Endoscopic ultrasound-guided hepaticogastrostomy using a novel double-lumen cannula designed for a 0.018-inch guidewire
Haruo Miwa, Ritsuko Oishi, Shotaro Tsunoda, Kazuki Endo, Yuichi Suzuki, Hiromi Tsuchiya, Shin Maeda

Abstract
Click any figure to enlarge with its caption.
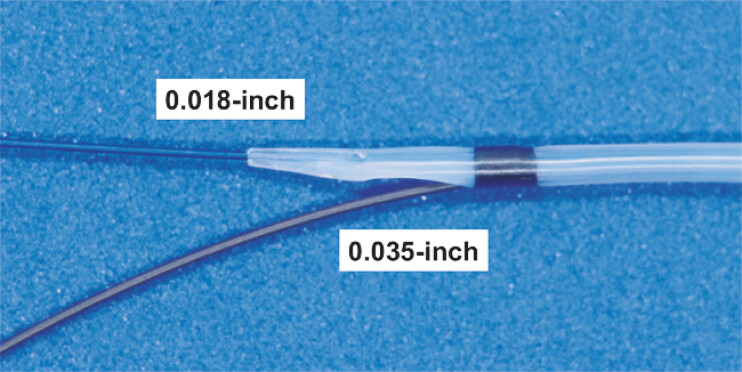 Fig. 1
Fig. 1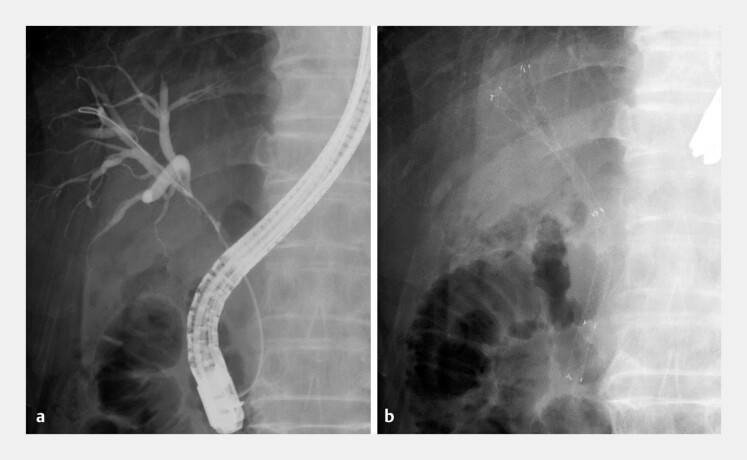 Fig. 2
Fig. 2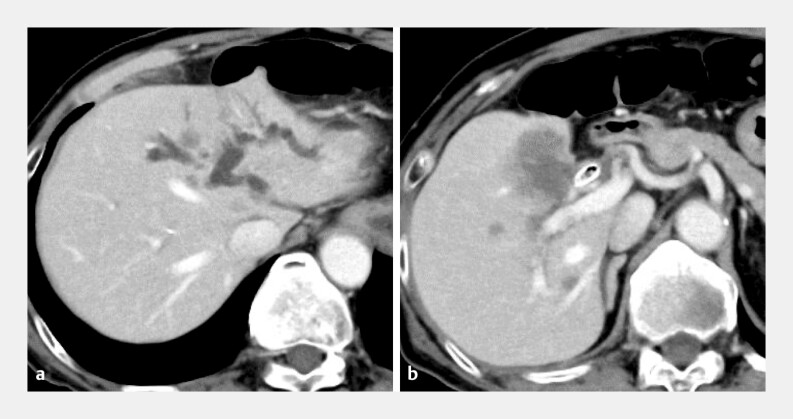 Fig. 3
Fig. 3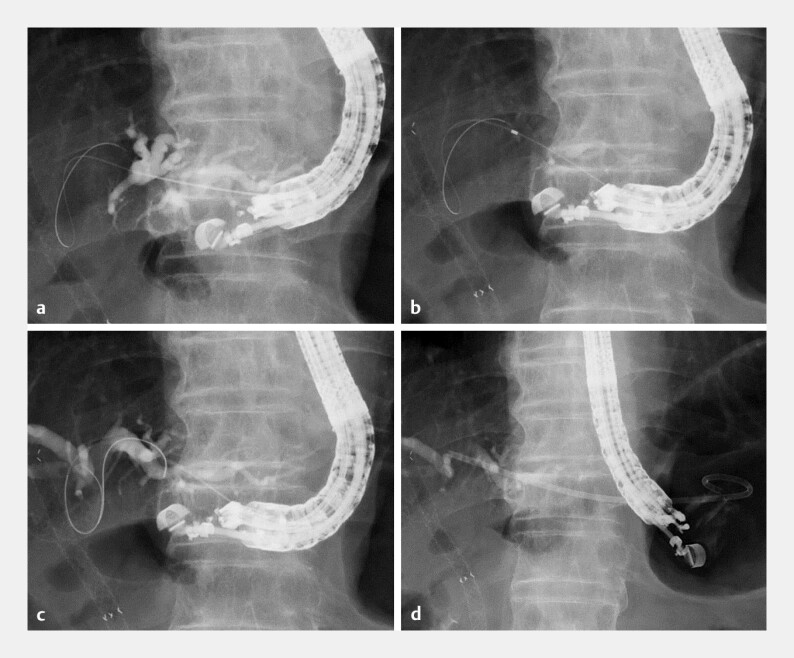 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Organ Transplantation Techniques and Outcomes · Hepatocellular Carcinoma Treatment and Prognosis
Endoscopic ultrasound-guided hepaticogastrostomy (EUS-HGS) using a 22-gauge needle and a 0.018-inch guidewire is well suited for bile duct puncture and initial guidewire insertion 1 2 ; however, subsequent tract dilation and stent delivery remain technically challenging. Although dilation devices compatible with a 0.018-inch guidewire have been reported 3 4 , tract dilation carries a potential risk of bile leakage. Furthermore, because no catheter specifically designed for a 0.018-inch guidewire has been available, switching to a stiff guidewire generally requires multiple device exchanges. This additional step may prolong the procedure and increase the risk of bile leakage 5 .
A novel uneven double-lumen cannula (UDLC; PIOLAX, Tokyo, Japan) features an ultra-tapered tip designed for a 0.018-inch guidewire and a side lumen for a 0.035-inch guidewire, with a maximum diameter of 6-Fr ( Fig. 1 ). This design enables effective bile aspiration while allowing one-step insertion of an additional stiff guidewire without device exchange, thereby improving procedural safety and stability while minimizing tract dilation.
A novel uneven double-lumen cannula (UDLC); PIOLAX, Tokyo, Japan) featuring an ultra-tapered tip designed for a 0.018-inch guidewire and a side lumen compatible with a 0.035-inch guidewire.
In the present case of EUS-HGS performed in a patient with hilar biliary obstruction and previously placed fully covered multi-hole metallic stents ( Fig. 2 and Fig. 3 ), a 0.018-inch guidewire (J-wire Premier Non-marker, J-Mit Co., Ltd, Kyoto, Japan) could not be advanced across the stents. Because of the short insertion length, a 0.018-inch guidewire alone was insufficient to provide adequate stability for stent delivery. Consequently, the novel UDLC was inserted over the 0.018-inch guidewire, enabling bile aspiration followed by insertion of an additional 0.035-inch stiff guidewire. Finally, a dedicated plastic stent (7-Fr, 10 cm, Through & Pass Type IT, Gadelius Medical, Tokyo, Japan) was successfully deployed without additional tract dilation ( Fig. 4 ; Video 1 ).
Initial drainage for hilar biliary obstruction caused by unresectable gallbladder cancer. a Cholangiography reveals a bismuth type IIIa stricture. b Fully covered multi-hole metallic stents are deployed in the right anterior and posterior branches.
Computed tomography findings before endoscopic ultrasonography-guided hepaticogastrostomy. a Markedly dilation of the intrahepatic bile duct in the left lobe. b Gallbladder cancer with invasion of the perihilar bile duct.
Endoscopic ultrasound-guided hepaticogastrostomy. a The intrahepatic bile duct (B3) is punctured with a 22-gauge needle, followed by a 0.018-inch guidewire. b The novel uneven double-lumen cannula is advanced smoothly, and bile aspiration is performed. c A 0.035-inch guidewire is inserted through the side lumen. d A 7-Fr dedicated plastic stent is successfully deployed.
EUS-guided hepaticogastrostomy using a novel uneven double-lumen cannula enabling bile aspiration and insertion of an additional stiff guidewire when advancement across pre-existing metallic stents is not feasible. EUS, endoscopic ultrasound.Video 1
To the best of our knowledge, this is the first report of EUS-HGS using the novel UDLC designed for a 0.018-inch guidewire. This device addresses the limitation associated with 22-gauge needle access during EUS-HGS.
Endoscopy_UCTN_Code_TTT_1AR_2AZ Endoscopy_UCTN_Code_CCL_1AZ_2AC
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hara K Okuno N Haba S How to perform EUS-guided hepaticogastrostomy easier and safer J Hepatobiliary Pancreat Sci 20202756356410.1002/jhbp.77432511837 · doi ↗ · pubmed ↗
- 2Ogura T Okuda A Ueno S Prospective comparison study between 19-gauge needle with 0.025-inch guidewire and 22-gauge needle with novel .018-inch guidewire during EUS-guided transhepatic biliary drainage (with video)Gastrointest Endosc 202296262268035300970 10.1016/j.gie.2022.03.013 · doi ↗ · pubmed ↗
- 3Yamada M Hara K Haba S Endoscopic ultrasound-guided hepaticogastrostomy using a novel drill dilator Endoscopy 202254 E 856E 85710.1055/a-1838-368235636451 PMC 9735340 · doi ↗ · pubmed ↗
- 4Ogura T Bessho K Kanadani T Endoscopic ultrasound-guided hepaticogastrostomy using a novel double-lumen tapered dilator combined with a 22-G needle Endoscopy 202557 E 169E 17039965767 10.1055/a-2530-3297 PMC 11835501 · doi ↗ · pubmed ↗
- 5Ishiwatari H Sakamoto H Doi T Prevention of adverse events in endoscopic ultrasound-guided biliary drainage DEN Open 20266 e 7014510.1002/deo 2.7014540416588 PMC 12098953 · doi ↗ · pubmed ↗