Beyond Asbestos: Malignant Pleural Mesothelioma Revealing Lynch Syndrome Through Mismatch Repair Deficiency
Stefanni Vivanco, Sebastian Vega, Angello Muguruza, Andrea Garzón, Sergio Daniel Zabaleta Orozco, Michael Hernández

TL;DR
A rare case links malignant pleural mesothelioma with Lynch syndrome, suggesting DNA repair defects may increase cancer risk from asbestos exposure.
Contribution
This case report highlights a novel connection between Lynch syndrome and mesothelioma through mismatch repair deficiency.
Findings
A 70-year-old woman with Lynch syndrome developed mesothelioma after asbestos exposure.
Loss of PMS2 expression confirmed a defect in DNA mismatch repair.
The case suggests impaired DNA repair may lower cancer risk thresholds in asbestos-exposed individuals.
Abstract
Lynch syndrome (LS) is a hereditary cancer predisposition condition. We report a rare case of malignant pleural mesothelioma occurring in a patient with this syndrome. The interplay between genetic susceptibility and environmental exposure remains underrecognized. We describe a case of a patient with multiple primary malignancies, including mesothelioma. A 70-year-old woman, with a history of endometrial, breast, and colorectal cancers, developed malignant pleural mesothelioma following 15 years of residence in a mining area with probable asbestos exposure. Immunohistochemistry revealed a loss of PMS2 expression, supporting a defect in MMR. This report documents an exceptional coexistence of malignant pleural mesothelioma and LS, suggesting that impaired DNA repair may lower the carcinogenic threshold for asbestos exposure. Clinicians should consider LS in patients with multiple or…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
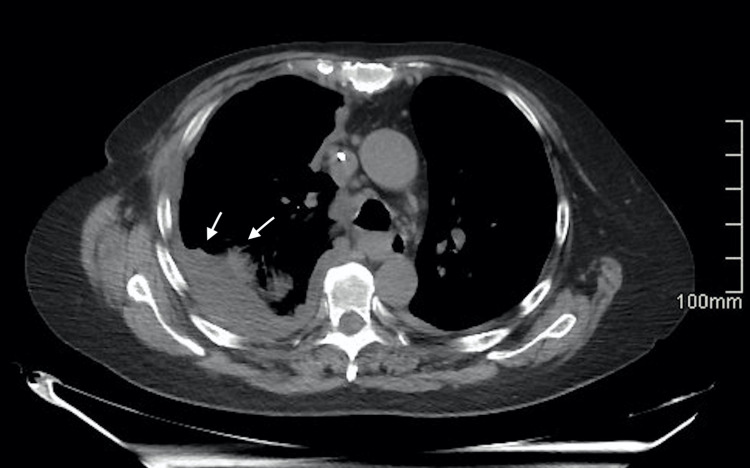 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGenetic factors in colorectal cancer · Occupational and environmental lung diseases · Multiple and Secondary Primary Cancers
Introduction
Lynch syndrome (LS), or hereditary non-polyposis colorectal cancer (HNPCC), is the most common cause of hereditary colorectal cancer and is associated with germline mutations in mismatch repair (MMR) genes (MLH1, MSH2, MSH6, PMS2, and EPCAM) [1,2]. It accounts for 2-4% of all CRC cases and confers a lifetime risk of 52-82% for developing the disease [3-5]. In addition, LS is linked to several extracolonic tumors, including those of the endometrium, ovary, skin, and, less frequently, the pleura [6-9].
The estimated incidence of LS is 1 in 300 individuals, likely underestimated due to limited systematic genetic screening [10]. Its clinical relevance lies in the predisposition to multiple primary neoplasms, which requires intensive surveillance [11-13].
Malignant pleural mesothelioma is a rare neoplasm; most of the approximately 30,870 global cases correspond to this location [13]. Although typically associated with asbestos exposure, cases linked to germline mutations in MMR genes, particularly MSH2, have also been reported [9,14]. This association complicates the differential diagnosis with pleural metastases and expands the recognized tumor spectrum of LS.
The present case is notable for the coexistence of multiple neoplasms: CRC, breast cancer, endometrial cancer, and pleural mesothelioma in the same patient, representing an unusual pattern within LS and highlighting the importance of recognizing atypical manifestations and performing genetic evaluation in families with multiple oncologic histories.
The aim of this report is to describe an atypical presentation of LS with pleural involvement, emphasizing the diagnostic and molecular implications and the need for expanded surveillance in high-risk families.
Case presentation
A 70-year-old woman with a history of endometrial cancer treated 20 years ago with radical hysterectomy, chemotherapy, and brachytherapy; right breast cancer operated on 10 years ago; and colon cancer 9 years ago treated surgically without systemic therapy due to an enterocutaneous fistula. She reported a strong family history of malignancies suggestive of a hereditary cancer syndrome. Among her siblings, one had two episodes of colorectal cancer and cutaneous squamous cell carcinoma, while two other siblings were each diagnosed with a single episode of colorectal cancer. In the second generation, one nephew had three episodes of colorectal cancer. Additionally, one niece was diagnosed with two episodes of colorectal cancer and endometrial cancer, and another niece had two episodes of colorectal cancer and biliary tract cancer.
She lived for 15 years in a mining area in Pasco, with chronic exposure to mining dust from blasting; asbestos exposure was suspected but not directly measured/confirmed.
During an outpatient follow-up, a non-contrast thoracic-abdominal-pelvic computed tomography (CT) scan identified subpleural pseudonodules smaller than 10 mm in the right lower lobe and a left laminar pleural effusion. A subsequent positron emission tomography-computed tomography (PET-CT) showed a right hilar mediastinal lymph node measuring 0.6 × 0.6 cm, suspicious for metastatic activity, along with bilateral laminar pleural effusion.
Video-assisted thoracoscopic surgery (VATS) was performed with resection of pulmonary nodules, mediastinal lymph nodes, and pleural biopsies (pleural and diaphragmatic). During the procedure, pleural carcinomatosis (visceral, parietal, diaphragmatic, and pericardial pleura), multiple mediastinal lymphadenopathies, and multiple pulmonary nodules were observed. Up to that point, she had only presented right-sided chest pain, without dyspnea or any other symptoms.
The mediastinal biopsy revealed soft tissue with mucoid material and isolated atypical epithelioid cells. The incisional lung biopsy showed pulmonary parenchyma and pleural surface with nodules of mucoid material and neoplastic proliferation of malignant epithelioid cells. The pleural biopsy demonstrated fibromuscular tissue with neoplastic proliferation of malignant epithelioid cells in a mucoid background.
Histopathological examination of the pleural biopsy revealed features consistent with epithelioid malignant mesothelioma. Immunohistochemical analysis of the tumor cells demonstrated positivity for CK7, WT1, and D2-40, with negativity for CK20, GATA3, PAX8, CDX2, TTF1, ER, SOX10, calretinin, and CD68, supporting the diagnosis of epithelioid malignant mesothelioma with areas of rhabdoid pattern. Given the patient’s personal oncologic history and a strong family history suggestive of a hereditary cancer syndrome, additional mismatch repair (MMR) immunohistochemistry was subsequently performed. This analysis demonstrated isolated loss of nuclear PMS2 expression, with preservation of MLH1, MSH2, and MSH6, consistent with mismatch repair deficiency and raising strong suspicion for Lynch syndrome. The diagnosis was established based on histopathologic evaluation and immunohistochemistry at the treating institution; an external confirmatory pathology review was not performed. Pleural thickening with nodules and bilateral pleural effusions were identified, as shown in Figures 1, 2.
A non-contrast thoracic CT scan identified diffuse tumoral thickening of the pleura in the right hemithorax
A non-contrast thoracic CT scan identified moderate right pleural effusion
The patient was treated with multiple thoracic drainages and chemotherapy. She received immunotherapy with nivolumab and ipilimumab. Notably, a first-degree relative (her brother) was later diagnosed with colorectal cancer and a cutaneous squamous cell carcinoma, both subsequently linked to Lynch syndrome, further supporting the familial nature of this condition.
Discussion
This case highlights the complexity of Lynch syndrome (LS), particularly when malignancies fall outside the classic tumor spectrum. The presentation of malignant pleural mesothelioma in a patient with confirmed LS-associated cancers, combined with similar malignancies identified in her brother, illustrates the interplay between genetic predisposition and environmental exposure in carcinogenesis. This case, therefore, provides an opportunity to examine how LS predisposition may modulate tumor behavior in the presence of environmental carcinogens.
Malignant mesothelioma is an aggressive neoplasm strongly linked to asbestos exposure, most commonly in occupational settings. Although globally rare [13], prolonged or repeated exposure to asbestos remains a well-established risk factor [15]. In this case, the development of mesothelioma introduces the critical environmental component. A large case-control study has demonstrated that asbestos exposure significantly increases the risk of malignant pleural mesothelioma, even in individuals without direct occupational contact [15]. This supports the evidence that low-level or para-occupational exposure can still be carcinogenic.
The patient’s long-term residence (15 years) in a mining zone with dust generated from blasting represents a plausible source of environmental asbestos exposure. Additionally, an ecological study of mesothelioma mortality in Peru identified elevated rates in regions with high mineral fiber importation, including Pasco, where the patient resided [16]. The timeline is consistent with known disease biology: mesothelioma typically manifests decades after initial exposure, aligning with the 15-year latency observed here [17].
The familial history further indicates LS as the underlying genetic disorder. Multiple first-degree relatives, including the patient’s brother, were diagnosed with colorectal and cutaneous malignancies associated with LS. The coexistence of endometrial, breast, colorectal cancer, and now malignant mesothelioma in the index patient underscores the broad phenotypic variability reported in LS [13,18].
Diagnosing malignant mesothelioma in this patient presented notable challenges. Notably, the tumor was negative for calretinin, an unusual finding given that approximately 90% of epithelioid malignant mesotheliomas express this marker [19]. However, rare calretinin-negative cases have been reported, underscoring the importance of using a broad immunohistochemical panel. The final diagnosis of epithelioid malignant mesothelioma was supported by characteristic histological features, including epithelioid morphology with rhabdoid areas. Immunohistochemical analysis demonstrated tumor cell positivity for WT1, D2-40, and CK7, with negativity for markers associated with alternative primary malignancies, including CK20, GATA3, PAX8, CDX2, TTF1, ER, SOX10, calretinin, and CD68, thereby excluding other potential primary sites.
The coexistence of mesothelioma, MMR deficiency, and environmental asbestos exposure suggests a synergistic carcinogenic effect. Shih et al. reported only two cases of LS-associated mesothelioma, both occupationally exposed [20], illustrating the rarity of this association. Our case strengthens the limited evidence by proposing a plausible mechanism: defective DNA mismatch repair may lower the carcinogenic threshold, allowing even modest or intermittent asbestos exposure to induce mesothelioma in genetically predisposed individuals.
Conclusions
We describe a rare occurrence of malignant pleural mesothelioma in a patient with Lynch syndrome, broadening the tumor spectrum associated with mismatch-repair deficiency. The coexistence of MMR-deficient malignancy and environmental asbestos exposure suggests a potential synergistic carcinogenic effect. Clinicians should consider LS in patients with multiple or atypical tumors, and genetic counseling should be offered to at-risk relatives. Further studies are needed to clarify how MMR defects modify susceptibility to environmental carcinogens.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Quadruple primary tumors in a lynch syndrome patient surviving more than 26 years with genetic analysis: a case report and literature review Front Oncol Zhu B Liu M Mu T 13821541420243889486410.3389/fonc.2024.1382154 PMC 11184617 · doi ↗ · pubmed ↗
- 2Instituto Nacional del Cáncer: Diccionario de cáncer del NCI 11 2025 2011 https://www.cancer.gov/espanol/publicaciones/diccionarios/diccionario-cancer/def/sindrome-de-lynch
- 3A brief review of Lynch syndrome: understanding the dual cancer risk between endometrial and colorectal cancer Oncol Rev Pallatt S Nambidi S Adhikary S 15494161920254045289210.3389/or.2025.1549416 PMC 12122774 · doi ↗ · pubmed ↗
- 4Hereditary colorectal cancer N Engl J Med Lynch HT de la Chapelle A 91993234820031262113710.1056/NEJ Mra 012242 · doi ↗ · pubmed ↗
- 5Metachronous cutaneous squamous cell carcinoma in a young patient as the only presenting symptom to uncover Lynch syndrome with MLH 1 Germline mutation Hered Cancer Clin Pract Khaddour K Fields RC Ansstas M Rosman IS Ansstas G 23182020 https://hccpjournal.biomedcentral.com/articles/10.1186/s 13053-020-00155-w 3329240910.1186/s 13053-020-00155-w PMC 7670704 · doi ↗ · pubmed ↗
- 6Hereditary nonpolyposis colon cancer (Lynch syndrome): an emerging public health concern Health Sci Rep Mohiuddin M 08202510.1002/hsr 2.71286 PMC 1244735040978308 · doi ↗ · pubmed ↗
- 7Síndrome de Lynch: aspectos genéticos, clínicos y diagnósticos Rev Gastroenterol Perú Castro-Mujica M del C Barletta-Carrillo C 265279382018 http://www.scielo.org.pe/scielo.php?pid=S 1022-51292018000300008&script=sci_arttext 30540731 · pubmed ↗
- 8Lynch syndrome: from multidisciplinary management to precision prevention Cancers (Basel) Dal Buono A Puccini A Franchellucci G 162024 https://www.mdpi.com/2072-6694/16/5/84910.3390/cancers 16050849 PMC 1093065738473212 · doi ↗ · pubmed ↗