Clinical-Radiological Outcomes of Early Versus Delayed Weight-Bearing Following Proximal Femoral Nail Antirotation 2 Fixation for Intertrochanteric Fractures: A Prospective Randomized Comparative Study
Anup Kumar, Rupendra Jhariya, Sudeep Kumar, Ritesh Pandey, Shikhar Yadav

TL;DR
This study found no significant difference in hip function or radiological outcomes between early and delayed weight-bearing after surgery for hip fractures in elderly patients.
Contribution
The study provides evidence that early weight-bearing after PFNA2 fixation is safe and does not compromise recovery outcomes.
Findings
No significant difference in Modified Harris Hip Scores between early and delayed weight-bearing groups at 24 weeks.
Radiological parameters like tip-apex distance and Parker’s ratio showed no significant differences between the groups.
Early weight-bearing did not increase the risk of complications or affect functional recovery.
Abstract
Background Intertrochanteric fractures commonly occur in elderly patients following minor trauma due to osteoporosis, arthritic hip changes, and balance disorders. Early mobilization is crucial to prevent complications of prolonged bed rest. This study compared Modified Harris Hip Scores (mHHS) between early and delayed weight-bearing protocols following proximal femoral nail antirotation 2 (PFNA2) fixation. Methodology This prospective randomized comparative study was conducted at a tertiary care center, where patients with intertrochanteric fractures treated with PFNA2 were randomly allocated before surgery into the following two groups: Group 1 (early weight-bearing within 24 hours post-surgery) and Group 2 (delayed weight-bearing after four weeks). Outcomes were assessed using mHHS and radiographs over 24 weeks. Results Of the 55 enrolled patients, 46 completed follow-up (21 in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
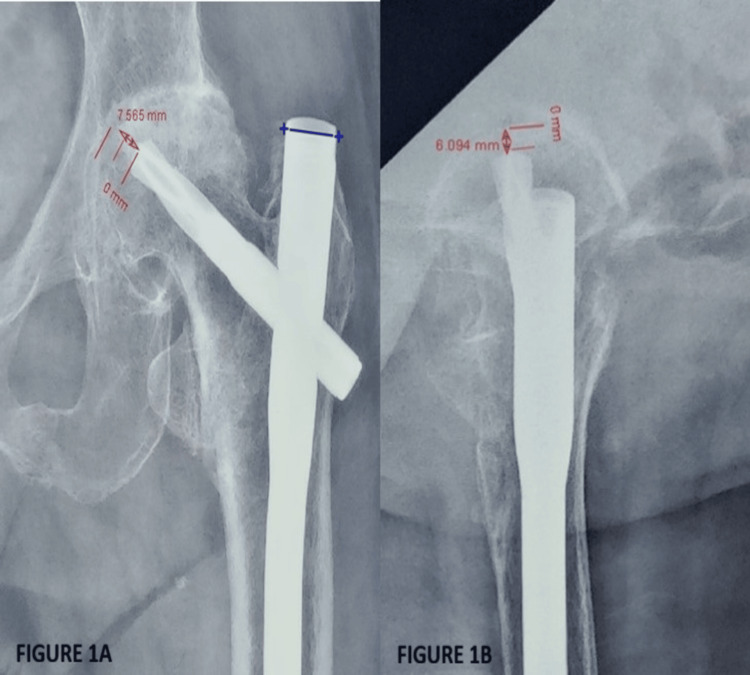 Figure 1
Figure 1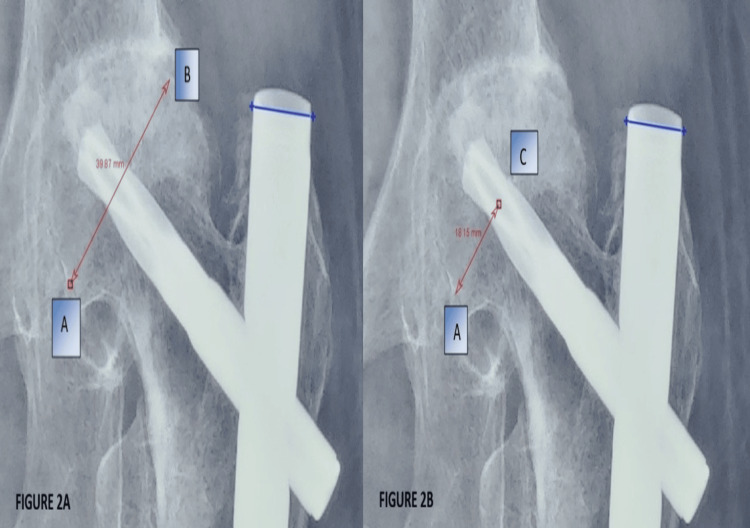 Figure 2
Figure 2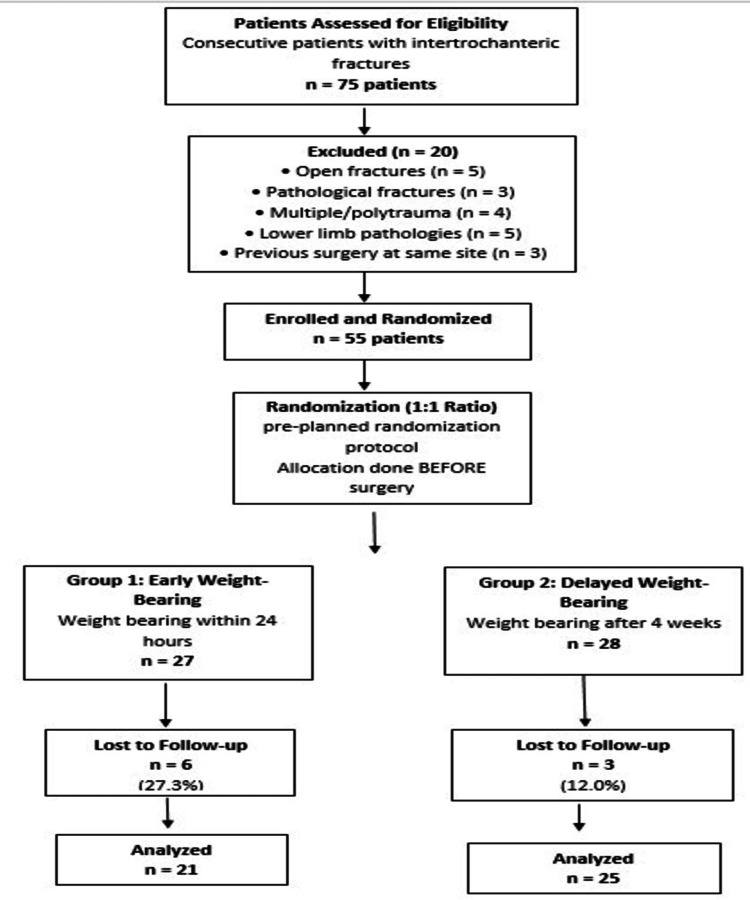 Figure 3
Figure 3| Characteristics | Late weight-bearing (n = 25) | Early weight-bearing (n = 21) | P-value |
| Age (years) | 65.80 ± 12.95 | 69.10 ± 11.67 | 0.374 |
| Gender | |||
| Male | 13 (52.0%) | 11 (52.4%) | - |
| Female | 12 (48.0%) | 10 (47.6%) | |
| Fracture side | |||
| Right | 16 (64.0%) | 14 (66.7%) | - |
| Left | 9 (36.0%) | 7 (33.3%) | |
| Fracture classification | |||
| AO 31A1 | 15 (60.0%) | 14 (66.7%) | - |
| AO 31A2 | 7 (28.0%) | 5 (23.8%) | |
| AO 31A3 | 3 (12.0%) | 2 (9.5%) | |
| Hospital stay (days) | 9.1 ± 2.8 | 8.2 ± 2.1 | 0.156 |
| mHHS | Late weight-bearing | Early weight-bearing | Unpaired t-test | |||
| Mean | SD | Mean | SD | t-value | P-value | |
| Baseline | 93.16 | 10.10 | 96.00 | 5.18 | 1.17 | 0.250 |
| 4th week | 47.48 | 9.85 | 51.67 | 9.70 | 1.45 | 0.155 |
| 8th week | 56.28 | 10.68 | 59.67 | 12.52 | 0.99 | 0.328 |
| 12th week | 70.80 | 10.54 | 73.90 | 13.64 | 0.87 | 0.389 |
| 24th week | 82.28 | 12.29 | 84.95 | 15.82 | 0.64 | 0.523 |
| Intragroup (repeated measures ANOVA) | F = 168.45, p < 0.001 | F = 102.92, p < 0.001 | ||||
| TAD (in mm) | Late weight-bearing | Early weight-bearing | Unpaired t-test | |||
| Mean | SD | Mean | SD | t-value | P-value | |
| 4th week | 18.07 | 4.03 | 19.54 | 6.24 | 0.97 | 0.339 |
| 8th week | 17.78 | 3.76 | 19.71 | 4.56 | 1.58 | 0.121 |
| 12th week | 17.92 | 3.67 | 20.23 | 5.49 | 1.70 | 0.097 |
| 24th week | 18.13 | 4.04 | 22.11 | 9.68 | 1.87 | 0.068 |
| Intragroup (repeated measures ANOVA) | F = 1.64, p = 0.188 | F = 1.39, p = 0.254 | ||||
| Parker’s ratio | Late weight-bearing | Early weight-bearing | Unpaired t-test | |||
| Mean | SD | Mean | SD | t-value | P-value | |
| 4th week | 0.54 | 0.08 | 0.53 | 0.08 | -0.40 | 0.693 |
| 8th week | 0.54 | 0.09 | 0.55 | 0.07 | 0.45 | 0.656 |
| 12th week | 0.54 | 0.08 | 0.55 | 0.07 | 0.37 | 0.714 |
| 24th week | 0.56 | 0.10 | 0.56 | 0.10 | 0.13 | 0.900 |
| Intragroup (repeated measures ANOVA) | F = 2.74, p = 0.050 | F = 1.60, p = 0.200 | ||||
| mHHS | Number of patients | Percentage (%) |
| Excellent | 20 | 43.4 |
| Good | 12 | 26.08 |
| Fair | 8 | 17.39 |
| Poor | 6 | 13.04 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHip and Femur Fractures · Bone fractures and treatments · Bone health and osteoporosis research
Introduction
Intertrochanteric fractures are encountered in both young and elderly populations, but occur more commonly in older age groups. According to the International Osteoporosis Foundation, six million such fractures could occur globally by 2050, up from the current estimate of 1.6 million each year [1]. A 2019 study by Ayoade et al. [2] reported that primary diagnoses of intertrochanteric fractures and all hip fractures had incidence rates per 100,000 of 171 and 402, respectively. Treatment of these fractures is almost always an operative intervention with an extramedullary or intramedullary implant. Postoperatively, patients can be mobilized either with delayed or immediate weight-bearing with support.
Delaying weight-bearing reduces mechanical failure but increases complications related to patient immobilization, such as deep venous thrombosis and pressure sores. Moreover, restricted weight-bearing has been associated with low revision rates (2.9%) after primary fixation of intertrochanteric fractures [3]. Early mobilization counters complications that can occur due to decumbency at old age, but poses the risk of mechanical failure due to implant cut-out secondary to osteoporosis and/or excessive mobilization in this age group. In addition to having a major effect on short-term outcomes such as fewer complications and shorter hospital stays, early mobilization recovery also improves long-term outcomes such as increased autonomy and decreased mortality [4-7]. The goal of surgery is mainly stable fixation, allowing mobilization with early full weight-bearing and rapid return to pre-fracture activity level.
The present study was conducted to determine whether there was any difference in functional recovery as measured by the Modified Harris Hip Score (mHHS) of patients undergoing early weight-bearing compared to late weight-bearing postoperatively in patients undergoing fixation with proximal femoral nail antirotation 2 (PFNA2) for intertrochanteric fractures.
Materials and methods
Study design and setting
In this prospective study, we analyzed 55 consecutive patients who had intertrochanteric fractures and underwent fixation with PFNA2. This study was conducted in the Department of Orthopedics at a tertiary care center over a defined study period. This was a prospective comparative study utilizing a randomized cohort allocation with two different postoperative weight-bearing protocols.
Ethical approval
Before the commencement of the study, ethical approval was obtained from the Institutional Ethics Committee, All India Institute of Medical Sciences, Patna (approval number: AIIMS/Pat/IEC/PGTh/Jan21/18). Consecutive patients meeting the inclusion criteria were enrolled in the study after providing informed consent.
Inclusion and exclusion criteria
Patients with intertrochanteric fractures type AO31A1, 31A2, and 31A3; those with closed intertrochanteric fractures; those aged 18 years and above; and those who provided consent to participate in the study were considered for inclusion in the study. Patients with open fractures, pathological fractures, multiple fractures, and polytrauma; those with pathologies of the knee or lower limb; those with intraoperative fractures and undergoing additional intervention; and those with previous surgery on the same site were excluded from the study.
Group allocation and randomization
The study population was divided into the following two groups: Group 1 (early weight-bearing) included patients who were randomly allocated to undergo weight-bearing as able mobilization after 24 hours following fixation of the intertrochanteric fracture with a PFNA2 using a walker or axillary crutches. Group 2 (delayed weight-bearing) included patients who were randomly allocated to undergo weight-bearing mobilization only after four weeks following fixation of the intertrochanteric fracture with a PFNA2 using a walker or axillary crutches.
Patients meeting the inclusion criteria were randomized in a 1:1 ratio to Group 1 or Group 2 using a pre-planned randomization protocol before surgical intervention. The randomization sequence was generated before patient enrollment.
Study procedure
Patients were subjected to routine clinical examination and radiological investigations. Preoperatively, mHHS was calculated by the evaluator to assess the pre-fracture status. Patients were randomly allocated to Group 1 or Group 2 before surgery using the pre-planned randomization protocol. Mobilization of patients was done with walker support as soon as possible, and weight-bearing was allowed according to their randomized study group. The duration of hospital stay postoperatively was recorded.
Postoperative protocol
Patients in the early weight-bearing group were made to bear weight as able and mobilized using walkers within 24 hours of surgery. Patients in the late weight-bearing group were made to sit by the side of the bed or made to walk without bearing weight on the operated limb using walker support. All patients in both groups received the same deep vein thrombosis prophylaxis (enoxaparin 40 mg subcutaneously once daily starting 12 hours postoperatively to 48 hours postoperatively, followed by aspirin 75 mg orally once daily for three weeks).
Outcome assessment
A comprehensive examination of the hip was performed, and inspection and palpatory findings were documented. To determine functional status using mHHS, patients were provided with scoring sheets, and assistance was provided in filling them as required. Radiological assessment was performed using the tracker app. The tip-apex distance (TAD) and Parker’s ratio were calculated for all radiographs, as shown in Figure 1 and Figure 2. During the measurement, the diameter of the helical blade and the proximal portion of the nail, which were 10.6 mm and 16.5 mm, respectively, were taken as the reference scale. The TAD was calculated from the center of the tip of the helical blade to the center of the femur head in both anteroposterior and lateral views of the radiograph, and then both were summed. Radiographs were also checked for signs of union and complications such as helical blade cutout and implant breakage. Each patient was assessed preoperatively and at 4, 8, 12, and 24 weeks postoperatively.
Tip-apex distance calculation on anteroposterior and lateral radiographs.(A) Anteroposterior view. (B) Lateral view.The tip-apex distance is calculated as the sum of measurements in anteroposterior and lateral radiographs. Blue line = reference measurement (proximal nail diameter = 16.5 mm).
Parker’s ratio calculation demonstrating proper blade positioning.(A) Measurement of the femoral head diameter (Line AB) perpendicular to the femur-neck axis. (B) Perpendicular line to the head-neck axis intersecting at the helical blade mid-point (Line AC).Parker’s ratio = Line AC/Line AB. Blue line = reference measurement.
Statistical analysis
Significance of the association between two categorical variables was assessed using the chi-square test, and the significance of the mean difference was ascertained using Student’s t-test. Repeated measures analysis of variance (ANOVA) was applied to determine the change in the mean score within and between study groups over time. A two-sided p-value of less than 0.05 was deemed statistically significant. SPSS version 23 (IBM Corp., Armonk, NY, USA) was used for data analysis.
Results
Study participants and baseline characteristics
In this prospective randomized comparative study, patients were randomly allocated into early versus delayed weight-bearing groups before surgical intervention. A total of 55 consecutive eligible patients were randomized to the two groups, though nine patients (six from the early weight-bearing group and three from the late weight-bearing group) were lost to follow-up (Figure 3), leaving 46 patients for the final analysis (21 in the early weight-bearing group, 25 in the late weight-bearing group). The baseline demographic and clinical characteristics of both groups were comparable, with no significant differences in age, gender, fracture side, or fracture classification, indicating successful randomization (Table 1).
Flow diagram showing patient enrollment, randomization, allocation, follow-up, and analysis.EWB: early weight-bearing; LWB: late/delayed weight-bearing; PFNA2: proximal femoral nail antirotation 2
Primary outcome: Modified Harris Hip Score
No statistically significant differences were observed in mHHS between the early and delayed weight-bearing groups at any time point throughout the 24-week follow-up period. Both groups demonstrated significant within-group improvement over time (late weight-bearing: F = 168.45, p < 0.001; early weight-bearing: F = 102.92, p < 0.001 on repeated measures ANOVA). Detailed mHHS at each timepoint are presented in Table 2.
Secondary outcomes: radiological parameters
TAD and Parker's ratio remained comparable between both groups throughout the follow-up period with no significant between-group differences. Detailed radiological measurements at each timepoint are presented in Table 3 and Table 4. No significant differences were observed in postoperative complications, including surgical site infections, deep vein thrombosis, pressure sores, or implant failures, between the two groups during the 24-week follow-up period.
Functional outcome at 24 weeks
At the end of 24 weeks, functional assessment demonstrated excellent or good outcomes in 69.5% of patients (20 with excellent outcomes, 12 with good outcomes). Fair outcomes were observed in 17.39% (n = 8), while poor outcomes occurred in 13.04% (n = 6) of participants (Table 5).
Subgroup analyses
Subgroup analyses stratified by age groups (≤65 years vs. >65 years), fracture type (31A1 vs. 31A2/A3), and gender demonstrated consistent findings with no significant between-group differences in mHHS outcomes, suggesting that early weight-bearing is safe and effective across diverse patient populations.
Discussion
Main findings
Hip fractures can change the course of an orthogeriatric patient’s life. Reduction of mobility in hip fracture patients poses a significant threat to their clinical outcome, quality of life, and survival, particularly in the elderly population. Early mobilization without weight-bearing restrictions has been shown to benefit these patients. Conversely, prolonged bed rest and difficulty in mobilization can lead to various complications, including urinary tract infections, respiratory pneumonia, deep vein thrombosis, and pressure sores. Even brief periods of muscle disuse can result in substantial losses in muscle mass and function [8].
The results of this prospective randomized comparative study demonstrate that early weight-bearing does not adversely impact functional outcomes compared to delayed weight-bearing protocols. Both groups showed significant within-group improvement in mHHS over the 24-week follow-up period, with no statistically significant between-group differences. Radiological parameters (TAD and Parker’s ratio) also remained comparable between groups, indicating that implant positioning and stability were not compromised by early mobilization. Additionally, subgroup analyses stratified by age, fracture type, and gender consistently demonstrated comparable outcomes between protocols, suggesting that early weight-bearing is safe and effective across diverse patient populations.
Comparison with existing literature
These findings suggest that early weight-bearing may be a viable option for patients undergoing fixation of intertrochanteric fractures with PFNA2, without compromising functional outcomes. Our results align with Siu et al. [9], who reported that mobilization in the early postoperative phase is of superior importance, as delays are associated with diminished physical function at two months and worse survival rates at six months. Our findings are further supported by Kuru et al. [10], who reported that early weight-bearing within 24 hours postoperatively results in significantly better Harris and pain scores compared to delayed weight-bearing. Similarly, Ottesen et al. [11] found that elderly hip fracture patients with weight-bearing restrictions had higher rates of adverse events, including delirium, infection, and mortality, compared to those allowed to weight-bear as tolerated.
Further, our results are consistent with a retrospective analysis by Takemoto et al. [12] of 293 patients, who found that weight-bearing restriction did not decrease the incidence of surgical failures; moreover, the non-weight-bearing group had significantly more surgical complications than the weight-bearing group. A comparable study by Vishwanathan et al. [13] included 81 patients treated with proximal femoral nail, with 75 patients completing follow-up, and revealed that the mHHS significantly improved at one, three, and six months postoperatively. Another study by Jia et al. [14] conducted among 806 matched patients revealed no significant difference in implant failure at 12 months between immediate and restricted weight-bearing groups; however, patients with immediate weight-bearing had a significantly shorter time to full weight-bearing (87.6 vs. 121.3 days).
A study by Pfeufer et al. [15] reported that elderly hip fracture patients with postoperative weight-bearing restrictions had significantly reduced mobility and gait speed compared to those with full weight-bearing (Parker Mobility Score: 3.21 vs. 4.73, p < 0.001; gait speed: 0.16 m/s vs. 0.28 m/s, p = 0.003). Another similar study by Oldmeadow et al. [4] found that at one-week post-surgery, patients in the early ambulation group walked further than those in the delayed ambulation group (p = 0.03) and required less assistance to transfer (p = 0.009). Compared to the delayed ambulation group, patients in the early ambulation group were less likely to require high-level care (36.8% vs. 56%) and more likely to be sent home straight from acute care (26.3% vs. 2.4%).
A study by Li et al. [16] investigated the effects of varying loads on the PFNA2 implant, specifically examining displacement and loading cycles under different weight-bearing conditions post-implantation. Their findings indicated that in elderly patients with unstable intertrochanteric femoral fractures, the nail offers the primary postoperative structural support and stability; however, weight-bearing should be restricted to 900 N to reduce the risk of implant failure and complications. Therefore, early initiation of graduated weight-bearing is permissible, as long as it remains within the mechanical strength of the implant.
Generalizability and clinical implications
This study was conducted in a single tertiary care center in India and involved predominantly elderly patients with stable intertrochanteric fractures treated with PFNA2 implants. The findings may have limited generalizability to other healthcare settings with different resources, surgical expertise, postoperative rehabilitation protocols, or patient populations with different baseline characteristics and comorbidity profiles. Furthermore, the study population was relatively homogeneous in terms of implant type (PFNA2), and results may not directly apply to other fixation methods, such as the dynamic hip screw or intramedullary nailing. Future multicenter prospective randomized controlled trials are needed to validate these findings across diverse populations and healthcare settings.
Study limitations
This study had several important limitations that warrant consideration. First, although patients were randomly allocated to weight-bearing groups before surgery, this prospective randomized comparative study was designed and reported as an observational comparative study rather than with full randomized controlled trial (RCT) methodology (such as concealment of allocation sequence, blinding of participants/assessors, or pre-registered protocol). This methodological design choice may affect the interpretation of causality compared to a fully reported RCT. However, the randomized allocation before surgery does reduce selection bias from postoperative decision-making based on operative findings.
Second, the surgeries were performed by different surgeons, which may have introduced variations in reduction quality, fixation technique, and implant positioning, potentially affecting radiological parameters (TAD and Parker’s ratio) and functional outcomes. These differences could have masked or exaggerated the true effects of weight-bearing protocols.
Third, our follow-up period was relatively short (24 weeks), precluding assessment of the complete time required for individuals to recover and return to their pre-injury functional status. Long-term outcomes beyond six months, including late implant failures and return to community ambulation, were not evaluated.
Fourth, the study was conducted at a single tertiary care center with a specific patient population, which may limit the generalizability of findings to other healthcare settings, patient demographics, or geographic regions with different resource availability and patient characteristics.
Fifth, loss to follow-up occurred in 16.4% of enrolled patients (9 of 55), with slightly higher attrition in the early weight-bearing group (27.3% vs. 12%). This differential loss could introduce bias if the reasons for dropout were related to weight-bearing status or clinical outcomes.
Sixth, this study was not powered for subgroup analysis by AO classification. Future larger studies should examine whether fracture severity influences weight-bearing protocol outcomes.
Finally, while randomization was performed, potential unmeasured confounding variables such as bone quality assessment, specific comorbid medical conditions, smoking status, medication use (particularly anticoagulants or bisphosphonates), and variations in surgeon experience could have influenced outcomes independent of the weight-bearing protocol itself.
Conclusions
This prospective randomized comparative study supports early weight-bearing as a safe and effective option for patients with intertrochanteric fractures treated with PFNA2. No significant differences were observed in complication rates, functional recovery, or radiological outcomes between early and delayed weight-bearing groups. These findings align with existing literature, further reinforcing that early mobilization does not compromise fracture healing or fixation stability. Early weight-bearing within 24 hours post-surgery appears to be a viable and safe option that may facilitate faster patient mobilization and potentially reduce complications associated with prolonged immobilization, without compromising functional or radiological outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Implant options for the treatment of intertrochanteric fractures of the hip: rationale, evidence, and recommendations Bone Joint J Socci AR Casemyr NE Leslie MP Baumgaertner MR 12813399-B 20172805326810.1302/0301-620X.99B 1.BJJ-2016-0134.R 1 · doi ↗ · pubmed ↗
- 2Incidence and economic burden of intertrochanteric fracture: a Medicare claims database analysis JB JS Open Access Adeyemi A Delhougne G 04201910.2106/JBJS.OA.18.00045 PMC 651046931161153 · doi ↗ · pubmed ↗
- 3Dependency after hip fracture in geriatric patients: a study of predictive factors J Orthop Trauma Koval KJ Skovron ML Polatsch D Aharonoff GB Zuckerman JD 531535101996891591410.1097/00005131-199611000-00004 · doi ↗ · pubmed ↗
- 4No rest for the wounded: early ambulation after hip surgery accelerates recovery ANZ J Surg Oldmeadow LB Edwards ER Kimmel LA Kipen E Robertson VJ Bailey MJ 6076117620061681362710.1111/j.1445-2197.2006.03786.x · doi ↗ · pubmed ↗
- 5Institutional prescreening for detection and eradication of methicillin-resistant Staphylococcus aureus in patients undergoing elective orthopaedic surgery J Bone Joint Surg Am Kim DH Spencer M Davidson SM 182018269220102061077310.2106/JBJS.I.01050 · doi ↗ · pubmed ↗
- 6Which factors are independent predictors of early recovery of mobility in the older adults' population after hip fracture? A cohort prognostic study Arch Orthop Trauma Surg Morri M Forni C Marchioni M Bonetti E Marseglia F Cotti A 354113820182895615210.1007/s 00402-017-2803-y · doi ↗ · pubmed ↗
- 7The basic mobility status upon acute hospital discharge is an independent risk factor for mortality up to 5 years after hip fracture surgery Acta Orthop Kristensen MT Kehlet H 47528920182894678110.1080/17453674.2017.1382038 PMC 5810832 · doi ↗ · pubmed ↗
- 8Protecting muscle mass and function in older adults during bed rest Curr Opin Clin Nutr Metab Care English KL Paddon-Jones D 34391320101989823210.1097/MCO.0b 013e 328333 aa 66PMC 3276215 · doi ↗ · pubmed ↗