Minimally invasive orthodontic management: a paradigm shift in interceptive care. Part I - concept and palatally displaced canines
Daniela GARIB, Ana Cláudia de Castro Ferreira CONTI, Felicia MIRANDA, Camila MASSARO, Susan SASSAKI, Silvio Augusto BELLINI-PEREIRA, Cibele ALBERGARIA

TL;DR
This paper introduces a new approach to early orthodontic care that uses minimal intervention to improve outcomes and reduce future treatment needs.
Contribution
The paper introduces Minimally Invasive Orthodontic Management (MIO) as a new paradigm for interceptive orthodontic care in children.
Findings
Early diagnosis of palatally displaced canines between ages 10 and 12 improves treatment outcomes.
Interceptive strategies like deciduous canine extraction have a success rate of about 70%.
MIO reduces the need for complex adolescent orthodontic treatments and improves cost-effectiveness.
Abstract
Conservative approaches in childhood may enhance esthetics and function while reducing the likelihood of complex Phase II orthodontic treatments during adolescence. This article aims to introduce the principles of Minimally Invasive Orthodontic Management (MIO) during the mixed dentition period, promoting the concept of “as little intervention as possible”, in accordance to The “Orange July” campaign. The core principles of MIO include: (1) early diagnosis and risk assessment; (2) evidence-based, timely, and targeted interventions; and (3) prioritization of patient comfort and psychosocial well-being. Part I addresses the application of MIO to the interceptive management of palatally displaced canines (PDC). Early diagnosis, typically between ages 10 and 12, is based on clinical indicators and radiographic assessment. Major risk factors for PDC include female sex, hypodivergent facial…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1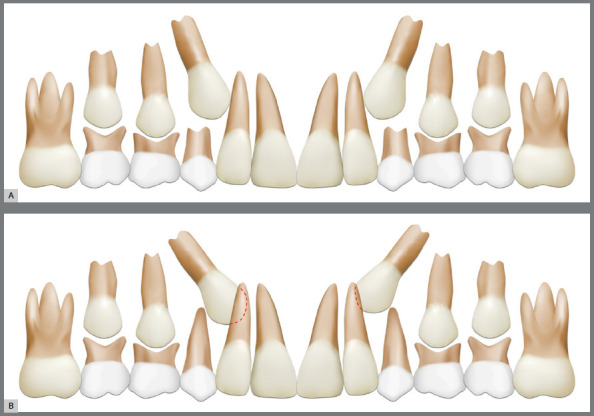 Figure 2
Figure 2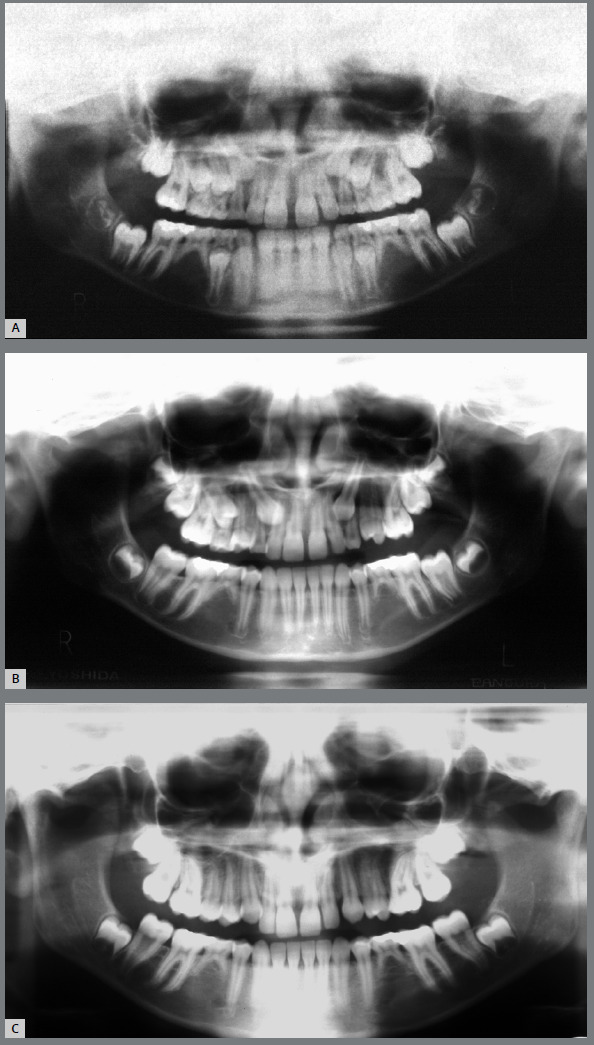 Figure 3
Figure 3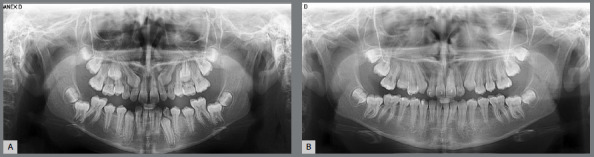 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthodontics and Dentofacial Orthopedics · dental development and anomalies · Dental Trauma and Treatments
INTRODUCTION
The term “conservative” is not new in Dentistry. The concept of minimally invasive dentistry emerged during the transition from the 20th to the 21st century, emphasizing the preservation of healthy tooth structure, risk assessment, early diagnosis, and conservative treatment approaches. The principle of “as little intervention as possible” was advocated by Peters and McLean from the University of Michigan in 2001.1 This concept has found significant application in operative dentistry, particularly in the principle of “prevention of extension.”2 However, the principles of minimally invasive dentistry are equally applicable to orthodontics, particularly within the context of interceptive treatment. Minimally Invasive Orthodontic Management (MIO) advocates for the use of simple yet effective procedures during the mixed dentition period to guide normal dental and skeletal development, prevent the progression of more severe malocclusions, and reduce the need for extensive orthodontic or surgical interventions in the permanent dentition. The ultimate goal of minimally invasive orthodontic care is to simplify or even eliminate the need for Phase II orthodontic treatment.
MIO aligns with the perspective that less is more-and often better. Its core principles include: 1. Early diagnosis and risk assessment: By using clinical indicators and conservative imaging techniques, clinicians can identify deviations from normal eruption patterns or growth discrepancies at an early stage. In some cases, diagnosis is dynamic and requires longitudinal follow-up to monitor dental development and facial growth patterns. 2. Evidence-based, timely, and targeted interventions: Interventions should be undertaken only when supported by evidence demonstrating long-term benefits. A cost-effectiveness analysis should be conducted for each individual case within a patient-centered care framework. The timing of these interventions is crucial to minimize invasiveness while maximizing therapeutic efficacy. Conservative approaches should adhere to interdisciplinary collaboration and evidence-based practice principles; and 3. Patient comfort and psychosocial well-being: Minimally invasive orthodontic care prioritizes the child’s comfort and emotional development.
Conservative interventions during the mixed dentition can enhance esthetics and function earlier, potentially preventing the need for more complex Phase II orthodontic treatments during adolescence. Minimally invasive strategies implemented during the mixed dentition period can simplify orthodontic management in the permanent dentition. As orthodontics advances toward precision and individualized care, the minimally invasive approach serves as a unifying concept that encourages clinicians to balance treatment efficacy with the preservation of biological structures. It promotes thoughtful and timely intervention-favoring less but more effective treatment. Clinicians should recognize the value of a shorter and simpler pathway to achieving the best possible occlusion.
“Orange July” is a national awareness campaign launched in Brazil to promote early orthodontic assessment, based on the principles of minimally invasive orthodontic management (Fig. 1). The campaign advocates for the first orthodontic evaluation to take place between 5 and 7 years of age, coinciding with the early mixed dentition phase, rather than following the traditional approach of waiting until approximately 12 years of age during the permanent dentition stage. This shift changes the recommendation for the timing of the first orthodontic appointment: on exfoliation of the first deciduous tooth, rather than after exfoliation of the last tooth. By promoting earlier referrals, the Orange July campaign aims to facilitate timely diagnosis, risk assessment, and conservative interceptive interventions, thereby potentially reducing the need for complex and more invasive treatments during adolescence. The campaign targets both general dental professionals and parents/caregivers, emphasizing that early identification of developing malocclusions enables more simple, biologically compatible, and patient-centered care. This initiative reflects a broader trend in orthodontics toward preventive and minimally invasive strategies that emphasize treatment simplification and long-term stability. Prevention represents the highest expression of well-being that individuals can experience in healthcare.
Figure 1:The Orange July campaign advocates for early orthodontic evaluation, emphasizing principles of minimally invasive orthodontic management to support timely, preventive, and patient-centered care.
The cost-effectiveness of early treatment includes esthetic and functional improvements, enhanced quality of life, preservation of dental and periodontal tissues, long-term stability, and the simplification of Phase II treatment through reductions in duration, complexity, and invasiveness. Evidence demonstrates a clear cost-effectiveness ratio for the interceptive treatment of three dentofacial irregularities: (1) palatally displaced canines; (2) malocclusions primarily caused by oral habits, including posterior crossbites and dentoalveolar open bites; and (3) Class III malocclusions. This Part I article addresses palatally displaced canines, while malocclusions related to oral habits and the Class III facial pattern are the focus of Parts II and III, respectively.
PALATALLY DISPLACED CANINES (PDC)
EARLY DIAGNOSIS
The optimal window for early diagnosis of palatally displaced canines is during the late mixed dentition period, between 10 and 12 years of age.³ In most cases, the canine bud develops in its normal position distal to the maxillary lateral incisors, at the level of the nasal floor.⁴ In this context, the position of the canine during the early and intermediate mixed dentition may mislead even the most attentive clinicians. The disturbance becomes apparent only when the canines begin to erupt. Rather than following a direct path to the dental arch, the ectopic eruption causes the canine to deviate palatally and mesially. In rare cases, the maxillary canine tooth germ is malpositioned even before eruption begins.
Early diagnosis begins with clinical evaluation. During the late mixed dentition, clinical indicators of palatally displaced canines (PDC) include asymmetry or severe tipping of the maxillary lateral incisors, as well as the absence of palpable maxillary canine buds on the buccal aspect of the alveolar ridge.5 In these cases, a panoramic radiograph should be requested to assess the position of the canine buds relative to the roots of the adjacent lateral incisors. When the contour of the maxillary canine cusp overlaps the root contours of the lateral incisor, the canine is considered ectopic (Fig. 2). Clark periapical radiographs can confirm the palatal position of maxillary canines relative to the roots of the lateral incisors. Unilateral occurrence of palatally displaced canines (PDC) is more common than bilateral involvement.6
Figure 2:A) Physiologic position of the maxillary canines during the late mixed dentition observed in a panoramic radiograph, illustrating the “ugly duckling” phase; B) Ectopic eruption of the maxillary canines toward the palate, with superimposition of the canine bud image over the lateral incisor root bilaterally.
Two major consequences of palatally displaced canines (PDC) may arise. Ectopic eruption can result in canine impaction, requering complex and invasive procedures in the permanent dentition, such as tooth traction. Additionally, tooth traction can prolong the duration of Phase II orthodontic treatment.7 Root resorption of maxillary incisors is another consequence associated with PDC.8 In accordance with the principles of minimally invasive orthodontics, interceptive management is recommended upon diagnosis of PDC to simplify comprehensive orthodontic treatment and preserve dental tissues.
RISK ASSESSMENT
PCD probably has a genetic background. Besides previous citation of familiar history and occurrence in homozygotic twins,9 ^,^ 10 PDC is more likely to occur in patients with other dental anomalies with a genetic origin.10 ^-^ 12 To enable preventive management of PDC during the mixed dentition, risk assessments should be conducted early in this developmental phase. Critical risk factors for palatally displaced canines are:
Female gender: Females are two to three times more likely to be affected than males. Consequently, female gender is associated with a higher risk of developing ectopic eruption of maxillary canines compared to males.11 ^,^ 13
Hypodivergent facial pattern: The majority of PDC cases occur in patients with a hypodivergent facial growth pattern.6 Although PDC can also be observed in normodivergent and hyperdivergent patterns, most patients with PDC in our experience are hypodivergent. It is hypothesized that hypodivergent patients possess a greater anteroposterior dimension of the maxilla, providing increased space. Consequently, the maxillary canine can more easily deviate from the labial to the palatal side of the alveolar ridge, encountering less interference from the roots of adjacent teeth.
Positive tooth-arch size discrepancies: Dental arches with spacing exhibit a higher risk for PDC compared to crowded arches.¹⁴ This may be explained by the increased space availability in the dental arch, which facilitates ectopic eruption.
Presence of other dental anomalies: PDC is part of a dental anomaly pattern.10 ^-^ 12 A shared genetic background may affect multiple teeth with variable expression, resulting in associated dental anomalies. Tooth agenesis, small maxillary lateral incisors, infraocclusion of deciduous molars, and other ectopic tooth eruptions serve as red flags indicating the potential development of PDC in the late mixed dentition.10 ^-^ 12 When these anomalies are identified during the early mixed dentition, close monitoring of canine eruption between 10 and 12 years of age is essential (Fig. 3).
Figure 3:Development of PDC in a patient with agenesis of second premolars. **A)**At the intertransitional period of the mixed dentition, at 9.75 years of age, both maxillary canines were in a normal position. B) At the second transitional period of the mixed dentition, at 11.33 years, both maxillary canine were ectopic. The extraction of 53 and 63 was accomplished. **C)**The maxillary permanent canines successfully erupted in the dental arch.
MINIMALLY INVASIVE MANAGEMENT STRATEGIES
Minimally invasive management of palatally displaced canines (PDCs) during the mixed dentition period emphasizes interceptive treatment aimed at stimulating proper eruption and preventing the need for more complex surgical or orthodontic interventions later. When PDC is diagnosed during the late mixed dentition, extraction of the predecessor deciduous canine can promote normalization of the canine’s eruption path (Fig. 4).3 ^,^ 15 The success rate of deciduous canine extraction is approximately 70%.3 Prognosis is influenced by patient age and the position of the canine.16 Canines that are more mesially displaced have a poorer prognosis compared to those that are only slightly mesially displaced.16 In a minimally invasive approach, extraction of deciduous maxillary first molars alongside deciduous canines is not recommended, as the success rate of double extraction is comparable to that of deciduous canine extraction alone.17
Figure 4:Bilateral case of palatally displaced canine successfully treated with deciduous canine extraction. A) At 12 years of age in the second transitional period of the mixed dentition, the superimposition of maxillary canine bud with the root of the lateral incisors revealed the ectopic eruption of maxillary canines. Clark periapical radiographs confirmed the PDC; B) One year after the extraction of maxillary deciduous canines at 13 years of age. The maxillary permanent canines successfully erupted, preventing impaction (credit: Dr. Cristiane Nakano).
Following deciduous canine extraction, normalization of the permanent canine eruption should be monitored with a panoramic radiograph taken 10 to 12 months post-extraction.3 After deciduous canine extraction, the mean time for permanent canine eruption is approximately 15 months, with a variation of ±6 months.15 Unilateral deciduous canine extraction does not cause deviation of the maxillary midline.18 Concerns regarding tooth space loss are minimal.18 However, a fixed or removable space maintainer with a temporary prosthetic tooth may be used to enhance psychosocial comfort.
Another procedure that influences the eruption of palatally displaced canines during the late mixed dentition is rapid maxillary expansion (RME). RME alone has demonstrated a success rate of 66%, which increases to 80% when combined with deciduous canine extraction.16 ^,^ 19 In Class II patients with PDC, the use of a cervical headgear appliance has also been shown to increase the success rate of permanent canine eruption.20
CONCLUSIONS
The first orthodontic examination should be conducted no later than the early mixed dentition stage. When interceptive treatment is indicated, the principles of minimally invasive orthodontic care should be applied.
Interceptive management of palatally displaced canines is essential to prevent root resorption of permanent maxillary incisors and to simplify comprehensive orthodontic treatment-thereby reducing patient and family stress, treatment costs, invasiveness, and treatment duration.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Peters MC Mc Lean ME Minimally invasive operative care. I. Minimal intervention and concepts for minimally invasive cavity preparations J Adhes Dent 20013171611317386 · pubmed ↗
- 2Mc Intyre J Minimal intervention dentistry Ann R Australas Coll Dent Surg 19941272797993063 · pubmed ↗
- 3Ericson S Kurol J Early treatment of palatally erupting maxillary canines by extraction of the primary canines Eur J Orthod 1988104283295320884310.1093/ejo/10.4.283 · doi ↗ · pubmed ↗
- 4van der Linden FPGM Duterloo HS Development of the human dentition 19761 Chicago Quintessence Publishing
- 5Ericson S Kurol J Radiographic assessment of maxillary canine eruption in children with clinical signs of eruption disturbance Eur J Orthod 198683133140346443610.1093/ejo/8.3.133 · doi ↗ · pubmed ↗
- 6Sacerdoti R Baccetti T Dentoskeletal features associated with unilateral or bilateral palatal displacement of maxillary canines Am J Orthod Dentofacial Orthop 200412667257321567313210.1043/0003-3219(2004)074<0725:DFAWUO>2.0.CO;2 · doi ↗ · pubmed ↗
- 7Kokich VG Jr Mathews DP Surgical and orthodontic management of impacted teeth Dent Clin North Am 19933721812048477864 · pubmed ↗
- 8Ericson S Kurol PJ Resorption of incisors after ectopic eruption of maxillary canines a CT study Angle Orthod 20007064154231113864410.1043/0003-3219(2000)070<0415:ROIAEE>2.0.CO;2 · doi ↗ · pubmed ↗