscess capsule was removed. The bone flap was stored in the abdomen, and pus was sent for microbiological analysis, including Gram stain, KOH testing, aerobic bacterial culture, fungal culture, Ziehl-Neelsen (ZN) staining, cartridge-based nucleic acid amplification test (CBNAAT) for Mycobacterium tuberculosis, and histopathology (Table 1).
Postoperatively, the patient was admitted to the intensive care unit, where his Glasgow Coma Scale declined to E2V1M5, necessitating intubation and ventilatory support. Despite treatment with antibiotics, antifungals, antiepileptics, analgesics, and decongestants, he developed high-grade fever and hypotension, requiring inotropic support. Based on the KOH findings, voriconazole was initiated, but his condition continued to deteriorate, resulting in a cardiac arrest on the third day. Despite resuscitation efforts, he was declared dead. Fungal culture of the pus obtained during surgery confirmed the presence of Scedosporium apiospermum after 14 days of incubation. Cause of death was determined to be septic shock resulting from a right frontal fungal abscess due to Scedosporium species, with associated mass effect and midline shift.
Laboratory investigations
Table 1 summarizes the key laboratory findings and their significance for the case. Contrast-enhanced MRI of the brain revealed a T2 hyperintense mass measuring 6.3 × 4.1 × 4.1 cm with peripheral enhancement, suggestive of a cerebral abscess.
Pus sample from the brain was sent for microbiological analysis. Gram stain of the pus revealed an abundance of pus cells, but no microorganisms. However, the KOH (10%) examination of the pus showed the presence of hyaline, septate hyphae [Figure 1 (A)].
(A) KoH mount of pus sample from brain showing hyaline septate hyphae (40×). (B) Growth on Sabouraud dextrose agar- Grayish black reverse and white cottony growth on the obverse side. (C and D) Lactophenol cotton blue images of the growth showing branching septate hyphae with single-celled ovoid conidia, typical of Scedosporium apiospermum
No signs of tuberculosis were detected in the pus sample, as acid-fast bacilli were absent in the ZN stain. Additionally, the CBNAAT using the GeneXpert system (Cepheid Inc.) was also negative for M. tuberculosis.
The pus sample obtained from the brain abscess was inoculated onto Sabouraud dextrose agar (SDA) and incubated aerobically at 37 °C. After 14 days of aerobic incubation, the culture displayed white, cottony growth on the front, while the reverse side showed a grayish-black coloration [Figure 1 (B)]. A lactophenol cotton blue mount was prepared from the fungal growth, which revealed branching septate hyphae with single-celled, ovoid conidia, characteristic of S. apiospermum [Figure 1 (C and D)].
Mould identification was carried out using the VITEK^®^ MS Mould Kit (BioMérieux, France), which provides reagents for protein extraction and inactivation from agar plates for subsequent analysis by the VITEK^®^ MS System (BioMérieux, France). The process involved collecting a 1-2 cm diameter sample of mould from Sabouraud Dextrose Agar (SDA) plates using a sterile swab. The sample was then suspended in 0.9 mL of ethanol (70%), followed by centrifugation. After discarding the supernatant, the pellet was treated with formic acid (70%) and acetonitrile (100%) for protein extraction and inactivation. The resulting protein mixture was spotted on a target slide, dried, and overlaid with the VITEK® MS-CHCA matrix for analysis [ 10 ]. The processed slide was analyzed using the VITEK® MS System (BioMérieux, France) for mould identification based on the mass spectrometric profile, and was identified as S. apiospermum [ 13 ].
Discussion
This case report presents a rapidly fatal brain abscess caused by S. apiospermum in an immunocompetent adult male. Although infections due to S. apiospermum are commonly seen in immunocompromised individuals, this case underscores that environmental exposure, such as trauma or contamination with soil or water, can serve as a significant risk factor even in healthy individuals. The patient's fall into a sewer 20 days prior to the onset of symptoms likely played a crucial role in facilitating the fungal invasion, highlighting the importance of environmental factors in the pathogenesis of Scedosporium infections.
The patient's diagnosis was delayed due to the nonspecific presentation and initial lack of suspicion for a fungal etiology. This is consistent with many previous cases, where initial symptoms often mimic more common bacterial infections, leading to delayed appropriate antifungal treatment [ 2 ]. Unlike some reports where patients had identifiable risk factors such as immunosuppression or history of near-drowning, this patient had no such predispositions apart from a fall into a sewer, which likely introduced the pathogen [ 3 ].
Compared with other reported cases, the age and immunological status of patients have varied widely. The majority of patients with Scedosporium infections reported in the literature were immunocompromised [ 2 , 6 ], including those with leukemia, transplant recipients, and individuals on long-term corticosteroid therapy. These patients usually exhibited severe disseminated infections, including brain abscesses, and had a poorer prognosis than immunocompetent individuals.
Previous case reports have documented varying outcomes in Scedosporium brain abscesses. Wilson and Kennedy (2013) reported a fatal case of an immunocompetent 69-year-old male with silicosis who developed a brain abscess following environmental exposure [ 3 ]. Similarly, other case reports have documented fatal cases involving immunocompetent individuals with environmental exposure, emphasizing that trauma-related contamination remains a critical risk factor even in the absence of immunosuppression. These cases demonstrate that despite aggressive surgical and medical intervention, Scedosporium CNS infections carry a high mortality risk.
Globally, S. apiospermum infections affect various age groups and immunological statuses. In a study by Troke et al. (2008) involving 107 patients treated with voriconazole, most were immunocompromised, spanning from children to the elderly, with a high mortality rate, especially among those with CNS involvement [ 8 ]. This study reinforces our case findings, where the patient succumbed to the infection despite prompt surgical and medical intervention due to its aggressive nature and septic shock complications. Review of literature of similar cases of brain abscess by the Scedosporium spp. from India and abroad have been depicted in Table 2.
Treatment for S. apiospermum infections usually combines surgical intervention and antifungal therapy. In this case, gross total resection (GTR) of the abscess was achieved, which literature supports as crucial for reducing fungal load and improving outcomes [ 10 ]. Voriconazole is the cornerstone of treatment for S. apiospermum infections [ 8 ]. Unlike S. apiospermum, which demonstrates good susceptibility to voriconazole, S. prolificans exhibits notable resistance to most antifungal agents, including voriconazole, making infections with this species particularly challenging to treat [ 11 ]. In contrast, Nesky et al. reported successful treatment of a Pseudallescheria boydii brain abscess with surgical drainage and voriconazole [ 12 ]. Despite starting voriconazole based on KOH findings, the patient's condition worsened. This aligns with literature indicating that while voriconazole is effective, CNS infections have a poor prognosis and high mortality rates even with treatment [ 6 ].
S. apiospermum infections, while reported worldwide, rarely lead to brain abscesses. Most cases occur in immunocompromised individuals, yet there are significant instances in immunocompetent patients, particularly after trauma or near-drowning events. The patient's fall into a sewer in this case underscores the potential risk from environmental fungi, suggesting that a more thorough initial evaluation might have been beneficial. Clinicians must maintain a high suspicion for fungal pathogens in similar scenarios. Unfortunately, despite aggressive surgical and medical management, the outcome was fatal, highlighting the urgent need for further research into effective treatment protocols and antifungal therapies. This case reinforces the aggressive nature of S. apiospermum infections and the challenges in diagnosing and managing fungal brain abscesses. Previous cases have consistently demonstrated the difficulties in early detection and the limited success of current strategies, emphasizing the need for heightened clinical awareness and advancements in diagnostic techniques to improve patient outcomes.
Conclusion
This case of S. apiospermum brain abscess in an immunocompetent individual highlights the potential for rapid disease progression and the challenges in the diagnosis of fungal CNS infections. Despite the absence of typical risk factors, environmental exposure, such as trauma and contamination from a sewer, likely played a key role in the onset of the infection. Rapid deterioration of the patient, even with aggressive treatment, underscores the high mortality rate associated with these infections.
Early recognition and intervention are critical, as fungal brain abscesses can often mimic more common conditions, leading to diagnostic delays. This case emphasized the need for heightened clinical suspicion in patients with neurological symptoms and a history of environmental exposure, regardless of their immune status. Given the limited success of current antifungal treatments in such severe cases, further research into adjunctive therapies and alternative antifungals is essential. Clinicians should remain vigilant and consider fungal etiologies when managing brain abscesses, especially in cases where environmental factors may be involved. Improved diagnostic methods and treatment strategies are crucial for better patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yan P Chen J Wang H Jia Q Xie J Mo G A systemic infection involving the lung, brain, and spine caused by Scedosporium apiospermum species complex after near-drowning: a case report and literature review BMC Infect Dis 20242413423851507510.1186/s 12879-023-08279-9PMC 10956195 · doi ↗ · pubmed ↗
- 2Cortez KJ Roilides E Quiroz-Telles F Meletiadis J Antachopoulos C Knudsen T Walsh TJ Infections caused by Scedosporium spp Clin Microbiol Rev 20082111571971820244110.1128/CMR.00039-07PMC 2223844 · doi ↗ · pubmed ↗
- 3Wilson HL Kennedy KJ Scedosporium apiospermum brain abscesses in an immunocompetent man with silicosis Med Mycol Case Rep 2013275782443222210.1016/j.mmcr.2013.02.006PMC 3885959 · doi ↗ · pubmed ↗
- 4Tadros TS Workowski KA Siegel RJ Hunter S Schwartz DA Pathology of hyalohyphomycosis caused by Scedosporium apiospermum (Pseudallescheria boydii): an emerging mycosis Hum Pathol 19982912661272982410510.1016/s 0046-8177(98)90255-6 · doi ↗ · pubmed ↗
- 5Bouza E Munoz P Invasive infections caused by Blastoschizomyces capitatus and Scedosporium spp Clin Microbiol Infect 20041076851474880410.1111/j.1470-9465.2004.00842.x · doi ↗ · pubmed ↗
- 6Kantarcioglu AS Guarro Jde Hoog GS Central nervous system infections by members of the Pseudallescheria boydii species complex in healthy and immunocompromised hosts: epidemiology, clinical characteristics and outcome Mycoses 200851275901833144810.1111/j.1439-0507.2008.01489.x · doi ↗ · pubmed ↗
- 7Kermani F Yazdani Charati J Roohi B Moslemi A Bandeghani A Faeli L Shokohi T Roilides E A systematic review and disability-adjusted life years of Scedosporium/Lomentospora infection in patients after near-drowning Mycoses 2024672 e 137033834526510.1111/myc.13703 · doi ↗ · pubmed ↗
- 8Troke P Aguirrebengoa K Arteaga C Ellis D Heath CH Lutsar I Rovira M Nguyen Q Slavin M Chen SCA Treatment of Scedosporiosis with voriconazole: Clinical experience with 107 patients Antimicrob Agents Chemother 2008525174317501821211010.1128/AAC.01388-07PMC 2346616 · doi ↗ · pubmed ↗