Infant HIV-protection: Comparing antiretroviral therapy, maternal and infant factors influence on infant HIV acquisition in Uganda: A six-year real-world experience
Collins Ankunda, Jude Emunyu, Brendah Kyomuhangi, Sharon Namasambi, Conrad Sserunjogi, Iving Mumbere, Jane Nakaweesi, Nisha Anne Sunny Jacob, Nisha Anne Sunny Jacob, Nisha Anne Sunny Jacob, Nisha Anne Sunny Jacob, Nisha Anne Sunny Jacob

TL;DR
This study from Uganda shows that infant feeding practices strongly influence HIV transmission, even with antiretroviral therapy.
Contribution
The study identifies infant feeding as a stronger predictor of HIV transmission than maternal factors in real-world PVT programs.
Findings
Mixed feeding and no breastfeeding strongly increase infant HIV positivity.
Maternal viral load non-suppression increases transmission risk.
Infant feeding models showed better predictive performance than maternal models.
Abstract
Although antiretroviral therapy (ART) scale up has markedly lowered vertical transmission, the relative contribution of ART regimens, maternal factors, and infant practices within Prevention of vertical transmission (PVT) programs is not fully understood. We assessed the comparative influence of maternal and infant factors on infant HIV positivity. We retrospectively reviewed records of 962 HIV exposed infants attending the Mildmay Uganda PVT clinic between 2018 and 2023. Of these, 918 were mother-infant pairs. Descriptive statistics summarised maternal and infant characteristics. Associations were assessed using Chi square or Fisher exact tests. Two independent logistic regression models identified infant and maternal factors associated with HIV positivity. Pseudo R² evaluated model performance and area under the curve measured discrimination. Among 918 mother-infant pairs, HIV…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
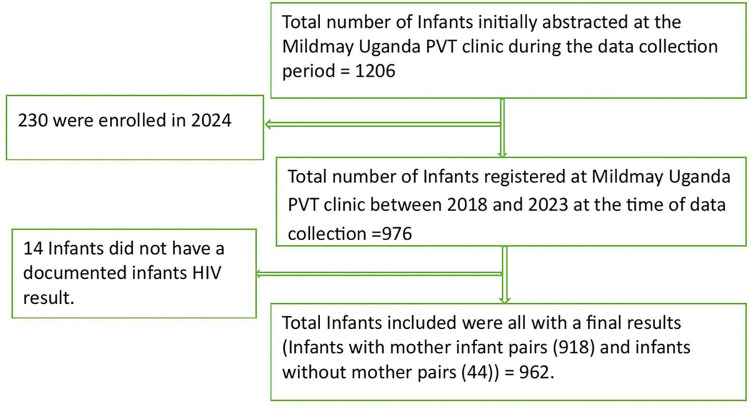 Fig 1
Fig 1- —http://dx.doi.org/10.13039/501100000683Royal Society of Tropical Medicine and Hygiene
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHIV/AIDS Research and Interventions · HIV/AIDS drug development and treatment · HIV Research and Treatment
Background
Globally, vertical transmission (VT) remains a major source of paediatric HIV infection, particularly in sub-Saharan Africa [1], where the burden of HIV is high. However, ART scale-up among pregnant women living with HIV (PWLH) has significantly reduced transmission risk during pregnancy, delivery, and breastfeeding. Without intervention, VT risk ranges from 15% to 45% [1], but with effective ART and comprehensive PVT measures, it can be reduced to under 5%, or even below 2% in some settings [1–3].
Several maternal factors influence the risk of vertical transmission during pregnancy and the postpartum period, including ART use, maternal viral load, overall health status, breastfeeding practices, and coexisting sexually transmitted infections (STIs), such as syphilis [4,5]. Among these, a high maternal viral load during pregnancy, delivery, or breastfeeding is a key driver of transmission [6]. Effective antiretroviral therapy (ART) regimens that achieve rapid and sustained viral load suppression are essential for preventing VT [7,8]. This highlights the importance of timely ART initiation, sustained adherence, and robust maternal healthcare systems, with a preference for regimens that reliably and quickly suppress viral replication [9,10]. Dolutegravir (DTG)-based regimens have become the preferred first-line treatment for PWLH due to their superior efficacy in rapidly suppressing viral load compared to previous regimens, such as efavirenz (EFV)-based combinations [2,11,12].
Infant feeding practices and maternal viral load are major determinants of postnatal vertical transmission risk [13,14]. Accordingly, breastfeeding plays a pivotal role in shaping postpartum transmission outcomes. The World Health Organization recommends exclusive breastfeeding for the first six months of life, followed by the introduction of appropriate complementary foods while continuing breastfeeding up to one year or beyond, contingent on sustained maternal viral suppression [15]. In parallel, infant antiretroviral prophylaxis, such as nevirapine, is tailored according to the infant’s level of HIV exposure risk [2]. Maintaining sustained maternal viral load suppression throughout the breastfeeding period remains critical to minimizing postnatal HIV transmission among HIV-exposed infants [10].
Although the effectiveness of postnatal PVT interventions is well established, existing studies largely assess the overall impact of ART and infant prophylaxis without disentangling the relative contributions of antepartum and postpartum interventions. Consequently, there is limited evidence directly comparing how interventions at different stages of the maternal–infant care continuum influence infant HIV outcomes. The study compared the impact of antepartum and postpartum factors that influence infant HIV positive status among PWLH on different ART regimens. By examining these factors across the continuum of care, the study aims to inform strategies to optimise PVT outcomes and advance progress toward the elimination of paediatric HIV in high-burden settings.
Methods and materials
Ethics statement
Ethical approval was obtained from the Mildmay Uganda Research Ethics Committee (#REC REF 0201–2024) and the Uganda National Council for Science and Technology (HS3873ES). A waiver of informed consent was granted by Mildmay Uganda Research Ethics Committee for the use of de-identified retrospective data. Administrative clearance was sought from MUgH administration to access participant data.
Study design
This was a retrospective cohort study that reviewed medical records of PWLH enrolled in the PVT clinic at the Mildmay Uganda Hospital (MUgH) from 2018 to 2023.
Study site and population
This study was conducted at MUgH, a peri-urban facility in Wakiso District with 50-bed capacity, providing integrated TB-HIV care and ART to nearly 15,000 active HIV patients [16]. The study population included HIV-exposed infants with documented final HIV test results in accordance with Ministry of Health guidelines. Infant HIV diagnosis in Uganda is performed using DNA PCR for infants under 18 months and serology for infants aged 18–24 months [2].
Data collection and management
Data collection and participant recruitment were conducted over a three-month period (1st July to 30th September 2024). Data on participants’ socio-demographic characteristics and medical history were extracted from PVT registers, patient cards, and Electronic Medical Records (EMR). Age was categorized into three groups;15–24, 25–34, and >35 years based on biological relevance and previous research [17]. HIV severity was classified according to WHO stages: Stage 1 (asymptomatic), Stage 2 (mild symptoms), Stage 3 (advanced disease), and Stage 4 (severe/AIDS-defining illness). Viral load suppression was defined as HIV RNA ≤ 200 copies/mL, while non-suppression >200 copies/mL, in line with WHO guidelines [2,3]. Drug lines were classified per WHO recommendations: first line ART refers to the initial regimen for starting therapy, second line is used after first line failure, and third line is reserved for patients failing both first and second line regimens [3]. Data entry was performed using Microsoft Excel, with regular accuracy checks against hard copy records to ensure data integrity.
A flowchart illustrates the data collection process as shown in Fig 1 below.
A flowchart.
Statistical analysis plan
Data were analysed using Stata version 17 (StataCorp, College Station, TX, USA). The primary outcome was infant HIV status, defined as a binary variable (positive vs. negative). Maternal and infant characteristics were summarized using frequencies and percentages, with group differences assessed using chi-square or Fisher’s exact tests, as appropriate. Differences between maternal ART regimen and infant HIV status were evaluated using Fisher’s exact test and were restricted to linked mother–infant pairs. Two separate multivariable logistic regression models were fitted: one evaluating maternal factors and a second independently evaluating infant factors. Crude odds ratios (COR) and adjusted odds ratios (aOR), with 95% confidence intervals (CI), were reported with statistical significance defined as p < 0.05. Variables associated with infant HIV positivity at p < 0.20 in bivariate logistic regression, together with biologically plausible factors, were considered for multivariable analysis [18].
Evaluation of model performance was determined using Pseudo R^2^ and discrimination metrics of the area under the receiver operating characteristic curve (AUC). Predictive robustness was assessed using cross-validated AUC. However, due to sparse outcome events which precluded reliable cross-validation in the maternal model, predictive robustness was evaluated using bootstrap internal validation AUC. Formal calibration metrics were not applied due to the very small number of outcome events, which limit their reliability. Given the low level of outcome missingness (1.4%; 14/976), exclusion was unlikely to materially affect study validity or power. Predictor variables with missing data were retained by coding them as “unknown” or “not sure” to minimize potential bias and preserve sample size.
Collinearity among ART-related variables (regimen, duration, and prophylaxis) was assessed using variance inflation factors, with values <5 indicating no problematic multicollinearity.
Sensitivity analyses using Firth’s penalized logistic regression were conducted to address sparse outcome events and yielded directionally consistent estimates with comparable confidence intervals.
A post hoc power analysis was performed using simulation to estimate the study’s ability to detect associations of clinically meaningful magnitude. Assuming an odds ratio of 6, reflecting moderate maternal effects and stronger infant effects, a sample size of 962, and a baseline event rate of 1.96%, 2,000 simulated datasets were generated under a logistic model. Power was estimated as the proportion of simulations yielding p < 0.05 and was 83%, indicating adequate sensitivity to detect effects of this magnitude despite the low outcome prevalence.
Results
Distribution of infant HIV positivity by maternal and infant characteristics
Among the 918 mother-infant pairs, key maternal factors significantly associated with infant HIV positivity included maternal age (p < 0.001), with the highest positivity among women over 35 years (5.8%), and PWLH with a non-suppressed viral load (6.7% vs. 1.6%, p = 0.025). When all the 962 infants were assessed, all infant-related factors were significantly associated with infant HIV positivity. Infants not receiving nevirapine prophylaxis had a markedly higher HIV positivity rate (53.7% vs. 2.3%, p < 0.001). Similarly, those not on cotrimoxazole had a 50% positivity rate compared to 4.1% among those who received it (p < 0.001). Feeding practices also impacted outcomes: exclusive breastfeeding had the lowest HIV positivity (0.4%), while mixed and no breastfeeding had significantly higher rates (9.1% and 25.0%, respectively; p < 0.001) (Table 1).
Table 1: Distribution of infant HIV status by maternal and infant characteristics.
Influence of PVT ART regimen on infant HIV positivity
Among 918 HIV-exposed infants with mother pairs, 18 (1.96%, 95% CI: 1.15–3.06) were confirmed HIV positive. When stratified by maternal ART regimen, HIV positivity was 1.40% (8/571; 95% CI: 0.61–2.74) for infants whose mothers were on DTG-based regimens, 2.96% (8/270; 95% CI: 1.29–5.75) for those on Efavirenz(EFV)-based regimens, 0% (0/43; 95% CI: 0.00–8.22) for Nevirapine(NVP)-based regimens, and 5.88% (2/34; 95% CI: 0.72–19.68) for Protease inhibitor(PI)–based regimens. The difference in HIV positivity rates across these ART regimens was not statistically significant (p = 0.113) as shown in Table 2 below.
Table 2: Proportion of HIV positive infants by PVT ART regimen category.
Bivariate and multivariate analysis of maternal and infant factors associated with VT of HIV
Among maternal factors, being on a PI-based regimen showed higher odds of VT compared with DTG (COR = 4.32; 95% CI: 0.88–21.18; p = 0.071), with a stronger association observed in multivariable analysis (aOR = 22.89; 95% CI: 2.20–238.14; p = 0.009). Maternal age 25–34 years was associated with significantly lower odds of VT compared with mothers aged >35 years (COR = 0.03; 95% CI: 0.00–0.24; p = 0.001) though the association was not sustained after adjustment. Unsuppressed viral load was independently associated with increased VT risk (aOR = 4.97; 95% CI: 1.45–17.10; p = 0.011).
Among infant factors, lack of nevirapine prophylaxis or uncertain receipt was strongly associated with higher odds of VT in bivariate analysis (COR = 49.62; 95% CI: 23.42–105.16; p < 0.001); however, this association was not retained after adjustment (aOR = 1.25; 95% CI: 0.43–3.69; p = 0.682). Similarly, lack of cotrimoxazole prophylaxis was associated with increased VT risk in bivariate analysis (COR = 23.46; 95% CI: 5.66–97.30; p < 0.001), but not in the multivariable model (aOR = 1.02; 95% CI: 0.20–5.22; p = 0.983). In contrast, infant feeding practices remained strongly associated with VT after adjustment. Compared with exclusive breastfeeding, mixed feeding (aOR = 26.87; 95% CI: 5.82–124.10; p < 0.001) and not breastfeeding (aOR = 86.94; 95% CI: 17.40–434.56; p < 0.001) were independently associated with higher odds of VT (Table 3).
Table 3: Bivariate and multivariate analysis of maternal and infant factors associated with VT of HIV.
Comparison of Maternal and Infant Predictors of VT of HIV
The maternal factors model (N = 821) yielded a log-likelihood of −74.54, a pseudo-R² of 0.09, and 10 degrees of freedom, with a standard area under the receiver operating characteristic curve (AUC) of 0.7. Since cross-validated AUC was unreliable due to sparse events, so bootstrap resampling was used for internal validation, yielding moderate discrimination (AUC 0.70, bootstrap 95% CI 0.58–0.83).
In contrast, the infant factors model (N = 962) demonstrated a log-likelihood of −85.95, a pseudo-R² of 0.51, and 7 degrees of freedom, with a standard AUC of 0.94 and a cross-validated AUC of 0.95 (95% CI: 0.79–0.95). AIC and BIC values for each model are reported descriptively as shown in Table 4 below.
Table 4: Model fit statistics for maternal and infant predictors of VT of HIV.
Discussion
This study comprehensively assessed the relative contributions of maternal and infant factors to vertical transmission (VT) of HIV in Uganda. With an overall infant HIV positivity of 1.96% across maternal ART regimens, the findings emphasising the substantial progress achieved through widespread PVT interventions [1–3], while highlighting persistent challenges in the care of HIV-exposed infants. Additionally, no significant difference in HIV positivity was observed across ART regimens (p = 0.113). However, both bivariable and multivariable analyses indicated higher odds of HIV positivity with PI-based regimens, likely reflecting adherence challenges due to higher pill burden and twice-daily dosing. Programmatically, PIs are typically prescribed as second-line therapy, often among individuals with prior treatment failure, which may further confound associations [12,19]. Overall, DTG-, EFV-, and NVP-based regimens appear to provide comparable protection against mother-to-child HIV transmission [20].
Differences in HIV positivity across maternal age groups were significant (p < 0.001). HIV positivity occurred predominantly among mothers aged ≥35 years, while younger age groups showed none or very few events, resulting in perfect prediction in regression analysis. Similarly, a study done in India reported that women aged 30 years and above had a sevenfold increased risk of VT [19]. This finding may reflect HIV program risk stratification, as younger mothers are often perceived as higher risk and thus receive enhanced support within PVT programs, while older mothers may receive relatively less intensive intervention. While previous literature often associates older age with better antiretroviral therapy (ART) outcomes due to presumed greater maturity, awareness, and adherence [17,18], this trend was not observed in our cohort. Furthermore, our study showed that unsuppressed maternal viral load was associated with HIV positivity, consistent with the established link between maternal viremia and infant infection [2,21,22]. This emphasises viral load suppression as a cornerstone of PVT success highlighting the need for routine viral load monitoring among pregnant and breast-feeding women for better exposed HIV infant outcomes [2].
The noted statistical differences in HIV positivity across infant-related factors emphasizes their critical role in prevention of postnatal HIV transmission. However, in the regression analysis, infant feeding practices emerged as a strong factor associated with HIV positivity, with exclusive breastfeeding associated with the lowest HIV positivity. These findings are consistent with biological mechanisms: mixed feeding can damage the infant gut mucosa, facilitating viral entry, while exclusive breastfeeding maintains gut integrity and transmits protective maternal antibodies [23]. The heightened risk in infants not breastfed may relate to lack of immune protection and replacement feeding challenges in resource-limited settings [2,23]. The high odds to HIV positivity among infants with unknown feeding practices may highlight data gaps and possible non-adherence to recommended feeding guidelines.
This study compared maternal and infant logistic regression models to evaluate predictors of infant HIV positivity. The maternal model showed modest explanatory power (pseudo-R² = 0.09) and acceptable discrimination (AUC = 0.74), reflecting limited ability of maternal factors alone to distinguish HIV-positive from HIV-negative infants. Sparse outcome events further prevented reliable cross-validated AUC estimation, highlighting reduced maternal model stability. In contrast, the infant model demonstrated substantially stronger performance (pseudo-R² = 0.51) with excellent discrimination (AUC = 0.94; cross-validated AUC = 0.95, 95% CI 0.79–0.95), indicating robust predictive capacity. These findings suggest that infant-level factors provide greater explanatory and discriminatory value than maternal factors alone, highlighting the dual importance of maternal and infant interventions; as maternal factors reduce intrauterine and intrapartum transmission, while infant care practices drive postnatal HIV positivity. Maintaining maternal viral suppression and promoting safe infant care practices, including exclusive breastfeeding, are therefore essential in PVT programs [2,24].
Implications for policy and practice
Our findings highlight the importance of scaling up all ART regimens in PVT programs, except PI-based regimens, unless DTG-, EFV-, or NVP-based regimens are contraindicated or have documented resistance. Policy should avoid unnecessary regimen switch or transition among pregnant and breast-feeding women unless clinically indicated.
In addition, special attention is warranted for older mothers and those with unsuppressed viral loads, who represent a higher-risk group. Interventions such as targeted adherence counselling, peer to peer psychosocial support, viral load monitoring, and regimen optimization could reduce their transmission risk.
Importantly, during the postpartum period, infant prophylaxis coverage, timely initiation of Nevirapine and cotrimoxazole for all HIV-exposed infants, and exclusive breastfeeding promotion are key actionable areas in PVT programming.
Strengths and limitations
This study’s strengths include a large sample size and clinic-based data collected over six years, offering a comprehensive evaluation of both maternal and infant factors within a real-world clinical context. This enhances the generalizability of the findings. However, some limitations must be acknowledged. The inherent limitations of a retrospective design, including the inability to infer causality and potential bias from incomplete data, may have affected the accuracy of some point estimates. Small numbers in some ART regimen subgroups reduced statistical power, and self-reported infant feeding practices may be subject to recall or social desirability bias. In addition, the low number of outcome events may have increased uncertainty in effect estimates; however, Sensitivity analysis using Firth’s penalised logistic regression evaluated robustness, producing directionally consistent estimates with comparable confidence intervals despite sparse data. Additionally, unmeasured factors such as maternal nutritional status, co-infections, socio-economic conditions, and adherence support interventions could confound the observed associations. Despite these constraints, the study provides important insights into the relative contributions of maternal and infant factors to VT and identifies key areas for strengthening the PVT program.
Conclusion
While maternal factors such as ART regimen and viral load suppression appear important in reducing VT risk, infant factors, particularly prophylaxis and feeding practices, may play a more influential role in shaping infant HIV positivity. These findings emphasize the need for integrated approaches that concurrently optimize maternal treatment and infant care to achieve the goal of eliminating paediatric HIV.
Targeted strategies promoting exclusive breastfeeding, ensuring prophylaxis coverage, and supporting maternal viral suppression, especially among older women, are essential. Strengthening health systems to improve postnatal follow-up will further augment PVT programs. Continued research focusing on disentangling postnatal transmission pathways, including adherence to exclusive breastfeeding, and transitions in feeding practices remain critical in sustaining and accelerating progress toward an HIV-free generation in Uganda and beyond.
Supporting information
S1 FigImpact of negative maternal and infant factors on infant HIV positive outcome.(DOCX)
S2 FigHIV testing algorithm for HIV exposed infants below 18 months.(TIF)
S1 TableShowing time of positive HIV diagnosis among infants.(DOCX)
S2 TableMaternal characteristics for positive infants.(DOCX)
S3 TableSensitivity analysis-penalized regression.(DOCX)
S1 DataFull study dataset.(XLSX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mother-to-child transmission of HIV. [cited 18 May 2025]. Available from: https://www.who.int/teams/global-hiv-hepatitis-and-stis-programmes/hiv/prevention/mother-to-child-transmission-of-hiv
- 2Consolidated guidelines for the prevention and treatment of HIV and AIDS in Uganda. GPC. 2022. [cited 24 Mar 2025]. Available from: https://hivpreventioncoalition.unaids.org/en/resources/consolidated-guidelines-prevention-and-treatment-hiv-and-aids-uganda-november-2022
- 3Consolidated guidelines on HIV prevention, testing, treatment, service delivery and monitoring: recommendations for a public health approach. [cited 10 Jun 2025]. Available from: https://www.who.int/publications/i/item/978924003159334370423 · pubmed ↗
- 4Ellington SR, King CC, Kourtis AP. Host factors that influence mother-to-child transmission of HIV-1: genetics, coinfections, behavior and nutrition. Future Virol. 2011;6(2):1451–69. doi: 10.2217/fvl.11.119 29348780 PMC 5769959 · doi ↗ · pubmed ↗
- 52024 global AIDS report — The Urgency of Now: AIDS at a Crossroads | UNAIDS. [cited 18 May 2025]. Available from: https://www.unaids.org/en/resources/documents/2024/global-aids-update-2024
- 6Kafack EVF, Fokam J, Nana TN, Saniotis A, Halle-Ekane GE. Evaluation of plasma viral-load monitoring and the prevention of mother-to-child transmission of HIV-1 in three health facilities of the Littoral region of Cameroon. P Lo S One. 2022;17(11):e 0277271. doi: 10.1371/journal.pone.0277271 36342923 PMC 9639847 · doi ↗ · pubmed ↗
- 7Fact Sheet: HIV Drug Resistance. [cited 18 May 2025]. Available from: https://www.who.int/news-room/fact-sheets/detail/hiv-drug-resistance
- 8Viral suppression key to preventing mother-to-child transmission, but food insecurity, TB and ST Is may also be risk factors. In: aidsmap.com [Internet]. 2018 [cited 18 May 2025]. Available from: https://www.aidsmap.com/news/nov-2018/viral-suppression-key-preventing-mother-child-transmission-food-insecurity-tb-and