Uptake of malaria vaccine (RTS,S/AS01) among children aged 6–24 months: A cross-sectional survey conducted in the Western region of Cameroon, 1 year following the vaccine introduction
Jerome Ateudjieu, Merveille Claire Nana Djapou, Benjamin Kevin Bekoa Onana, Abdias Aron Tatsabong Tiomeni, Gretta Ludivine Okoumokath Mpande, Donald Kapso Nanguep, Collins Buh Nkum, Dora Winny Ateudjieu Kenfack, Anne Cecile Bissek, André Siqueira, André Siqueira

TL;DR
A study in Cameroon found low uptake of a malaria vaccine in children, with parental perceptions significantly affecting vaccination rates.
Contribution
The study evaluates vaccine coverage and the influence of parental perceptions in two Cameroonian health districts.
Findings
Vaccination coverage for the first dose was 31.2%, with completion rates declining for subsequent doses.
Parental perception was strongly associated with vaccination uptake and timeliness.
Coverage indicators were below expected levels to significantly impact malaria reduction.
Abstract
Malaria vaccination using RTS,S/AS01 was introduced as part of Cameroon’s EPI to prevent malaria morbidity and mortality among children aged 6–24 months. This study aims to assess the coverage, completeness, and timeliness of this vaccine and to explore parental perceptions of children’s access to vaccination. This was a community-based, descriptive cross-sectional study targeting children aged 6–24 months and caregivers, selected by stratified random cluster sampling in Foumbot and Foumban health districts. Data were collected from caregivers by trained and supervised enumerators using a pretested questionnaire administered face-to-face. Malaria vaccine coverage, completeness, and timeliness were estimated with 95% confidence intervals. The contribution of caregivers’ perception on the first dose malaria vaccination status was explored by estimating crude odds ratio (cOR) and adjusted…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
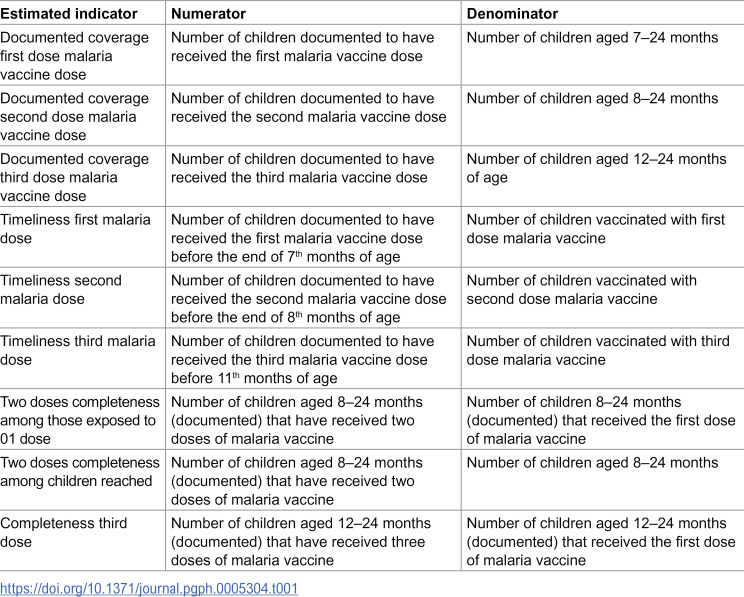 Figure 1
Figure 1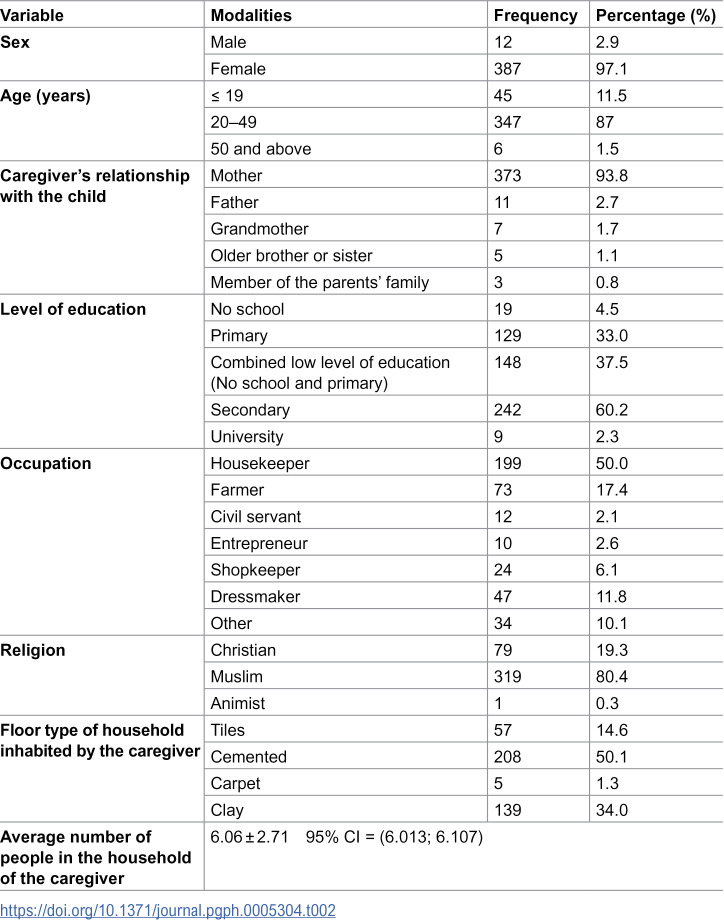 Figure 2
Figure 2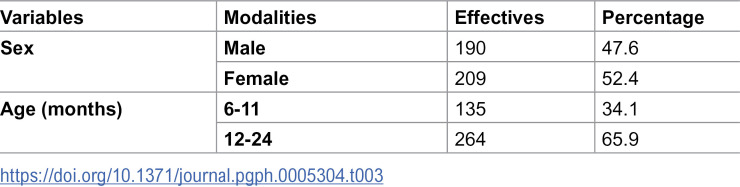 Figure 3
Figure 3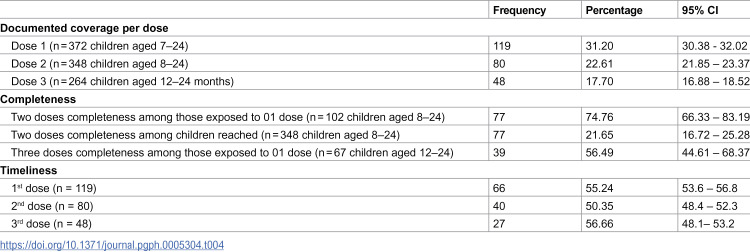 Figure 4
Figure 4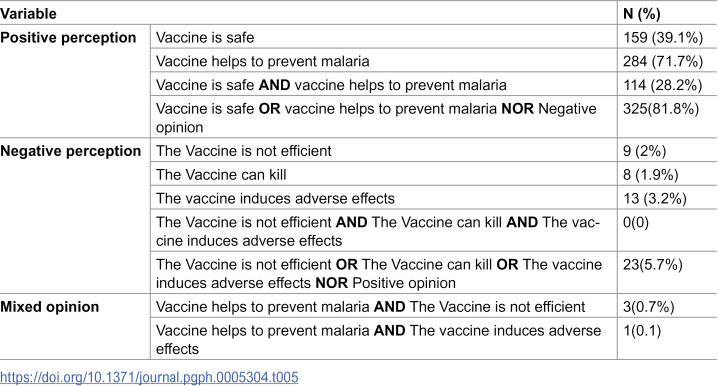 Figure 5
Figure 5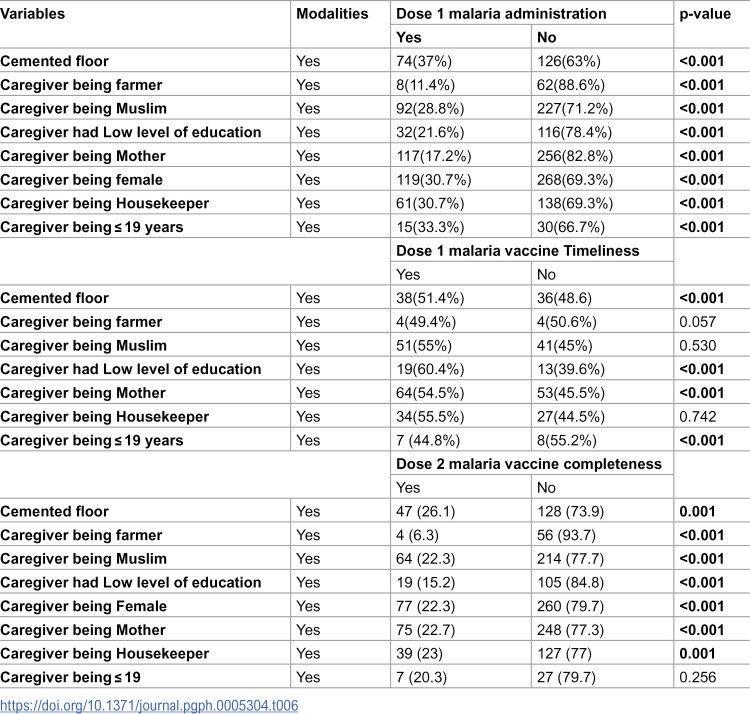 Figure 6
Figure 6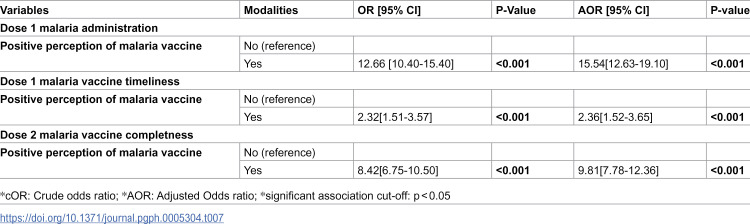 Figure 7
Figure 7- —Meilleur accès aux soins de santé (M.A SANTE), Cameroon
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMalaria Research and Control · Vaccine Coverage and Hesitancy · Immune responses and vaccinations
Background
Malaria remains a public health challenge worldwide, with the highest burden in Africa [1,2]. Several interventions have been prioritized to reduce the disease burden, including environmental interventions, the use of long-lasting mosquito nets, and prophylactic treatment for vulnerable groups such as pregnant women and children in malaria-endemic areas [3–6]. Although these interventions have contributed to a notable reduction in malaria morbidity and mortality, further efforts are required to achieve disease control [7]. In this context, vaccine development has led to the development of RTS,S/AS01, R21/Matrix-M, and PfSPZ vaccine. Among these, RTS,S/AS01 and R21/Matrix-M are currently recommended by the WHO [8–15].
Available literature documents the efficacy, safety, and benefits of malaria vaccination in various settings [7,11,16]. Evidence consolidated from pilot projects within the Expanded Program on Immunization (EPI) in Ghana, Kenya, and Malawi, along with subsequent WHO recommendations, supported the extension of malaria vaccination to other countries, including Cameroon [15–18]. This was followed by major reported challenges that included logistic difficulties, funding constraints, the complexity of administering the four-dose vaccine, and low caregivers’ adherence in some contexts [19,20]. In Cameroon, RTS,S/AS01 was introduced in 2024 as part of the expanded national immunization program targeting children aged 6–24 months in 42 health districts with the highest malaria burden in children. Ten month after the introduction, administrative data reported a 44.8% third-dose coverage [21]. Exploring this coverage and caregivers’ perceptions of malaria vaccination in households could generate evidence to guide interventions planning to reach the maximum number of targeted children.
Methodology
Ethics Statement
This study was conducted to generate evidence for the improvement of malaria vaccination in Cameroon. Its implementation involved household-based data collection from caregivers with the risk of increasing access to participants’ confidential data and compromising participant autonomy. All participants were informed of the study objectives and procedures and were included only after providing a written consent form. Participants’ confidentiality was protected by not collecting identifiable data, by password-protecting access to collected data, and by limiting access to the dataset to the team in charge of data management and analysis. The study protocol was reviewed and approved by the West Region Ethics Review Committee for Human Health Research in Cameroon (reference number N°/580/29/05/2024/CE/CERSH-OU).
Study design
This was a community-based descriptive cross-sectional study conducted from 5 to 13 May 2025, targeting children aged 6–24 months, selected by stratified random cluster sampling. Data were collected using a pretested questionnaire administered face-to-face to caregivers and a grid to review children’s vaccination booklets. Malaria vaccine coverage, completeness, and timeliness were estimated from the collected data.
Study setting
The study was conducted in the Foumban and Foumbot health districts in the West Region of Cameroon. At the time of the study, these were the only two districts in the region where the malaria vaccine was available under the EPI.
Study population
Children aged 6 to 24 months residing in either the Foumbot or Foumban health district were eligible. Those with caregivers consenting to participate were included. Children without caregiver available to provide data on vaccination status, or those living in health areas with recent insecurity, were excluded.
Sample size estimation
The minimum required sample size was estimated to be 392 mother-child couples. This calculation was based on an assumed a third-dose malaria vaccin coverage of 50%, a 95% confidence level, a 7% margin of error, and a cluster design effect of 2. Assuming approximately 7 children per cluster would be reached, the estimated sample was allocated across 55 clusters.
Sampling process
The sampling process was stratified by the population size of the Foumban and Foumbot health districts. Six and three health areas, respectively, were randomly selected to be part of the study. For each health area, a list of communities and their respective population sizes was obtained. Clusters were allocated proportionally to communities’ population size using a stratified systematic sampling approach. In targeted community participants of each cluster were selected by randomly choosing a starting household and a direction of recruitment. Households bordering the street were visited following the direction to identify and enroll study participants. Recruitment was considered completed in each cluster when approximately 7 children were included.
Data collection tools and variables
Data were collected using a questionnaire administered face-to-face and a grid to review vaccination cards. These tools were adapted from an existing questionnaire that was originally developed to assess documented and undocumented EPI vaccination coverage, timeliness, and completeness [22,23]. The main data collected included the sociodemographic characteristics of the mothers and children, the child’s malaria vaccination status, and the caregivers’ exposure to malaria vaccination information, and their perception of the malaria vaccination benefits and safety.
Data collection process
Data collection was performed by teams of three members including two trained enumerators and one trained supervisor. The teams were introduced by the supervisors in each household after obtaining the permission from the household head. If an eligible child (children aged 6–24 months) was present, informed consent was obtained from the caregiver. Data were then collected from the cargiver using a face-to-face administered questionnaire. If the child had vaccination booklet, a data extraction form was used to collect data on the vaccination status. Data were collected electronically using the Kobocollect mobile interface, uploaded online after verification by supervisors, and downloaded daily by the data management team for review. Queries were sent back to enumerators for corrections when necessary.
Data analysis
We estimated the documented vaccine coverage, timeliness, and completeness using numerators and denominators as presented in Table 1. The analysis was conducted using sampling weights. The individual weights corresponded to the ratio between the total population of each health area and the number of children actually surveyed in that area. Weighting allowed reconstruction of the target population distribution without further normalization. We explored the association between caregivers’ perception of the malaria vaccine on first malaria documented dose coverage and second dose malaria vaccine completeness using a case-control approach, estimating crude and adjusted odds ratios. Adjustment was done using mixed-effects logistic regression, with confounders identified from the comparison of key characteristics between cases and controls. Controls were children with documented vaccination, and cases were children with no documented vaccination. A positive perception was defined as reporting that “the vaccine is safe” OR “the vaccine helps prevent malaria” NOR any negative opinion. Conversely, participants who reported that “the vaccine is not effective” OR “the vaccine can kill” OR “the vaccine causes adverse effects” NOR any positive opinion were classified as having a negative perception. Individuals who reported that “the vaccine is safe” OR “the vaccine helps prevent malaria” AND “the vaccine is not effective” OR “the vaccine can kill” OR “the vaccine causes adverse effects” were classified as having a mixed perception and were excluded from the analysis. Data were analyzed using SPSS version 24.0 and R version 4.4.2. Estimates were reported with 95% confidence intervals.
Table 1: Definition of denominators and numerators for the estimate of the documented vaccine coverage, timeliness, completeness of the malaria vaccines uptake.
Results
Survey coverage
We reached the 55 targeted clusters and 399 participants, all of whom consented to participate, with average cluster coverage of 93.41% (95% CI 91.32-95.50).
Socio-demographic characteristics of caregivers and children
The mean age of the caregivers and children was 27.38 ± 7.45 years and 14.24 ± 5.41 months, respectively. Socio-demographic characteristics of the study population are presented in Table 2. The majority of caregivers (97.1%) were female; 11.5% were adolescents, and 37.5% had a low level of education. Table 3 presents the socio-demographic characteristics of the children.
Table 2: Socio-demographic characteristics of caregivers.
Table 3: Socio-demographic characteristics of children.
Vaccine coverage, completeness and timeliness
Of the 399 children reached, 208 (51.9%) were reported by caregivers to have received at least 1 dose of malaria vaccine, while 121 (29.8%) were documented to have received at least 1 dose of malaria vaccine.
Children’s vaccination coverage, timeliness, and completeness are presented in Table 4. Among included children, 48 (17.70%) were documented as having received the third dose of malaria vaccine. Of the 119 children who received the first dose, 46 (37.98%) completed the three-dose schedule. Timeliness rates for the three doses ranged from 50.34% to 56.66%.
Table 4: Malaria vaccine coverage, completeness and timeliness.
Caregivers’ perception of the malaria vaccine
Caregivers’ perception regarding the malaria vaccine is presented in Table 5. Of the 399 included caregivers, 325 (81.8%) had positive perceptions of vaccination.
Table 5: Caregiver perceptions of malaria vaccination.
Comparison of the distribution of socio-demographic characteristics between vaccinated and unvaccinated children
Table 6 presents the distribution of sociodemographic characteristics between vaccinated and unvaccinated children. There was a significant difference in sociodemographic characteristics between children who received the first dose of the malaria vaccine and those who did not. However, no significant differences were observed for caregiver age ≤ 19 years, occupation (farmer or housekeeper), or religion (Muslim) when comparing children who received the first dose on time with those who did not, or for second-dose completeness.
Table 6: Sociodemographic characteristics distribution between selected vaccination status of children.
Association between caregivers’ perception and vaccination status of children
Table 7 presents the contribution of malaria vaccine perception to children’s vaccination status. Children whose caregivers had a positive perception of the malaria vaccine were more likely to receive the first dose, to receive it on time, and to complete two doses.
Table 7: Bivariate association between malaria vaccine perception and vaccination status of children.
Discussion
To our knowledge, this is the first community-based survey exploring the coverage, completeness, and timeliness of malaria vaccination since its introduction in Cameroon. Our findings indicate documented vaccine coverage was 31.20% for dose 1, 22.61% for dose 2, and 17.70% for dose 3. The completeness of the second and third doses was 74.76% and 56.49%, respectively, and the timeliness of the first, second, and third doses was 55.24%, 50.35%, and 56.66%, respectively. Children’s exposure to caregivers with a positive perception of malaria vaccination were more likely to receive the first dose, receive it on time, and complete two doses.
Vaccination coverage reflects the proportion of the target population that has benefited from the intervention. It is also an indicator of vaccine demand and of the effectiveness of strategies implemented to reach the target vaccinated population. This study revealed that less than one-third of eligible children were documented as having received the first dose of the malaria vaccine. The second and third dose coverage of the malaria vaccination dropped to less than one-quarter and to less than one-fifth, respectively. In contrast, a study analyzing administrative data one month after the introduction of malaria vaccination in Cameroon by the national EPI in the 42 targeted health districts reported a first-dose malaria vaccine coverage relatively higher (37% of eligible children) than that observed in our study [24]. Furthermore, fourteen months after the introduction of the malaria vaccine in Cameroon, and one month before the data collection of this study, the cumulative three-dose malaria vaccination coverage from January to April 2025, as reported by the national Expanded Program on Immunization, was 64.3%, 54.1%, and 62.3% at the national level and 53.9%, 40.6%, and 42.2% in the two health districts targeted by our study for the first, second, and third doses of the malaria vaccine, respectively [25]. The discrepancies between administrative data and this study’s findings remain to be fully understood. They may be explained by several factors: children accessed during vaccination sessions are not rigorously selected from communities within the target health districts; our study estimated only documented vaccination; and there is a potential for error in estimating either the numerator or denominator used for administrative vaccination coverage.
The relatively higher malaria vaccination coverage observed after the vaccine introduction in other countries can be explained by better communication prior to the vaccination introduction, resulting in better adherence of the caregivers and/or by vaccination strategies [16,26]. The coverage observed in our study was below the expectation of the national Cameroon EPI [27]. Assuming that the malaria vaccine introduced in Cameroon (RTS,S/AS01) maintains its efficacy as reported in clinical trials, the three-dose vaccination coverage reported in our study predicts that nearly one in twenty children in the study districts will be fully protected by their first birthday. This underlines the urgent need, on one hand, to investigate the determinants of poor performance of malaria vaccination and, on the other hand, to implement documented interventions that have been shown to contribute to improve EPI coverage in similar contexts [23].
The vaccination completeness indicator is important for monitoring performance immunization programs [28]. It also provides information on the health system’s capacity to ensure optimal protection for vaccinated children, as vaccine effectiveness depends on full compliance with the recommended vaccination schedule for each given vaccine. Malaria vaccination completeness is necessary to maximize individual immunity and also to significantly reduce malaria morbidity and mortality in children [11]. In this study, half of the children who started the malaria vaccine completed the third dose. The observed high dropout rate in our study aligns with varying with varying levels of perceived importance of the malaria vaccine and other EPI vaccines as documented from studies conducted in similar and other contexts [29]. The present study was not designed to understand factors contributing to the malaria vaccination dropout rate, evidence from studies of other vaccines suggests that negative maternal attitudes toward vaccination, home birth, and limited geographic access may increase the risk of incomplete vaccination [30]. Further studies should explore the contribution of these factors to malaria vaccination completeness and other factors, such as the scheduling of vaccination sessions and the occurrence of adverse events after vaccination, which have been identified as inducing vaccination hesitancy [31]. The benefit of other caregivers’ reminders using SMS or tracking of children’s vaccination status in households by community volunteers to catch up on missed doses, shown to be beneficial for other vaccines, should be explored for their contribution to improving malaria vaccination completeness [23,31].
The timing and recommended interval between vaccine doses are based on the immune response and child development, as assessed through clinical trials and age-specific disease risks [32,33]. To our knowledge, no previous studies have assessed the timeliness of malaria vaccination in Cameroon. Like all EPI vaccines, malaria vaccination has an administration schedule, it lacks an operational definition of vaccination timeliness. In this study, we considered a dose timely if administered within one month of the recommended age. Under this definition, approximately half of the children received each dose on time. Comparing this trend with the timeliness of other EPI vaccines administered in the same context a few years earlier shows a higher timeliness rate for the BCG vaccine, which is administered at birth, and a timeliness rate consistent with our study for the DPT-Hi + Hb 3 vaccine, i.e., nearly half of children receiving the third dose of this vaccine within one month of the age recommended by the EPI [29]. This consistency likely reflects that nearly half of vaccinated children received the vaccine later than recommended. This delay is related to the supply or demand of all Expanded Program on Immunization (EPI) vaccines, not just the malaria vaccine, and must be addressed programmatically. Follow-up studies of children in high-risk areas show an increase in malaria incidence with time after each malaria vaccine dose, suggesting that some benefit of the malaria vaccine is lost when the vaccine administration schedule is not respected [11]. Making available an operational definition of the timeliness of each vaccine dose, conducting studies to understand low vaccine timeliness, and identifying interventions to improve it should guide the Expanded Program on Immunization to improve malaria vaccine timeliness.
Caregivers’ perception of children’s vaccination is expected to influence its demand for the benefit of children. In our study, a positive perception of the malaria vaccine was significantly associated with increase children’s access to the first malaria dose as well as the timeliness of the dose and the completeness of the second dose. To our knowledge, no published study has investigated the contribution of caregiver perception to malaria vaccines and children’s access to this vaccine. In Malawi, evidence in line with our finding was documented by showing the contribution of caregivers’ exposure to negative rumors about the malaria vaccine and a significant reduction of children’s likelihood of full uptake of the malaria vaccine [34]. This finding extend beyond malaria vaccine**;** a systematic review of general childhood vaccination revealed that negative perceptions of vaccines were significantly associated with non-use of vaccination [35]. Therefore, generating evidence on innovative interventions to improve caregivers’ perception of the malaria vaccine is expected to guide decision makers in taking needed action to improve malaria vaccine uptake in children.
The results of this study should be used taking into consideration the following limitations. Malaria vaccination coverage, timeliness, and completeness were estimated based on documented vaccination status. This could underestimate access to vaccination, as a given proportion of vaccinated children may be vaccinated without documentation [36].
Conclusion
In conclusion, the coverage, completeness, and timeliness of malaria vaccination are below the targets needed to achieve optimal vaccination benefits. Children’s exposure to caregivers with a positive perception of malaria vaccination increased their chance of receiving the first dose of the malaria vaccine, of receiving this dose on time, and of completing two doses of the malaria vaccine. We recommend that the competent health authorities in the targeted health districts implement communication initiatives aimed at improving caregivers’ perceptions on malaria vaccination; that scientists test innovative interventions to improve caregivers’ perceptions on malaria vaccination; and that other determinants of children’s access to malaria vaccination be explored to guide decision-making on promoting children’s access to the malaria vaccine.
Supporting information
S1 DataDatabase.(SAV)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO. Malaria 2024. https://www.who.int/news-room/fact-sheets/detail/malaria
- 2World Health Organization. Mobilizing communities to help prevent and control malaria in Cameroon. https://www.who.int/news-room/feature-stories/detail/mobilizing-communities-to-help-prevent-and-control-malaria-in-cameroon 2022.
- 3Li J, Docile HJ, Fisher D, Pronyuk K, Zhao L. Current Status of Malaria Control and Elimination in Africa: Epidemiology, Diagnosis, Treatment, Progress and Challenges. J Epidemiol Glob Health. 2024;14(3):561–79. doi: 10.1007/s 44197-024-00228-2 38656731 PMC 11442732 · doi ↗ · pubmed ↗
- 4Xu M, Hu Y-X, Lu S-N, Idris MA, Zhou S-D, Yang J, et al. Seasonal malaria chemoprevention in Africa and China’s upgraded role as a contributor: a scoping review. Infect Dis Poverty. 2023;12(1):63. doi: 10.1186/s 40249-023-01115-x 37403183 PMC 10320994 · doi ↗ · pubmed ↗
- 5González-Sanz M, Berzosa P, Norman FF. Updates on malaria epidemiology and prevention strategies. Curr Infect Dis Rep. 2023;1–9.10.1007/s 11908-023-00805-9PMC 1024898737361492 · doi ↗ · pubmed ↗
- 6World Health Organization. Global technical strategy for malaria 2016–2030. World Health Organization. 2015. doi: Users/HP/Downloads/Documents/global-technical-strategy-for-malaria-2016-2030.pdf 2015.
- 7Nadeem AY, Shehzad A, Islam SU, Al-Suhaimi EA, Lee YS. Mosquirix RTS, S/AS 01 Vaccine Development, Immunogenicity, and Efficacy. Vaccines (Basel). 2022;10(5).10.3390/vaccines 10050713 PMC 914387935632469 · doi ↗ · pubmed ↗
- 8Zavala F. RTS,S: the first malaria vaccine. J Clin Invest. 2022;132(1):e 156588. doi: 10.1172/JCI 156588 34981788 PMC 8718142 · doi ↗ · pubmed ↗