Intraoperative Abdominal Penetration of the Lag Screw: A Rare Complication During Proximal Femoral Nail Anti‐Rotation Surgery
Mohammad Javad Dehghani Firoozabadi, Ramin Bozorgmehr, Fatemeh Bastan, Maryam Rashidian

TL;DR
This paper reports a rare surgical complication where a lag screw used in PFNA surgery accidentally penetrates the abdomen.
Contribution
The paper highlights a previously uncommonly reported intraoperative complication of PFNA surgery involving abdominal penetration by a lag screw.
Findings
Intraoperative abdominal penetration by a lag screw is a rare but critical complication of PFNA surgery.
Surgeons should be aware of this unique complication to prevent osteosynthesis failure.
The case underscores the technical challenges associated with PFNA use.
Abstract
Although the proximal femoral nail anti‐rotation (PFNA) is accompanied by several benefits, using the nail is technically challenging and may pose some errors, leading to osteosynthesis failure. Here, we report a critical presentation of an uncommon side effect of PFNA surgery. Intraoperative abdomen penetration via lag screw is a unique complication of PFNA surgery of which surgeons should be aware.
Click any figure to enlarge with its caption.
 FIGURE 1
FIGURE 1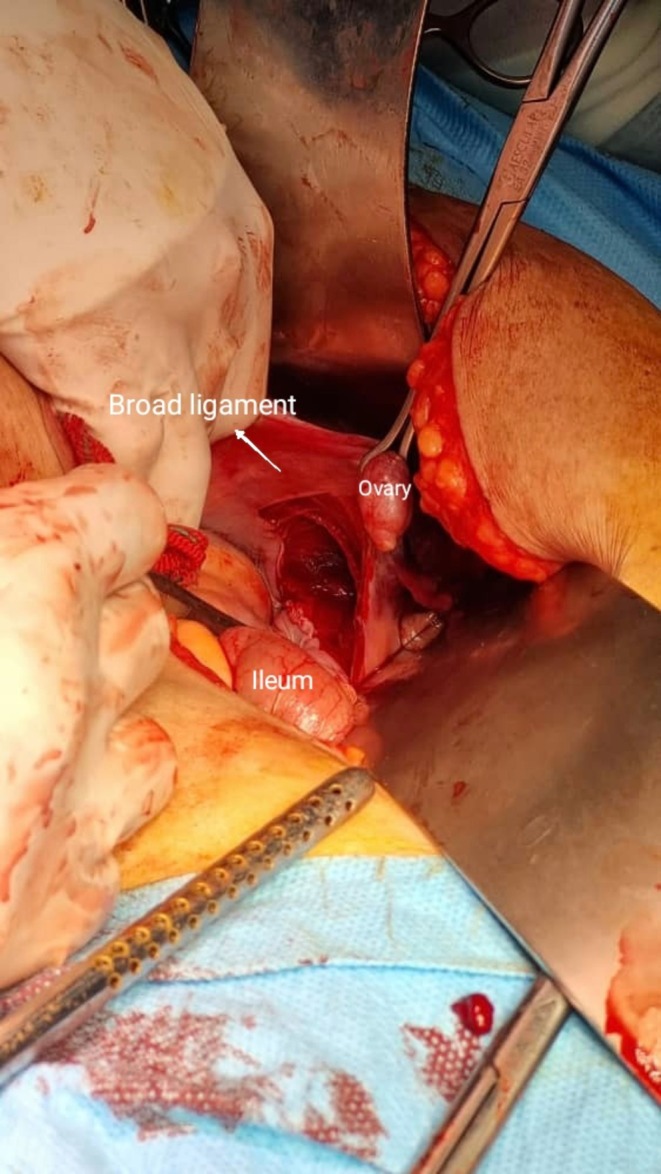 FIGURE 2
FIGURE 2| Day | Event | Intervention |
|---|---|---|
| Day 0 | Fall → Intertrochanteric fracture (31‐A1) | Hospitalization, IV heparin |
| Day 5 | Surgery → Intraoperative screw migration to abdomen | Exploratory laparotomy → screw removal → successful revision |
| Day 5 | ICU admission | Hemodynamic monitoring |
| Day 16 | DVT diagnosis | Enoxaparin 60 mg SC BD |
| Day 17 | Pulmonary embolism | |
| Day 21 | HIT (Platelets: 60,000/mm3) |
Switch to Apixaban Enoxaparin with prophylactic dose |
| Day 26 | Discharge | |
| Day 31 | Resuscitation attempted |
| Author | Year | Procedure | Treatment | Complications |
|---|---|---|---|---|
| Dimitrios Papanikolopoulos et al. [ | 2022 | A 50‐year‐old woman was treated with proximal femoral nailing after she suffered a left pertrochanteric fracture. She returned nine months later, complaining of agony and being unable to support her own weight. Imaging demonstrated the lack of fracture fixation and the hip screw's mechanical failure. | A left hip hemiarthroplasty and the removal of the damaged hardware were part of the revision procedure | The hip screw's mechanical failure and the loss of fracture fixation |
| Prasoon Kumar et al. [ | 2024 | A year after surgery, a 45‐year‐old man who had a subtrochanteric femur fracture that had been first treated with a short PFN was found to have a fractured implant and non‐union | The proximal nail portion was extracted using a typical technique during revision surgery. A beaded guidewire was used to retrogradely extract the distal portion through a lateral cortical window, avoiding the knee joint, while the central fragment was accessible and removed at the fracture site. Following the insertion of a long Proximal Femur Nail Antirotation (PFNA), bone grafting was carried out | A damaged implant and non‐union 1 year after surgery |
| Xiao‐Kun Chen et al. [ | 2022 | An 84‐year‐old woman suffered an intertrochanteric fracture after falling at home had PFNA used as the intramedullary fixation device during surgery. The helical blade's medial migration, which ultimately resulted in pelvic perforation, was discovered during postoperative inspection. | The savage treatment we used was a cemented total hip arthroplasty. The patient experienced no pain or loosening of the left hip prosthesis at the most recent follow‐up, which was 12 months following total hip replacement | Helical blade movement that ultimately resulted in pelvic perforation |
| Mayur Nayak et al. [ | 2019 | After a fall radiograph revealed an unstable left intertrochanteric fracture of the left hip, a 65‐year‐old man complained of excruciating left hip discomfort. PFNA‐II was used for internal fixation and a closed reduction. But 3 months after surgery, the patient complained of left hip pain when walking. The helical blade was perforated through the femoral head without any reduction loss, according to a follow‐up radiograph | After planning and executing a second surgery to remove the nail, it was discovered that the fracture had connected during the procedure | The helical blade's penetration through the femoral head |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone fractures and treatments · Total Knee Arthroplasty Outcomes · Surgical site infection prevention
Introduction
1
The intertrochanteric femoral fracture in elderly patients is common with increased marked incidence in recent years as societies grow continuously older. Several clinical and biomechanical studies have evaluated different implants such as the dynamic hip screw (DHS), the Gamma nail (GN), and the proximal femoral nail (PFN) [1]. The proximal femoral nail anti‐rotation (PFNA) system is a new device introduced by the AO/ASIF in 2003. The PFNA implant includes a helical blade for improved antirotation stability [2].
The advantages of osteosynthesis using the PFNA include the option of either static or dynamic distal locking, an unreamed insertion approach, and good rotational stability of the head–neck fragment. Even though PFNA is technically challenging, it produces impressive results when used correctly and with the proper technique. The most vital elements for a successful outcome are a non‐varus reduction, correct nail insertion, and precise lag screw placement. A stable biomechanical reduction by closed, percutaneous, or open methods is essential for effectively managing unstable intertrochanteric fractures [3, 4, 5, 6].
However, the use of nails is technically difficult and carries a high risk of surgical error and complications. These can include: a damaged implant and non‐union 1 year after surgery; helical blade movement that ultimately led to pelvic perforation; helical blade penetration through the femoral head and ultimately result in osteosynthesis failure; and the hip screw's mechanical failure and loss of fracture fixation [7, 8, 9, 10].
Despite adherence to surgical principles (anatomic reduction, precise nail insertion, and optimal lag screw placement), critical failures may occur. Key risk factors for screw migration include osteoporotic bone, fluoroscopic misinterpretation, over‐reaming or eccentric screw trajectory, excessive screw length, and anatomic variants [11].
We present the first case of intra‐abdominal PFNA lag screw penetration during surgery, occurring despite real‐time fluoroscopy. This highlights the limitations of intraoperative imaging and the need for tactile feedback and multiplanar verification. This report has been reported in line with the SCARE criteria [12].
Case History/Examination
2
An 87‐year‐old woman was referred to emergency with chief complaints of hip trauma as a result of falling four stairs in the dark. Her past medical history was only significant for essential hypertension and coronary angiography. Her drug history was positive for daily atenolol and atorvastatin consumption. Her habitual, allergy, and past surgical history were negative. On examination, vital signs were detected to be within the normal range. Her right leg had no laceration. It was tender to touch, and she was unable to raise it. Distal pulses were palpable and in the normal range. Other limbs were normal on examination and not damaged.
Methods (Differential Diagnosis, Investigations and Treatment)
3
Radiography revealed a right femur intertrochanteric fracture hip (AO/OTA classification 31‐A1) (Figure 1A). The patient was hospitalized. Intravenous heparin and acetaminophen as well as oral pantoprazole were initiated for her. Given the patient's preexisting cardiac disease and preoperative hemoglobin level of 9.1 g/dL, we administered 2 units of packed red blood cells based on our institutional protocol for high‐risk surgical patients. The surgery was performed under general anesthesia in supine position on a fracture table with manual traction. Antibiotic prophylaxis (cefazolin 1 g IV) was administered 30 min preoperatively. The procedure was conducted by a third‐year orthopedic resident under direct supervision of a senior trauma surgeon. During surgery, the femur was reset. The PFNA implant (manufactured by Mobtakran Co., Tehran, Iran) with a 240 mm nail length and 100 mm lag screw was placed. PFNA with a 240*12 mm short nail and 100 mm lag screw was placed with standard instructions. While fixing lag screw in the femur intraoperatively, we encountered unexpected screw migration into the abdominal cavity despite fluoroscopic guidance. It entered the abdominal cavity passing through the right acetabulum, iliopsoas muscle, and broad ligament (Figure 1B). Immediately, the general surgeon of the operating room performed exploratory laparotomy and removal of the lag screw. The ileum, ovary, ureter, and other intra‐abdominal organs hadn't been damaged (Figure 2). A new lag screw was placed successfully (Figure 1C). After recovery, she was transferred to the intensive care unit for 4 days and then moved to the orthopedic ward.
(A) Pre‐operative X‐ray of a right femur intertrochanteric fracture. (B) Intra‐operative X‐ray indicating the lag screw migrated to abdomen through acetabulum. (C) Post‐operative X‐rays of the fracture treated with proximal femoral nail.
Exploratory laparotomy and removal of the nail. Despite penetration of the broad ligament, intra‐abdominal organs, including ileum, ovary, and ureter were not damaged.
Conclusions and Results (Outcome and Follow‐Up)
4
The patient's postoperative trajectory was dominated by the intraoperative recognition of abdominal screw migration, a rare but critical complication. Immediate exploratory laparotomy confirmed the lag screw had penetrated the acetabulum and iliopsoas fascia without visceral injury. The surgical team successfully revised the fixation under augmented fluoroscopic guidance.
Subsequent recovery was complicated by thromboembolic events, including deep vein thrombosis (DVT) diagnosed on postoperative day 7 and pulmonary embolism confirmed by CT angiography. Anticoagulation management was further complicated by heparin‐induced thrombocytopenia (platelets 60,000/mm^3^), necessitating transition to direct oral anticoagulation. Despite stabilization of these conditions, the patient ultimately succumbed to pulmonary embolism on postoperative day 26 (Table 1).
This case highlights three predictable risks in geriatric PFNA patients: (1) Thromboembolism: Due to immobilization and fracture‐associated hypercoagulability. (2) HIT: Secondary to heparin exposure. (3) Surgical complications: Osteoporosis and aberrant anatomy increased screw migration risk. Proactive measures (e.g., DOAC prophylaxis, preoperative CT pelvimetry) might mitigate these risks.
Discussion
5
Proximal femoral fractures and related operations are becoming more common, which leads to an increase in sequelae such as nonunion, osteonecrosis, loss of fixation, and peri‐implant femoral fractures [13, 14]. Although uncommon, proximal femoral nail failure can have severe consequences [15]. This case indicates the first report that the lag screw migrated to the abdominal region during PFNA surgery.
There are additional reports demonstrating the post‐operative nail migration. A fifty‐year‐old woman was described in one study as having a left pertrochanteric fracture, which was treated with proximal femoral nailing, and she was sent home. Nine months later, the woman returned to the emergency room complaining of pain and being unable to bear her weight. Imaging showed that the hip screw had mechanically failed and that the fracture fixation had been lost [10]. In another study, a 72‐year‐old man who had fallen and was experiencing excruciating hip pain visited Busan Veterans Hospital. An unstable trochanteric fracture of the right femur was revealed by plain radiography. He did not have any trauma, and two months following the PFN surgery, he presented with moderate to severe right hip discomfort. Radiographs revealed that the lag screw had punctured the pelvis through the acetabulum and femoral head [16]. Our study illustrated an 87‐year‐old woman with a right intertrochanteric femur fracture who underwent PFNA surgery, which resulted in the device entering her abdomen. Other similar cases to ours have reported post‐operative device displacement as a problem. However, in our instance, this issue arose during the procedure and no other report have been published such complication in the literature (Table 2).
Even still, the exact reason for this event is still a mystery. This unusual complication may have been linked to some potential causes, including iatrogenic damage to the femoral head during reaming, improperly placed screws on the femoral head, early loading, exposing the implant to excessive torsional forces, direct trauma that results in a defect in the screw‐nail slot interface, misplacing the set screw in the proximal nail extremity, and selecting a cephalic screw that is either too short or too long [17, 18].
Conclusion
6
This case highlights a unique intraoperative complication of PFNA surgery—abdominal penetration by the lag screw and underscores the importance of meticulous surgical technique and immediate multidisciplinary intervention.
Author Contributions
Mohammad Javad Dehghani Firoozabadi: data curation, investigation. Ramin Bozorgmehr: conceptualization, supervision, writing – review and editing. Fatemeh Bastan: visualization, writing – original draft. Maryam Rashidian: software, writing – original draft, writing – review and editing.
Funding
The authors have nothing to report.
Ethics Statement
All ethical and moral issues have been considered in this study.
Consent
Written informed consent was obtained from the patient's legal next‐of‐kin after her passing, as documented in our institutional ethics committee records.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1J.‐S. Pu , L. Liu , G.‐L. Wang , Y. Fang , and T.‐F. Yang , “Results of the Proximal Femoral Nail Anti‐Rotation (PFNA) in Elderly Chinese Patients,” International Orthopaedics 33, no. 5 (2009): 1441–1444.19367404 10.1007/s 00264-009-0776-3PMC 2899136 · doi ↗ · pubmed ↗
- 2A. Raviraj , A. Anand , M. Chakravarthy , and S. Pai , “Proximal Femoral Nail Antirotation (PFNA) for Treatment of Osteoporotic Proximal Femoral Fractures,” European Journal of Orthopaedic Surgery & Traumatology 22, no. 4 (2012): 301–305.
- 3J. Windolf , D. A. Hollander , M. Hakimi , and W. Linhart , “Pitfalls and Complications in the Use of the Proximal Femoral Nail,” Langenbeck's Archives of Surgery 390, no. 1 (2005): 59–65.10.1007/s 00423-004-0466-y 15088148 · doi ↗ · pubmed ↗
- 4A. S. R. Kund , G. K. Boddana , C. Patnala , and R. Yalamanchili , “Parameters Governing the Fate of Fracture Fixation With Proximal Femoral Nailing (PFN) for Intertrochanteric Femur Fractures,” Cureus 15, no. 6 (2023): e 40952.37503460 10.7759/cureus.40952 PMC 10368960 · doi ↗ · pubmed ↗
- 5M. Y. Gökmen , M. Uluöz , H. O. Varmış , and H. Çiçek , “Comparison of Three Methods of Greater Trochanter Fixation in Intertrochanteric Femur Fractures (AO Type 31/A 2) Treated With Cementless Bipolar Hemiarthroplasty,” Journal of Cukurova Anesthesia and Surgical Sciences 7, no. 3 (2024): 195–199.
- 6H. O. Varmış , M. Y. Gökmen , and İ. Tan , “A Retrospective Comparative Study of the Clinical and Radiological Outcomes of Intertrochanteric Fractures Treated With Proximal Femoral Nail Antirotation (PFN‐A) and INTERTAN Nail,” P Lo S One 20, no. 1 (2025): e 0316954.39761283 10.1371/journal.pone.0316954 PMC 11703086 · doi ↗ · pubmed ↗
- 7X. K. Chen , J. Xiong , Y. J. Liu , Q. Han , T. B. Wang , and D. Y. Zhang , “A Rare Complication of Pelvic Perforation by an Excessive Medial Slide of the Helical Blade After Treatment of an Intertrochanteric Fracture With Proximal Femoral Nail Anti‐Rotation: A Case Report and Literature Review,” Chinese Journal of Traumatology 25, no. 2 (2022): 118–121.34509352 10.1016/j.cjtee.2021.08.007PMC 9039463 · doi ↗ · pubmed ↗
- 8P. Kumar , S. Aggarwal , A. Gupta , A. Dadra , S. Patel , and V. Goni , “A Corticotomy‐Assisted Extraction for a Rare 3‐Part Broken Proximal Femoral Nail: A Case Report,” Journal of Orthopaedic Case Reports 14, no. 12 (2024): 13–17.10.13107/jocr.2024.v 14.i 12.5000 PMC 1163250139669035 · doi ↗ · pubmed ↗