Transient Neonatal Diabetes Mellitus Potentially Associated With a Novel Homozygous MS4A6A Gene Variant: A Case Report
Sohrab Shakeel, Sandeep Kadam, Sameer Pawar, Dhyey Pandya, Pragathi Kamath, Rahul Dawre, Kanchan Sakharkar, Abhinav Kachare, Sangeeta Chivale, Suvidha Sardar, Abhilash Yamavaram, Poonam Mane, Prakash Gambhir, Parag M Tamhankar, Salil Vaniawala, Aarti A Kinikar

TL;DR
A rare case of transient neonatal diabetes in a premature infant is linked to a new genetic variant in the MS4A6A gene, which may affect calcium signaling or islet inflammation.
Contribution
This is the first report linking a homozygous MS4A6A gene variant to transient neonatal diabetes mellitus.
Findings
A novel homozygous MS4A6A variant (c.162G>C; p.Leu54Phe) was identified in a patient with transient neonatal diabetes.
The patient achieved remission without ongoing insulin therapy after initial treatment.
The MS4A6A variant is extremely rare and predicted to be damaging, suggesting a potential role in diabetes pathogenesis.
Abstract
Neonatal diabetes mellitus (NDM) is a rare metabolic disorder characterised by hyperglycemia within the first six months of life. While commonly monogenic, the MS4A6A gene, known for immune modulation and calcium signalling, has not previously been linked to NDM. We report a case of transient NDM (TNDM) potentially associated with a novel homozygous variant in the MS4A6A gene. A male infant born at 27 weeks of gestation (720 g) developed severe hyperglycemia (>200 mg/dL) and polyuria on day 14 of life, following the resolution of suspected meningitis. Investigations confirmed insulin-deficient diabetes with low C-peptide (0.3 ng/mL) and negative antibodies. While standard NDM genetic panels were negative, whole-exome sequencing identified a homozygous MS4A6A variant (c.162G>C; p.Leu54Phe). Chromosomal microarray confirmed a region of loss of heterozygosity (LOH) at 11q12.1q12.2,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
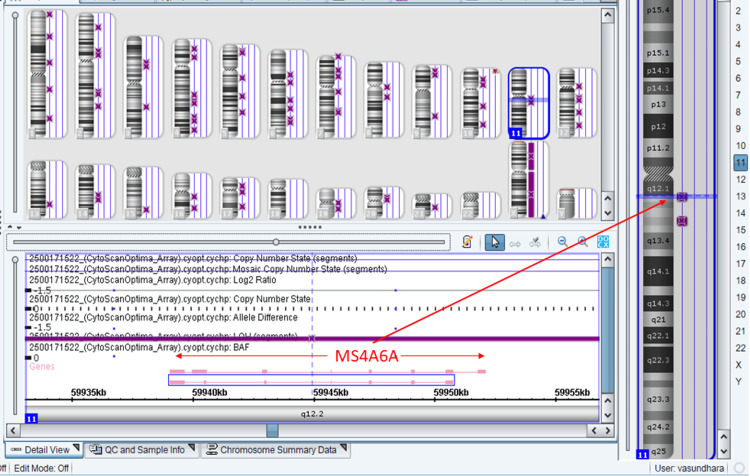 Figure 1
Figure 1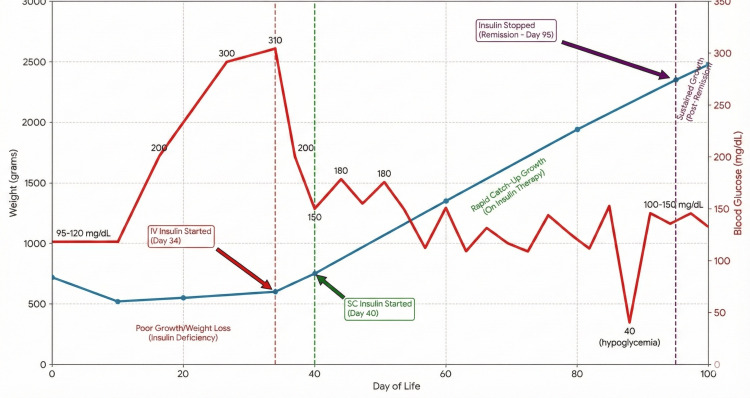 Figure 2
Figure 2| Parameter | Result | Reference Range | Interpretation |
| Blood Glucose | 260–320 mg/dL | 60–120 mg/dL | Hyperglycemia |
| Serum Insulin (Day 14) | 1.2 μIU/mL | 2–20 μIU/mL | Low (Insulin Deficiency) |
| β-Hydroxybutyrate | 4.1 mmol/L | <0.6 mmol/L | High (Ketosis) |
| C-Peptide | 0.3 ng/mL | 0.9–7.1 ng/mL | Low |
| CRP | 2 mg/L | <3 mg/L | Sepsis ruled out |
| Blood Culture | Negative | — | Sterile |
| ABG (pH/HCO3) | 7.42/22 mmol/L | 7.35-7.45/22-26 | No Acidosis (No DKA) |
| Microarray (CMA) | arr[hg19] 11q12.1q12.2 (59,014,657-61,457,857) hmz | Negative for Del/Dup | LOH/Identity by Descent |
| WES (Proband) | MS4A6A variant | Homozygous | Variant identified (VUS) |
| WES (Parents) | MS4A6A variant | Heterozygous | Carrier of variant |
| Serum Insulin (Day 97) | 3.97 μIU/mL | 2–20 μIU/mL | Normal (Restoration of Secretion) |
| Gene and Transcript | Location | Variant | Phenotype | In Silico Prediction | Clinical Significance |
| MS4A6A | Exon 3 | c.162G>C (p.Leu54Phe) (dbSNP: rs1258408007) | None reported | SIFT: Damaging PolyPhen-2: Poss. Damaging CADD: 24.5 | Uncertain Significance (VUS) (PM2)# |
| Sample | Gene | Location | Variant | Inheritance | Remark |
| Mother | MS4A6A ( | Exon3 | c.162G>C; p.Leu54Phe (Chr11:60179951) | -- | Present (Heterozygous) |
| Father | MS4A6A ( | Exon3 | c.162G>C; p.Leu54Phe (Chr11:60179951) | -- | Present (Heterozygous) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic function and diabetes · Diabetes and associated disorders · Diabetes Treatment and Management
Introduction
Neonatal diabetes mellitus (NDM) is a rare metabolic disorder characterised by hyperglycemia beginning within the first six months of life [1]. With an estimated incidence of one in 90,000-160,000 live births [2], it is broadly classified into two main groups: permanent neonatal diabetes (PNDM), which requires lifelong treatment, and transient neonatal diabetes mellitus (TNDM), where hyperglycemia spontaneously resolves, typically within the first few months, but carries a high risk of relapse in later life [3]. While PNDM is genetically heterogeneous [4,5], TNDM is most commonly associated with abnormalities at the 6q24 locus [3,6]. The etiology of NDM is predominantly monogenic, with mutations in the K-ATP channel genes (KCNJ11,* ABCC8*) and the insulin (INS) gene being the most common overall [7,8]. A precise genetic diagnosis is paramount, as it informs prognosis and therapy [9].
Despite these advances, a subset of NDM cases remains without a molecular diagnosis. The MS4A6A gene is part of the membrane-spanning 4-domains, subfamily A (MS4A) group, known for its role in immune modulation and function as a calcium-permeable ion channel [10]. Unlike typical NDM genes involved in beta-cell embryogenesis, MS4A6A is predominantly expressed in myeloid cells and is implicated in inflammatory regulation [10]. Herein, we present the first case of TNDM potentially associated with a homozygous variant in the MS4A6A gene. Trio-based sequencing and chromosomal microarray confirmed an autosomal recessive inheritance pattern driven by identity by descent (IBD) [11]. This report describes a potential new monogenic association for NDM, provides in silico and chromosomal evidence of pathogenicity, and proposes a novel pathophysiological mechanism involving transient inflammation and calcium flux dysregulation.
Case presentation
A male infant born at 27 weeks and six days of gestation (birth weight 720 g) was admitted to the neonatal intensive care unit (NICU). He was born to asymptomatic, non-consanguineous parents, though a significant polygenic risk for diabetes was noted in the family history. His early course was complicated by respiratory distress requiring intubation, Grade II intraventricular haemorrhage, and suspected meningitis. The infant was treated with a 21-day course of intravenous antibiotics, specifically meropenem and gentamycin.
Around day 10 of life, the infant developed polyuria and weight loss. On day 14, persistent hyperglycemia (>200 mg/dL) (Table 1) was noted. To rule out sepsis-induced stress hyperglycemia, a full septic workup was performed. Blood cultures were sterile, and the C-reactive protein (CRP) was 2 mg/L (normal <3 mg/L) (Table 1), effectively ruling out active infection as the primary cause. Additionally, arterial blood gas (ABG) analysis showed a pH of 7.42 and bicarbonate (HCO_3_) of 22 mmol/L (Table 1), ruling out diabetic ketoacidosis (DKA).
Endocrine investigations confirmed insulin-deficient diabetes with low serum insulin (1.2 μIU/mL) and C-peptide (0.3 ng/mL) (Table 1) alongside ketosis. A standard NDM genetic panel was negative. Whole-exome sequencing (WES) subsequently identified a novel homozygous variant in the MS4A6A gene (c.162G>C; p.Leu54Phe) (Table 2). Both parents were confirmed as heterozygous carriers (Table 3).
Functional genetic analysis
To validate the genomic context of the homozygous variant, a chromosomal microarray (CMA) was performed on the infant (Figure 1). The analysis showed no clinically significant deletion or duplication. However, it revealed a significant region of loss of heterozygosity (LOH) at arr[hg19] 11q12.1q12.2(59,014,657-61,457,857) hmz. This region encompasses the MS4A6A gene. This finding confirms that the homozygosity of the variant is due to IBD, likely resulting from shared distant ancestry between the parents, despite the lack of known consanguinity.
Chromosomal microarray (CMA) of baby
Allele frequency and in silico prediction
The identified variant (MS4A6A c.162G>C) is extremely rare, with an allele frequency of 1.2x10^6^ (two alleles out of 1,613,944) in the Genome Aggregation Database (gnomAD). In silico pathogenicity prediction tools suggest a deleterious effect: SIFT (Damaging), PolyPhen-2 (Possibly Damaging), and a high Combined Annotation Dependent Depletion (CADD) score (24.5), indicating high conservation and potential functional impact. Despite this, the variant is currently classified as a variant of uncertain significance (VUS) according to the American College of Medical Genetics and Genomics (ACMG) guidelines.
Insulin therapy was initiated on day 34 (intravenous) and transitioned to a subcutaneous basal-bolus regimen on day 40. This led to catch-up growth, requiring weekly upward titration of the insulin dose to match the infant's rapid weight gain [12,13]. However, by day 92 (Figure 2), insulin requirements decreased, and the patient developed spontaneous hypoglycemia. Insulin was discontinued on day 95. The patient maintained euglycemia off therapy, and a repeat serum insulin level of 3.97 μIU/mL (Table 1) confirmed the restoration of endogenous secretion. Consequently, the diagnosis was revised from PNDM to TNDM [3].
Weight gain and blood glucose level vs. day of lifeGraph illustrating the timeline of weight gain and blood glucose level in relation to therapeutic interventions (IV Insulin, SC Insulin) and the eventual discontinuation of therapy.SC: subcutaneous; IV: intravenous
Discussion
The most critical finding of this report is the identification of a homozygous MS4A6A variant as a potential candidate gene for TNDM. The pathogenicity of this finding is supported by the CMA results, which identified a copy-neutral LOH region at 11q12.1q12.2 surrounding the gene. This LOH confirms that the homozygosity is authentic and driven by IBD [11], refuting the possibility of a deletion-induced hemizygosity artifact.
Proposed pathophysiology
Unlike transcription factors (e.g., PDX1, PTF1A) that cause pancreatic aplasia, MS4A6A is not known to be involved in pancreatic embryogenesis. Instead, we propose two alternative hypotheses for the transient nature of the diabetes in this patient:
Transient Islet Inflammation
MS4A6A is highly expressed in macrophages and is a key regulator of immune signalling [10]. Dysfunction of this gene may have led to a localised, transient inflammatory response within the pancreatic islets (sterile insulitis), resulting in temporary beta-cell silencing (stunning) rather than permanent destruction. As the inflammatory stimulus resolved, beta-cell function recovered.
Defective Calcium Signalling
The MS4A family of proteins shares structural homology with the CD20 calcium channel and is involved in regulating calcium flux [10]. Since insulin secretion is strictly calcium-dependent [14], a defect in MS4A6A could impair intracellular calcium handling in beta-cells or associated immune cells, leading to a temporary secretory failure that resolved with maturation or compensatory mechanisms.
Limitations
We acknowledge several limitations in this report. First, the identified MS4A6A variant is classified as a VUS (PM2), and no functional studies were performed to definitively prove pathogenicity. Second, the extreme prematurity of the infant is a confounding factor, although the clinical course was more severe than typical stress hyperglycemia [15]. Future in vitro studies are required to validate the impact of this variant on calcium flux and islet inflammation.
Management and surveillance
Management must now focus on the high lifetime risk of relapse, particularly during metabolic stress [3]. Parents have been educated on "sick day" management [16]. Long-term surveillance is mandatory, including annual HbA1c and oral glucose tolerance tests [17]. Furthermore, the heterozygous parents face a "dual-risk" profile: their carrier status combined with a polygenic family history warrants proactive metabolic surveillance [17,18]. Finally, genetic counselling should be offered, noting the current VUS status of the variant and the IBD findings [19,20].
Conclusions
We report a case of TNDM potentially associated with a homozygous MS4A6A variant. Chromosomal microarray confirmed that the homozygosity was due to IBD within a region of LOH. We hypothesize that the mechanism involves transient islet inflammation or defective calcium signaling. This case identifies MS4A6A as a candidate gene for NDM, highlighting the need for functional validation and lifelong metabolic monitoring.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Neonatal diabetes mellitus: a disease linked to multiple mechanisms Orphanet J Rare Dis Polak M CavéH 12220071734905410.1186/1750-1172-2-12PMC 1847805 · doi ↗ · pubmed ↗
- 2Neonatal diabetes mellitus: an update on diagnosis and management Clin Perinatol Lemelman MB Letourneau L Greeley SA 41594520182940600610.1016/j.clp.2017.10.006PMC 5928785 · doi ↗ · pubmed ↗
- 3Transient neonatal diabetes: widening the understanding of the etiopathogenesis of diabetes Diabetes Temple IK Gardner RJ Mackay DJ Barber JC Robinson DO Shield JP 135913664920001092363810.2337/diabetes.49.8.1359 · doi ↗ · pubmed ↗
- 4Emerging roles for the TG Fbeta family in pancreatic beta-cell homeostasis Trends Endocrinol Metab Brown ML Schneyer AL 4414482120102038203010.1016/j.tem.2010.02.008PMC 2897975 · doi ↗ · pubmed ↗
- 5The effect of early, comprehensive genomic testing on clinical care in neonatal diabetes: an international cohort study Lancet De Franco E Flanagan SE Houghton JA 95796338620152623145710.1016/S 0140-6736(15)60098-8PMC 4772451 · doi ↗ · pubmed ↗
- 6Clinical presentation of 6q 24 transient neonatal diabetes mellitus (6q 24 TNDM) and genotype-phenotype correlation in an international cohort of patients Diabetologia Docherty LE Kabwama S Lehmann A 7587625620132338573810.1007/s 00125-013-2832-1 · doi ↗ · pubmed ↗
- 7Mutations in ATP-sensitive K+ channel genes cause transient neonatal diabetes and permanent diabetes in childhood or adulthood Diabetes Flanagan SE Patch AM Mackay DJ 193019375620071744653510.2337/db 07-0043 PMC 7611811 · doi ↗ · pubmed ↗
- 8Insulin gene mutations as a cause of permanent neonatal diabetes Proc Natl Acad Sci U S A Støy J Edghill EL Flanagan SE 150401504410420071785556010.1073/pnas.0707291104 PMC 1986609 · doi ↗ · pubmed ↗