Improvement of perceived cochlear implant sound quality through individualized psychoacoustic-based frequency fitting
Tobias Rader, Lisa Lippl, Joachim Müller

TL;DR
This paper explores how individualized frequency fitting based on psychoacoustics can improve sound quality for cochlear implant users.
Contribution
A novel individualized frequency band allocation method based on binaural perceptual pitch matching is introduced for cochlear implants.
Findings
Individualized fitting led to improved speech perception and sound quality compared to default settings.
Frequency allocations were shifted toward lower frequencies, with larger adjustments for the second implant.
The method requires preserved hearing in one ear and good pitch discrimination abilities.
Abstract
In recent years, there has been a trend toward more individualization in the fitting of cochlear implants (CI). Here, a new individualized approach to frequency band allocation was used. This approach is based on binaural perceptual pitch matching. The patient had congenital bilateral progressive sensorineural hearing loss due to Usher Syndrome. He had used hearing aids in both ears since the age of 4 years. In his mid-40s, he received a CI on his right ear and, ten months later, a second CI on the left ear. Adjustments to the frequency band allocations were made, guided by the binaural perceptual pitch matching of piano notes. For the first CI, pitch matching was performed using the contralateral ear as the reference, which had preserved low-frequency residual hearing (bimodal pitch matching). For the second CI, pitch matching was performed using the first implanted side as the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
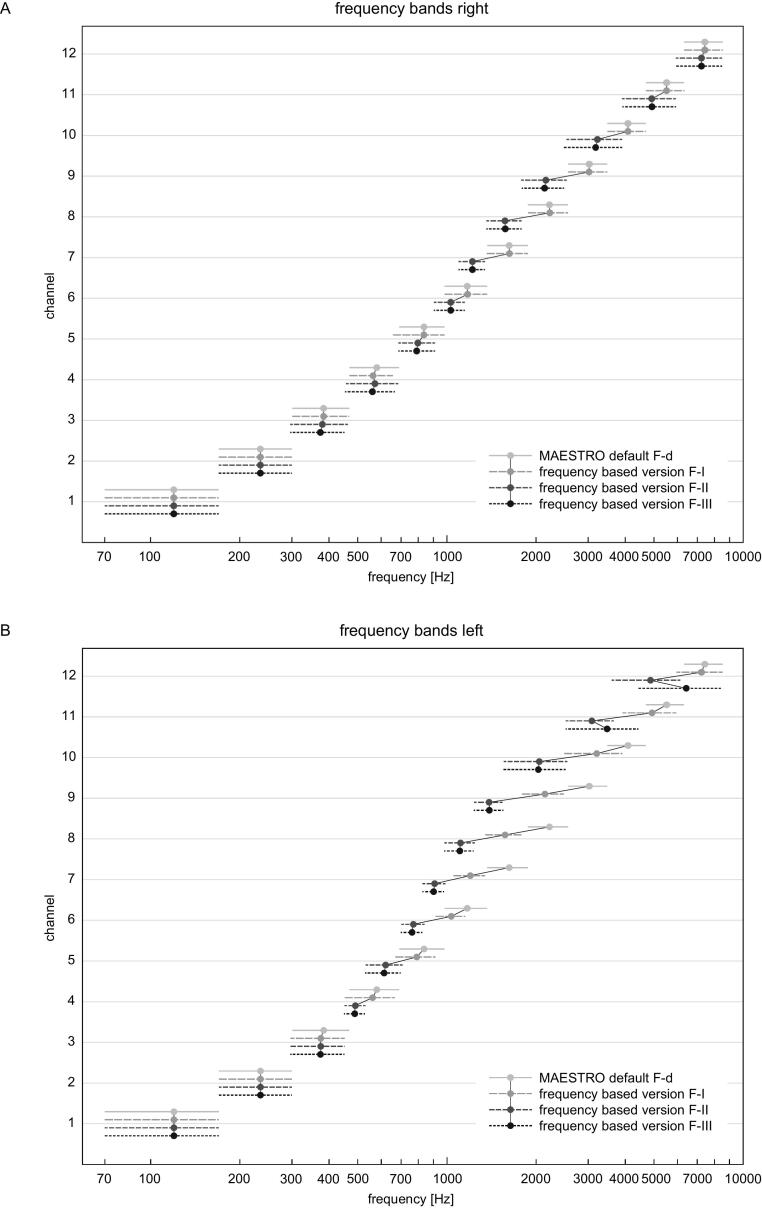 Figure 1
Figure 1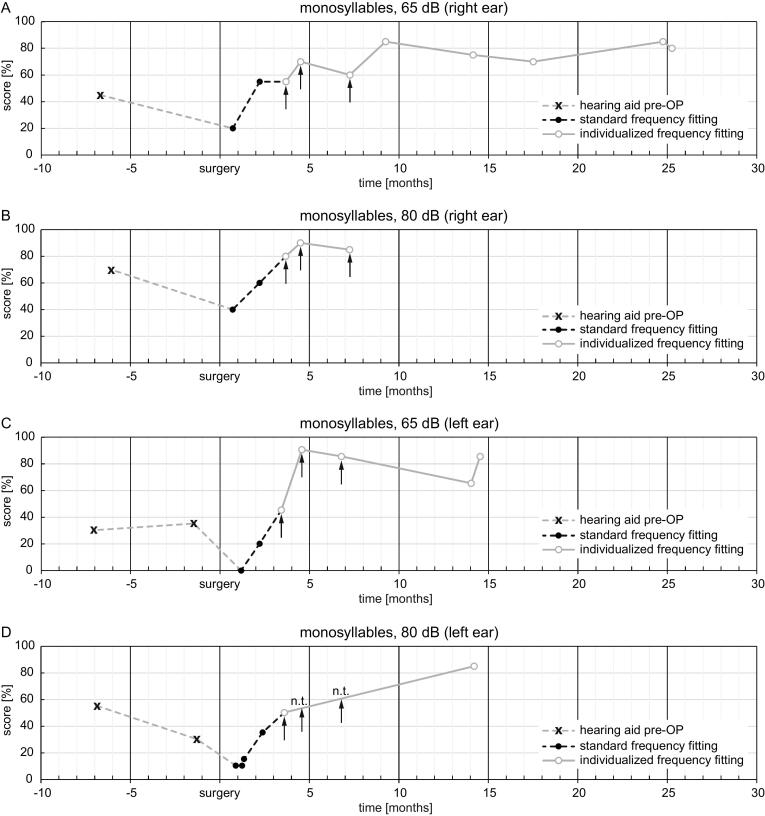 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHearing Loss and Rehabilitation · Noise Effects and Management · Acoustic Wave Phenomena Research
Objective
As part of their sound coding strategies, cochlear implant (CI) audio processors separate the acoustic input signal into distinct frequency bands, each of which is then allocated to the corresponding electrode contact. All CIs are initially programmed with a default frequency allocation table which can be modified using the clinical fitting software.
Mismatches can occur between frequency band assigned to an electrode contact and the range of perceived frequencies elicited by that electrode contact. Mismatches can alter the perception of pitch, inhibit binaural fusion, and may also impact sound quality and speech perception [1], [2], [3], [4]. One source of these mismatches may be the use of the Greenwood function for place-pitch mapping, which can yield frequency allocations that are inappropriately high [5], [6], [7], [8].
A potential alternative to place-pitch mapping functions is the use of individualized psychoacoustic fitting. This can be accomplished when there is sufficient residual hearing in the contralateral ear for pitch matching studies. Here we report the results of such a music based fitting procedure.
Patient
2
The patient, a male in his mid-40s, presented with congenital bilateral profound sensorineural hearing loss due to Usher Syndrome. Hearing aid use began at the age of 4 years. Despite his hearing loss, this patient developed a musical talent and could play several instruments. He had been implanted on the right side with a MED-EL SYNCHRONY2 CI with a 31.5 mm FLEXSOFT array. The array was fully inserted, verified by X-ray imaging with Stenvers view [9].
In the contralateral left ear, the hearing thresholds were 15–30 dB HL between 125 and 1 kHz and ≥65 dB HL between 1.5 and 9 kHz. In this ear he had worn a hearing aid (PHONAK Naida B70 SP) for a duration of 1.5 years.
Due to the progressive nature of his hearing loss, and to the degree of low-frequency residual hearing in the contralateral ear, the patient was offered to transition to electric-acoustic stimulation in that ear. However, the patient opted instead for a conventional CI partly due to concerns over his progressive loss of both vision and hearing.
Ten months after the first CI, the patient received a second CI in the left ear; a SYNCHRONY2 with the FLEXSOFT array. Following this, speech comprehension and reported enjoyment of music rapidly developed beyond what had been achieved with the hearing aids. After the second surgery, no residual hearing remained in either ear. SONNET2 audio processors with FS4 speech coding strategies were used in both ears. The stimulation rates of the electrodes were not modified. The number of fine structure channels remained unchanged at four during all fitting sessions. The electrical thresholds (T-values) and MCL-values (most comfortable loudness) were checked during the adaptation sessions and adjusted slightly if necessary.
Intervention
3
Pitch-matching experiments were performed after the first implantation. The patient was asked to compare the perceived pitch of two piano notes, played sequentially by himself on two keyboards, as heard the first through the CI (using the FS4 coding strategy) and the second through the non-implanted ear. He changed the second note on the keyboard until it matched the pitch of the first note. The patient documented the fundamental frequencies of the notes played and the fundamental frequencies of the corresponding pitches he perceived with each listening modality. For example when the patient was presented with the piano note c3 (1047 Hz), he stated that the perceived pitch via the CI was perceived as a2 (880 Hz) about three semitones lower than via the non-implanted ear.
Using the clinical fitting software of the manufacturer, we adjusted the center frequencies of the filter bands for the CI to attempt to match the pitch perceived with the unimplanted ear. The upper and lower cutoff frequencies of each frequency band were also changed so that that no gaps occurred in the filter bank, and so the shift was approximately equal for neighboring channels. The overall frequency range was kept at the default 70–8500 Hz.
After the second implantation, pitch-matching experiments were again conducted, this time with the left ear, using the first-implanted right ear as the perceptual reference.
Main outcome measures
4
The main outcome measures were the upper, lower, and center frequency allocations of each electrode contact, as well as scores on the Freiburg monosyllabic speech perception test (FMT) [10] and the subjective feedback of the patient regarding the sound quality with his devices.
Results
5
For the right ear, frequency allocations were changed across three post-operative fitting sessions (denoted F-I to F-III). The first session was performed two months after surgery. The center frequencies of channels 4 and 5 were both reduced by 16 Hz. Three months after surgery (F-II), the center frequencies of channels 3 and 5–12 were also reduced by 4–860 Hz and the center frequency of channel 4 was increased by 8 Hz. Six months after surgery (F-III), the center frequencies of channels 3–5, 9, and 10 were reduced by 10–884 Hz.
Fig. 1A shows the original (default) and psychoacoustic-based frequency band allocations of the right CI over time. The frequency adjustments on the right ear ranged from 4 Hz to 884 Hz (0.02 to 0.5 octaves) lower than the corresponding default center frequencies. There were no frequency adjustments to channels 1 and 2. With the final individualized map, the greatest frequency shifts were made at channel 7 (406 Hz, 0.42 octaves), channel 8 (649 Hz, 0.5 octaves), and channel 9 (884 Hz, 0.5 octaves).Figure 1. Frequency bands over the time for (A) right and (B) left side CIs. The grey line represents the default frequency bands of the fitting software (MAESTRO). The dashed and dotted lines show the frequency bands after individualized psychoacoustic fitting. Dots represent the center frequencies of each channel; the length of the line represents the length of each frequency band (upper and lower cutoff frequency). F-I, F-II, and F-III are the first, second, and third individualized fittings, respectively. The center frequencies of the different fittings are connected by lines.
After the second CI implantation, individualized psychoacoustic frequency fitting was also performed on the left ear, using the implanted right ear as the reference. Two months after surgery (F-I), the center frequencies of channels 3–12 were reduced by 10–890 Hz. One month later (F-II), the center frequencies of channels 4-12 were further reduced by 90–2510 Hz. At six months after surgery (F-III), the frequency bands of channels 2, 3, 5–8, 10 were reduced by 2–2036 Hz and the center frequencies of channels 9, 11, and 12 were increased by 7–1584 Hz.
Fig. 1B shows the original (default) and psychoacoustic guided frequency band allocations of the left CI over time. The frequency adjustments on the right ear ranged from 2 to 2510 Hz (0.01 to 1.11 octaves) lower than the corresponding default center frequencies. There were no frequency adjustments to channel 1. The final individualized map had the greatest frequency shifts at channel 8 (1111 Hz, 1.0 octaves), channel 9 (1620 Hz, 1.11 octaves), and channel 10 (2036 Hz, 1.0 octaves).
Fig. 2 shows the aided speech perception scores on the FMT with each ear tested separately. Speech was presented in free field at 65 dB and at 80 dB. In general, FMT scores increased over time, with some variation which was attributed to acclimatization to the new fittings and to the measurement uncertainty of the FMT.Figure 2. Freiburg monosyllable test scores in free field at (A) 65 dB, right ear; (B) 80 dB, right ear; (C) 65 dB, left ear; (D) 80 dB, left ear. Grey dashed lines show pre-operative aided scores. The black dashed lines show the scores with the default frequency allocations. The grey lines show the scores with the individualized frequency fittings. Arrows indicate the timepoints of F-I, F-II, and F-III for each ear. n.t.: not tested due to high scores at 65 dB.
The results in speech perception scores do not indicate that the improvement in speech comprehension was caused by the individualized psychoacoustic-based frequency fitting. It is certainly overlaid by the rehabilitative learning process.
After these adjustments, the perceived sound quality of the CIs, especially with regard to playing the piano and to the enjoyment of music, was reported to be significantly better. According to the patient, the improvements which he perceived after adjustments to the first CI contributed to his decision to opt for a second CI on the contralateral ear.
Conclusions
6
This case illustrates the potential of individualizing fitting via psychoacoustic pitch matching. As reported in previous studies, the perceived pitch in this case was up to 1.11 octaves lower than predicted by the Greenwood function [6], [7], [8]. With both ears, all frequency shifts in the final maps were towards lower frequencies relative to their default allocations. The frequency shifts of the second CI were larger in magnitude compared to the first CI. The apical channels 1 and 2 provided the least perceptual mismatches with their default frequency allocations. These results are in accord with a previous pitch matching study [11], [12].
Individualized psychoacoustic fitting may provide a useful alternative to fitting methods that rely on pitch-place functions to assign frequencies to electrode contacts. In this case, the procedure yielded perceived improvements in both sound quality and the enjoyability of music.
Speech perception test scores generally increased over time, as scores were higher with the individualized fitting compared to with the default frequency allocation. However, it is not possible to determine what proportion of this improvement, if any, can be attributed to the individualized fitting and what proportion can be attributed to the general improvement of speech perception which is typically observed over the first few months of CI use.
This procedure has some limitations. These include the necessity for functional residual hearing in at least one ear. The listener must also be able to not only perceive pitch differences, but to accurately report their magnitudes, a skill typically reserved for trained musicians. The method is also rather time consuming and can be challenging for both the patient and audiologist. Nevertheless, this method can yield improvements in the perceived sound quality with the CI.
CRediT authorship contribution statement
Tobias Rader: Writing – review & editing, Writing – original draft, Visualization, Validation, Supervision, Software, Resources, Project administration, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. Lisa Lippl: Writing – review & editing, Writing – original draft, Validation, Methodology, Investigation, Formal analysis, Data curation. Joachim Müller: Writing – review & editing, Resources.
Funding
This research received no external funding.
Data Availability Statement
The anonymized patient data can be made available on request due to privacy/ethical restrictions.
Declaration of competing interest
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: T.R. and J.M. received funding for other projects supported by different medical device companies. L.L. is an employee of MED-EL Deutschland GmbH, Starnberg, Germany.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Canfarotta M.W.O'Connell B.P.Buss E.Pillsbury H.C.Brown K.D.Dillon M.T.Influence of age at cochlear implantation and frequency-to-place mismatch on early speech recognition in adults Otolaryngol Head Neck Surg 162620209269323217857410.1177/0194599820911707 PMC 8590812 · doi ↗ · pubmed ↗
- 2Breitsprecher T.M.Baumgartner W.D.Brown K.Effect of cochlear implant electrode insertion depth on speech perception outcomes: a systematic review Otol Neurotol Open 342023 e 0453851654110.1097/ONO.0000000000000045 PMC 10950166 · doi ↗ · pubmed ↗
- 3Kurz A.Herrmann D.Hagen R.Rak K.Using anatomy-based fitting to reduce frequency-to-place mismatch in experienced bilateral cochlear implant users: a promising concept J Pers Med 137202311093751172210.3390/jpm 13071109 PMC 10381201 · doi ↗ · pubmed ↗
- 4Mertens G.Van de Heyning P.Vanderveken O.Topsakal V.Van Rompaey V.The smaller the frequency-to-place mismatch the better the hearing outcomes in cochlear implant recipients?Eur Arch Otorhinolaryngol 27942022187518833413177010.1007/s 00405-021-06899-y · doi ↗ · pubmed ↗
- 5Greenwood D.D.A cochlear frequency-position function for several species–29 years later J Acoust Soc Am 876199025922605237379410.1121/1.399052 · doi ↗ · pubmed ↗
- 6Rader T.Döge J.Adel Y.Weissgerber T.Baumann U.Place dependent stimulation rates improve pitch perception in cochlear implantees with single-sided deafness Hear Res 3392016941032737447910.1016/j.heares.2016.06.013 · doi ↗ · pubmed ↗
- 7Dorman M.F.Spahr T.Gifford R.An electric frequency-to-place map for a cochlear implant patient with hearing in the nonimplanted ear J Assoc Res Otolaryngol 8220072342401735171310.1007/s 10162-007-0071-1PMC 2441831 · doi ↗ · pubmed ↗
- 8Boëx C.Baud L.Cosendai G.Sigrist A.Kós M.I.Pelizzone M.Acoustic to electric pitch comparisons in cochlear implant subjects with residual hearing J Assoc Res Otolaryngol 7220061101241645021310.1007/s 10162-005-0027-2PMC 2504582 · doi ↗ · pubmed ↗