Evaluating Medical Education Escape Rooms: A Scoping Review Using the Kirpatrick Model
Hannah Sturm, Garrett Brown, Eric A. Gantwerker, Samar A Hegazy, Hannah Sturm, Chaewon Kim, Hannah Sturm

TL;DR
Medical education escape rooms are engaging and effective for teaching, but more research is needed on their long-term impact.
Contribution
This scoping review evaluates the effectiveness of medical education escape rooms using the Kirpatrick model.
Findings
Escape rooms show positive reactions and improved engagement, satisfaction, and perceived learning.
Significant improvements in pre- to posttest scores were observed in 45% of studies.
Escape rooms were more effective than flipped classrooms and traditional lectures.
Abstract
Medical educators are increasingly exploring innovative strategies such as medical education escape rooms (MEERs), team-based games in which participants solve puzzles and complete tasks within a time limit to achieve a goal, to enhance learner engagement. This scoping review aimed to evaluate the utility of MEERs as a teaching method in medical education. A scoping review was conducted using PubMed, MedEdPORTAL, and Scopus. Inclusion criteria were studies published in the past 15 years, written in English, involving medical students and/or residents, and reporting measurable outcomes. Exclusion criteria included systematic reviews, proof-of-concept studies, and studies outside medical school or residency contexts. Titles and abstracts were screened, followed by full-text review by two independent reviewers (HS and GB). A total of 20 studies met inclusion criteria. Data were extracted…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
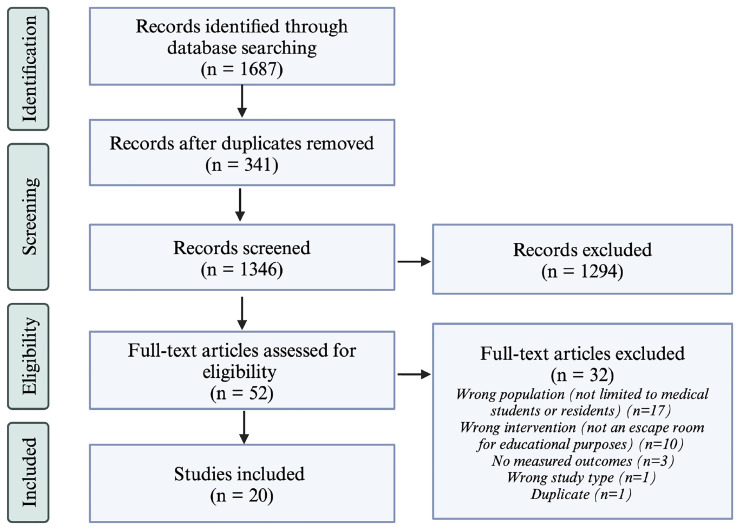 Figure 1
Figure 1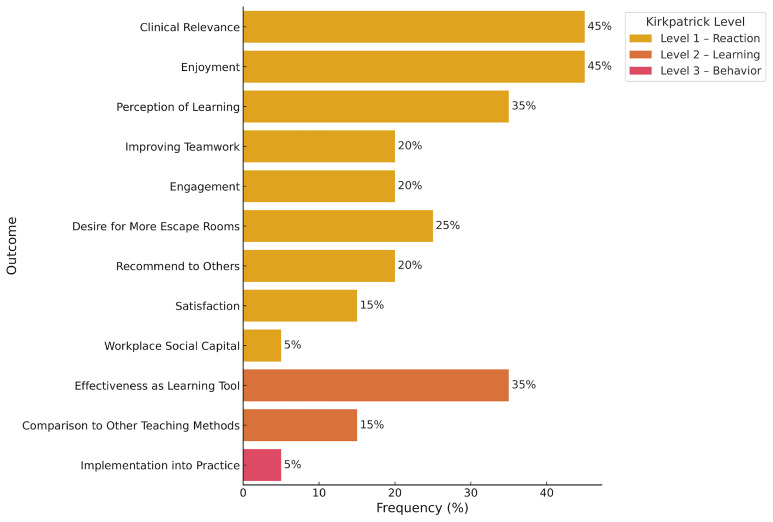 Figure 2
Figure 2| Review | Country | Aims | Escape Room
| Study Population | Sample
|
|---|---|---|---|---|---|
| Cantwell
| United
| Determine attitudes of students
| Virtual, serious
| 3
rd and 4
th year medical
| 134 |
| Cates
| United
| Test knowledge of toxicologic
| Virtual, serious
| Residents at a program
| 46 |
| Diemer
| United
| Educate incoming interns during
| In person,
| Interns from different
| 120 |
| Dimeo
| United
| Determine the value of virtual
| Virtual, gamification
| Emergency medicine
| 30 |
| Donovan
| United
| Assess the feasibility of teaching
| Virtual, serious
| 3
rd medical students
| 66 |
| Jaffe
| United
| Educate interns on identifying
| In person,
| Interns from 19 core
| 120 |
| Khanna
| United
| Determine the feasibility of an
| In-person,
| Internal medicine residents | 86 |
| Lundholm
| United
| Evaluate the effect of a
| In person,
| 1
st year internal medicine
| 52 |
| Martin & Gibbs (2022)
| United
| Explore the use of ERs in
| In person,
| Preclinical medical students | 148 |
| Podlog
| United
| Educate core emergency
| In person,
| Medical students and
| 30 |
| Zhang
| United States | Enhance active learning and
| In person,
| Interns attending
| 130 |
| Guckian
| United
| Determine the impact of ERs
| In person,
| 3rd year medical students | 101 |
| Faysal
| Pakistan | Evaluate the effectiveness of ERs
| In person, gamification only | 4th year medical students
| 97 |
| Liu
| United
| Create a pediatric radiology
| In person,
| Undergraduate medical
| 19 |
| Akatsu
| Japan | Determine the educational
| In person, serious
| 1st medical students
| 140 |
| Kinio
| Canada | Assess the effect of a vascular
| In person,
| 1st and 2nd year medical
| 13 |
| Backhouse & Malik (2018)
| United
| Use gamification to conduct
| In person,
| 3rd year medical students | 19 |
| Rosenkrantz
| Denmark | Determine the use of an ER for
| In person,
| Medical students with
| 49 |
| Jambhekar
| United
| Teach interesting content about
| In person,
| Incoming radiology
| 144 |
| Zhang
| United
| Determine the use of ERs to
| In person,
| Nine emergency medicine
| 10 |
| Measure | Study | Result | Sample
|
|---|---|---|---|
| Engagement | Cantwell
| 86% | 134 |
| Khanna
| Likert: 4.57 | 86 | |
| Zhang
| 41.18% | 130 | |
| Rosenkrantz
| 78% | 49 | |
| Enjoyment | Dimeo
| 78.57% | 30 |
| Donovan
| 92.4% | 66 | |
| Khanna
| 4.89/5 | 86 | |
| Guckian
| 100% | 16 | |
| Liu
| 94% | 19 | |
| Kinio
| 100% | 13 | |
| Rosenkrantz
| 98% | 49 | |
| Jambhekar
| Likert: 4.85 | 144 | |
| Zhang
| 100% | 10 | |
| Satisfaction | Cantwell
| 81% | 134 |
| Khanna
| Likert: 4.89 | 86 | |
| Jambhekar
| Likert: 4.85 | 144 | |
| Clinical Relevance | Cantwell
| 78% | 134 |
| Cates
| 54% | 46 | |
| Diemer
| 95.1% | 120 | |
| Jaffe
| 95% | 120 | |
| Khanna
| Likert: 3.78 | 86 | |
| Martin & Gibbs (2022)
| 82% | 148 | |
| Podlog
| 94% | 30 | |
| Backhouse & Malik (2018)
| 100% | 19 | |
| Zhang
| 100% | 10 | |
| Perception of Learning | Cantwell
| 84% | 134 |
| Cates
| 62.5% | 46 | |
| Donovan
| 93.9–97% | 66 | |
| Martin & Gibbs (2022)
| Likert: 4 | 148 | |
| Podlog
| 82% | 30 | |
| Kinio
| 75% | 13 | |
| Backhouse & Malik (2018)
| 100% | 19 | |
| Desire for More
| Cantwell
| 74% | 134 |
| Donovan
| 90.9% | 66 | |
| Khanna
| Likert: 4.38 | 86 | |
| Podlog
| 100% | 30 | |
| Liu
| 89.5 | 19 | |
| Recommend to Others | Cates
| 70.5 | 46 |
| Khanna
| Likert: 4.74 | 86 | |
| Rosenkrantz
| 85% | 49 | |
| Zhang
| 100% | 10 | |
| Workplace Social
| Lundholm
| 96% on pre-survey
| 246 |
| Improving Teamwork | Khanna
| Likert: 4.48 | 86 |
| Guckian
| 100% | 16 | |
| Kinio
| 100% | 13 | |
| Zhang
| 90% | 10 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInnovations in Medical Education · Simulation-Based Education in Healthcare · Medical Education and Admissions
Introduction
Medical educators are increasingly adopting innovative strategies to enhance learner engagement in both medical school and residency programs. One such strategy is gamification, the use of game elements in non-game contexts, which has been shown to improve motivation, satisfaction, and academic performance among health professions learners ^ 1 ^. In contrast, serious games are fully developed game-based experiences developed to achieve explicit educational or behavioral objectives, often simulating real-world environments for skill development and decision-making ^ 2 ^.
A hybrid of these two approaches is the Medical Education Escape Room (MEER), a team-based game in which players solve puzzles and complete tasks under time constraints. In medical education, MEERs have been implemented in diverse formats to suit various learning objectives. Some MEERs are designed as serious games, immersing learners in realistic, high-pressure clinical scenarios such as triage, infection control, and emergency response, thereby fostering critical thinking and teamwork under stress ^ 3, 4 ^. Others employ a more gamified approach, incorporating puzzles and challenges into classroom settings to reinforce curriculum content using game mechanics like point systems, collaboration, and immediate feedback ^ 5, 6 ^. Many MEERs integrate elements of both approaches, creating hybrid designs that combine immersive narrative scenarios with features such as time constraints, leaderboards, and competitive scoring to enhance learner engagement and motivation ^ 7 ^.
They have been used for purposes such as identifying and reporting safety hazards, setting patient safety priorities, assessing topic-specific knowledge, teaching clinical skills, improving teamwork, promoting well-being, and orienting new learners to clinical environments.
These tools have been used to teach both content knowledge and non-cognitive skills such as teamwork and communication ^ 4 ^. MEERs have also been adapted for various platforms, including in-person, virtual, and hybrid environments, demonstrating flexibility in curricular integration. They have been used for purposes such as identifying and reporting safety hazards and setting patient safety priorities ^ 8, 9 ^, assessing topic-specific knowledge ^ 10 ^, teaching clinical skills ^ 11 ^, improving teamwork ^ 12 ^, promoting well-being ^ 13 ^, and orienting new learners to clinical environments ^ 14 ^.
MEERs align with adult learning and experiential learning theories by offering immersive, learner-centered experiences that promote higher-order thinking, skill development, and knowledge application ^ 15 ^. Their gamified nature fosters intrinsic motivation and learner engagement, while the team-based format provides opportunities for peer learning and collaborative problem-solving in a low-risk setting.
To evaluate the effectiveness of such interventions, the Kirkpatrick Model provides a widely used framework encompassing four levels: reaction, learning, behavior, and results. Reaction assesses learner satisfaction and perceived value through post-activity surveys. Learning measures knowledge or skill acquisition, typically using pre- and post-tests. Behavior examines the application of learned skills in real-world settings, assessed through observation or follow-up surveys. Results evaluate the broader impact of the intervention on outcomes or institutional goals ^ 16 ^.
This study aimed to evaluate the utility of MEERs as a didactic tool in medical education through a scoping review. A preliminary search revealed no existing scoping reviews on this topic, highlighting a gap in the literature and an opportunity to synthesize and evaluate current practices, outcomes, and future directions for this emerging instructional strategy.
Materials and methods
Overview
The utility of MEERs in medical education was explored using a scoping review based on the methodology described by Arksey and O’Malley ^ 17 ^. A scoping review protocol was written to describe the search strategy and is available from the corresponding author upon request. This paper adheres to the JBI Scoping Review Network recommendations for the extraction, analysis, and presentation of results ^ 18 ^. The scoping review was performed in November 2022. IRB approval was not necessary for this study as there was no inclusion of human subjects.
Inclusion criteria
To be included, original peer-reviewed articles had to meet four criteria. First, the article had to be published in the last 15 years (since 2007). Second, the first version of the article needed to be in English. Third, the study population had to include medical students and/or residents in an accredited medical school or residency program either inside or outside the United States. Fourth, the study needed to have measured outcomes. Exclusion criteria included systematic reviews, proof-of-concept studies, and studies conducted in a healthcare discipline outside of medical school or residency.
Search strategy
The initial limited search of databases related to the use of MEERs in medical education showed that the databases PubMed, MedEdPORTAL, and Scopus were the most relevant to the topic and text words contained in the titles and abstracts and index terms were collected to describe the articles including “escape room”, “breakout room”, and “gamification”. Initial searches across all three databases showed that the term “breakout room” mostly applied to Zoom breakout rooms rather than ERs and “gamification” was too broad of a search term yielding many articles unrelated to ERs. Therefore, a second search using the search term “escape room” was conducted across the three included databases. Then, a reference list of all identified reports and articles was created. All identified articles from the searches were transferred to an online systematic review software for screenings (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia). The reviewers did not contact authors of primary studies or reviews for further information.
Selection of relevant and reliable studies
By applying the inclusion criteria, two reviewers (HS and GB) screened the articles on the reference list for selection ( Figure 1). The first screening was based on the title and abstract only and the second on a full-text review. All conflicts between the two reviewers that arose during the screening stages were discussed until an agreement was reached. If needed, a third reviewer was consulted to reach a consensus on including that article.
PRISMA Flow Diagram for the Scoping Review Process.The number of articles included after each step of the scoping review process is listed in parenthesis. On the right, the number of excluded articles is listed as well as the reasoning for article exclusion after full-text review. This figure was created using BioRender TM.
Extraction of the results
After the articles were selected from the second full-text screening, data was recorded in a Microsoft Excel spreadsheet. Variables collected included: author(s), year of publication, country of study, study aims or purpose, population and sample size, methodology, type and duration of the MEER, format (virtual or in-person), outcomes measured, and key findings. Outcomes and key findings were categorized according to the Kirkpatrick Model of Training Evaluation, which includes four levels: Reaction, Learning, Behavior, and Results.
Kirkpatrick Level 1 (Reaction) outcomes encompassed learners’ engagement, enjoyment, satisfaction, perceived clinical relevance, self-reported knowledge gain, desire for greater integration of MEERs into curricula, willingness to recommend MEERs to others, improvement in teamwork, and enhancements in workplace social capital (defined as the strength of social connections and trust within a professional setting). Kirkpatrick Level 2 (Learning) outcomes included performance on pre- and post-intervention assessments and comparisons to outcomes from traditional instructional methods. Kirkpatrick Level 3 (Behavior) outcomes addressed observed or self-reported behavioral changes following MEER participation ^ 16 ^.
Data analysis
Descriptive analysis of study characteristics and outcome measures was conducted using Microsoft Excel. For studies that reported the proportion of students endorsing specific outcome measures, the percentage of agreement and the corresponding sample size were recorded. For studies utilizing Likert scales (typically 5-point scales ranging from “strongly disagree” to “strongly agree”), the mean score and sample size were documented.
Results
Study selection
The initial search yielded 1,687 articles. After removing duplicates, 1,346 articles were screened by title and abstract by two independent reviewers (HS and GB), resulting in the exclusion of 1,294 articles. The remaining 52 articles underwent full-text screening, and 32 were subsequently excluded. A total of 20 articles met the inclusion criteria and were included in the final analysis and data extraction.
Article characteristics
Of the 20 included studies, 13 were conducted in the United States. Four studies evaluated MEERs implemented through virtual platforms. The study populations included residents in ten studies, medical students in nine, and both groups in one study. The publication years ranged from 2018 to 2022. The average number of participants per study was 73.1, and the average duration of the MEER activity was 43 minutes ( Table 1).
Purpose of escape room
The MEERs incorporated a range of game elements. Twelve studies implemented serious games with gamification components, seven used gamification elements only, and one used serious game elements exclusively. The number of puzzles per MEER ranged from 3 to 17, and nine studies allowed participants to receive hints to help progress through the activity. The MEERs addressed various educational goals: ten studies focused on reinforcing or assessing clinical knowledge and skills, five aimed to teach new content through team-based gamified learning, three emphasized safety education and hazard mitigation in clinical settings, and one focused primarily on team bonding.
Kirkpatrick model classification of training education
All studies evaluated the feasibility of MEERs using Kirkpatrick Level 1 outcomes, which assess learner reactions. In 45% of the studies, clinical relevance was examined, with 54–100% of participants agreeing that ERs were relevant to clinical practice (average Likert score: 3.78/5). Enjoyment was assessed in 45% of studies, with 92.4–100% of participants reporting enjoyment (average Likert score range: 4.85–4.89). Perceived learning was evaluated in 35% of studies, with 62.5–100% of learners indicating knowledge gain (average score: 4/5). Teamwork was assessed in 35% of studies, with 90–100% of participants reporting improved teamwork skills (average score: 4.48). Engagement was evaluated in 30% of studies, with 41.18–86% of participants feeling engaged (average score: 4.57). In 25% of the studies, desire for more MEERs in the curriculum was assessed, with 74–100% of learners expressing interest in additional sessions (average score: 4.38). In 20% of studies, participants were asked if they would recommend the MEER to colleagues; 70.5–85% responded affirmatively (average score: 4.74). Satisfaction was assessed in 15% of studies, with 81% of learners reporting satisfaction (average score range: 4.85–4.89). One study also measured workplace well-being before and after the MEER, showing an increase in workplace social capital from 96% to 100% (p = 0.003) ^ 13 ^ ( Table 2).
Nine studies (45%) evaluated Kirkpatrick Level 2 outcomes, which assess learning through pre- and post-intervention measures. Seven of these studies (35%) reported improvements in participant scores following the MEER activity ( Figure 2). For example, in studies focusing on safety hazard identification and reporting, mean confidence scores on a 10-point scale improved from 6.35 to 8.00 post-session (p < 0.001) ^ 8 ^. Another study showed a similar increase from 6.3 to 8.0 (p < 0.001) ^ 9 ^. Dimeo et al. reported that residents at two programs improved their quiz scores: University of California–Irvine residents improved from 77.8% to 88.9% (p = 0.028), and Prisma Health Upstate residents improved from 73.81% to 89.68% (p = 0.002) ^ 20 ^. Faysal et al. documented a score increase from 58% to 86% (p = 0.000) ^ 25 ^. One study assessed both immediate learning and retention after two weeks: pretest scores of 3.7/8 (range 2–6) increased to 7.3/8 (range 4–8) immediately after the session and remained at 7.3 (range 5–8) two weeks later ^ 26 ^. A dermatology-focused study showed an increase in confidence identifying skin conditions from 31.3% to 81.3%, and in performing systematic skin exams from 12.5% to 68.8% ^ 26 ^.
Escape Room Outcomes Based on Kirpatrick Levels of Education.Level 1 Outcomes are highlighted in yellow, Level 2 Outcomes are heighted in orange, and Level 3 Outcomes are highlighted in red. The percentage of articles discussing the outcome of interest is shown on the X axis. Note: Workplace Social Capital Score is a measurement of resident well-being. This figure was created by executing Python code in Google Colab TM.
Fifteen percent of the studies compared MEERs to traditional teaching methods such as flipped classrooms or case-based learning (CBL). These comparisons often showed greater improvements in learner performance with MEERs. For instance, Cantwell et al. found that average Likert scores for content clarity and effectiveness of educational materials in the MEER (3.6 ± 0.63 and 3.6 ± 0.63 respectively) were rated higher than in flipped classroom sessions on chest pain (3.5 ± 0.67 and 3.4 ± 0.77 respectively for the two categories) and abdominal pain (3.2 ± 0.77, 3.1 ± 0.80 respectively) (p = 0.0491; p<0.001) ^ 19 ^. Similar trends were observed in residency programs, where MEER participation led to improved quiz scores, while lecture-based activities did not yield significant gains ^ 20 ^. One study comparing MEERs with CBL found both methods equally effective, with a slightly higher improvement between pre and post test scores in the MEER group (48.3%) compared to the CBL group (48.2%) ^ 25 ^.
Only one study assessed Kirkpatrick Level 3 outcomes, which evaluate behavioral change. This study aimed to improve residents' understanding of patient safety priorities and voluntary event reporting systems. Six months after the intervention, there was no significant increase in the use of the reporting system compared to historical controls, indicating no measurable behavioral change. No studies assessed Kirkpatrick Level 4 outcomes, such as reductions in patient safety hazards as a result of the training.
Discussion
The use of MEERs has proven to be an engaging, motivating, and effective strategy in medical education. This scoping review shows that MEERs are consistently associated with positive learner reactions and educational outcomes among medical students and residents worldwide. Studies reported that learners were engaged, satisfied, and enjoyed the activity. Participants also found the experience relevant to their clinical training, gained knowledge and teamwork skills, and expressed interest in incorporating more MEERs into their curriculum. Many even recommended the activity to peers. Positive emotional responses such as enjoyment and enthusiasm are linked to academic success and improved cognitive processing ^ 31 ^, reinforcing the value of using MEERs as a tool to enhance learning and student well-being.
This scoping review illustrates that Medical Education Escape Rooms (MEERs) are not only consistently well-received but also demonstrate measurable educational benefits across multiple levels of the Kirkpatrick framework. Learner engagement, satisfaction, and enjoyment were near-universal themes, suggesting that MEERs are particularly effective in fostering positive emotional responses that are known to enhance motivation, cognitive processing, and academic success. These findings support the role of MEERs as a powerful pedagogical tool for enhancing the learner experience in both medical school and residency contexts.
Importantly, the review reveals that MEERs are not just entertaining games, but they are educationally effective. Nearly half of the included studies demonstrated significant improvements in knowledge or confidence through pre- and post-intervention assessments. These findings align with results from other health professions disciplines such as pharmacy and nursing ^ 32 ^, reinforcing the broader applicability of escape rooms as an interdisciplinary teaching modality. MEERs appear especially well-suited for reinforcing prior knowledge, clinical protocols, and team-based decision-making, areas where active learning and immersive environments offer distinct advantages over passive instruction.
Comparative studies further underscore the value of MEERs. When measured against flipped classrooms and traditional lectures, MEERs often yielded greater knowledge gains and learner satisfaction. This suggests that the integration of gamified and experiential elements may be more effective at stimulating critical thinking and long-term retention than conventional didactic approaches, which is supported by current educational theories supporting active learning ^ 33 ^. However, when compared to case-based learning, MEERs performed similarly, suggesting they may function best as complementary tools rather than outright replacements for traditional methods.
Despite their strengths, MEERs have not yet demonstrated consistent impact on behavior change (Kirkpatrick Level 3) or outcomes in clinical practice (Level 4). Only one study attempted to measure behavioral change, and it found no significant improvement in event reporting behaviors post-intervention. This points to a critical limitation of MEERs as currently implemented: while they may influence short-term learning outcomes, translating this knowledge into sustained behavioral change likely requires more than a single educational encounter. Structural, cultural, and institutional barriers may inhibit learners from applying new behaviors, especially in high-pressure or hierarchical environments. These findings suggest that for MEERs to drive long-term practice change, they may need to be embedded within longitudinal curricula, supported by follow-up reinforcement, mentorship, and systems-level alignment.
This review also highlights the versatility of MEERs across a range of educational objectives: they were used to introduce new concepts, review material, reinforce clinical protocols, identify safety hazards, and foster team bonding. Interestingly, Lopex-Pernas et al. found that students with stronger subject familiarity reported greater perceived learning, while MEERs aimed at teaching entirely new material received more critical evaluations ^ 34 ^. This may reflect the cognitive load imposed by complex escape room tasks, which can overwhelm learners unfamiliar with the foundational material. Future instructional design should consider sequencing MEERs after initial exposure to content or pairing them with preparatory learning activities to optimize educational value.
Despite their benefits, MEERs have practical limitations. They can be resource-intensive to design and implement. Time constraints may lead to superficial coverage of complex topics, and development requires substantial planning and facilitation. Physical materials can be costly and require maintenance, and space limitations may hinder realism. Additionally, poorly designed challenges or imbalanced group dynamics may reduce educational value. Moreover, MEERs may be less accessible or effective for individuals with disabilities, language barriers, or social anxiety.
To our knowledge, this is the first scoping review to systematically evaluate the use of Medical Education Escape Rooms (MEERs) specifically within undergraduate and graduate medical education, using the Kirkpatrick Model as a structured framework to classify outcomes. While previous studies have explored gamification or individual escape room interventions more broadly, this review is novel in its exclusive focus on MEERs designed for medical students and residents, offering a targeted synthesis of their educational value in clinical training contexts. By categorizing findings across reaction, learning, behavior, and results, this study not only highlights the consistent benefits of MEERs in promoting engagement and knowledge acquisition but also identifies a gap in evidence regarding long-term behavioral and clinical impact.
Limitations
One limitation of this study is that it was restricted to studies involving medical students and residents, excluding other healthcare trainees such as dental, pharmacy, and nursing students. As a result, the number of included studies was limited, particularly those evaluating long-term behavioral outcomes. Future research should explore MEER use across a wider range of healthcare disciplines to better understand their broader applicability. There are also limitations in using the Kirkpatrick Model to evaluate educational interventions. Measuring Levels 3 (behavior) and 4 (organizational outcomes) is challenging, especially in medical education. For example, assessing whether participants apply skills in clinical settings requires long-term observation, and attributing behavioral change solely to training is difficult due to ongoing clinical learning. Organizational shifts, such as system updates, may further confound results. Evaluating Level 4 outcomes demands significant time, resources, and expertise. Finally, the scoping review methodology has inherent constraints. While it provides a broad overview of the existing literature, it does not offer in-depth analysis or definitive answers to specific research questions. Furthermore, this review did not evaluate the methodological quality or risk of bias in the included studies, limiting its ability to offer concrete recommendations for practice or policy.
Conclusion(s)
Escape rooms are a valuable and versatile educational tool for teaching clinical concepts, reinforcing skills, and enhancing learner well-being in medical education. They consistently generate positive reactions and improve clinical knowledge and confidence. MEERs have outperformed traditional lectures and flipped classrooms and are as effective as CBL sessions, suggesting they could serve as an alternative or supplement within training programs. Most MEERs were used for reviewing content or reinforcing existing knowledge, which represents their most effective application. Further research should examine the feasibility and resources required to scale MEERs as CBL alternatives. While current evidence does not demonstrate consistent behavioral change, longitudinal studies are needed to explore their long-term impact on clinical practice and professional development.
Statements and declarations
Ethical considerations
Ethical approval was not required for this study as it involved the synthesis of existing, publicly available data and did not include human participants.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Subhash S Cudney EA : Gamified learning in higher education: a systematic review of the literature. Comput Human Behav. 2018;87:192–206. 10.1016/j.chb.2018.05.028 · doi ↗
- 2Graafland M Schraagen JM Schijven MP : Systematic review of serious games for medical education and surgical skills training. Br J Surg. 2012;99(10):1322–30. 10.1002/bjs.8819 22961509 · doi ↗ · pubmed ↗
- 3Shrivastava SR Shrivastava PS Joshi A : Escape rooms in medical education: unlocking realistic simulated clinical scenarios using interprofessional education. J Pharm Bioallied Sci. 2024;16(Suppl 3):S 2938–S 2940. 10.4103/jpbs.jpbs_1234_23 39346475 PMC 11426584 · doi ↗ · pubmed ↗
- 4Eukel HN Frenzel JE Cernusca D : Educational gaming for pharmacy students - design and evaluation of a diabetes-themed escape room. Am J Pharm Educ. 2017;81(7): 6265. 10.5688/ajpe 8176265 29109566 PMC 5663657 · doi ↗ · pubmed ↗
- 5Kinio AE Dufresne L Brandys T : Break out of the classroom: the use of escape rooms as an alternative teaching strategy in surgical education. J Surg Educ. 2019;76(1):134–139. 10.1016/j.jsurg.2018.06.030 30126728 · doi ↗ · pubmed ↗
- 6Moreno-Ger P Burgos D Martínez-Ortiz I : Educational game design for online education. Comput Human Behav. 2008;24(6):2530–2540. 10.1016/j.chb.2008.03.012 · doi ↗
- 7Hermanns M Deal B Campbell A : Using an “Escape Room” toolbox approach to enhance pharmacology education. J Nurs Educ Pract. 2017;8:89. 10.5430/jnep.v 8n 4p 89 · doi ↗
- 8Diemer G Jaffe R Papanagnou D : Patient Safety Escape Room: a graduate medical education simulation for event reporting. Med Ed PORTAL. 2019;15: 10868. 10.15766/mep_2374-8265.10868 32342008 PMC 7182042 · doi ↗ · pubmed ↗