The effect of shared decision-making for critically ill patients: a systematic review and meta-analysis
Yangyang Wang, Jiaqi Li, Na Yin, Baolin Huang, Kaibo Shen, Sheng He, Minfei Yang, Ju Zhang

TL;DR
Shared decision-making in critical care does not reduce mortality or hospital stays but may shorten ICU stays for patients who die.
Contribution
This study provides the first meta-analysis on shared decision-making in critical care, revealing specific effects on ICU length of stay for deceased patients.
Findings
Shared decision-making did not significantly affect mortality or overall ICU/hospital length of stay.
It reduced ICU length of stay for deceased patients but had no impact on mental health outcomes for surrogates.
Decision-making and communication quality remained unchanged with shared decision-making interventions.
Abstract
This systematic review and meta-analysis assessed the impact of shared decision-making on critically ill patients, focusing on outcomes such as mortality, intensive care unit (ICU) and hospital length of stay (LOS), and mental health symptoms in patients and their surrogates. Following PRISMA guidelines, we searched PubMed, EMBASE, Web of Science, and Cochrane databases through March 2025 for randomized controlled trials (RCTs) assessing shared decision-making interventions in critically ill patients or surrogates. Risk of bias was assessed using the Cochrane tool, and data synthesis employed fixed or random-effects models based on heterogeneity. Fifteen RCTs (2003–2025) involving 3,678 ICU patients and 2,777 surrogates were analyzed. Shared decision-making showed no significant association with all-cause mortality [risk ratio (RR) 1.05, 95% CI = 0.97–1.15]. Data analysis shows that…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
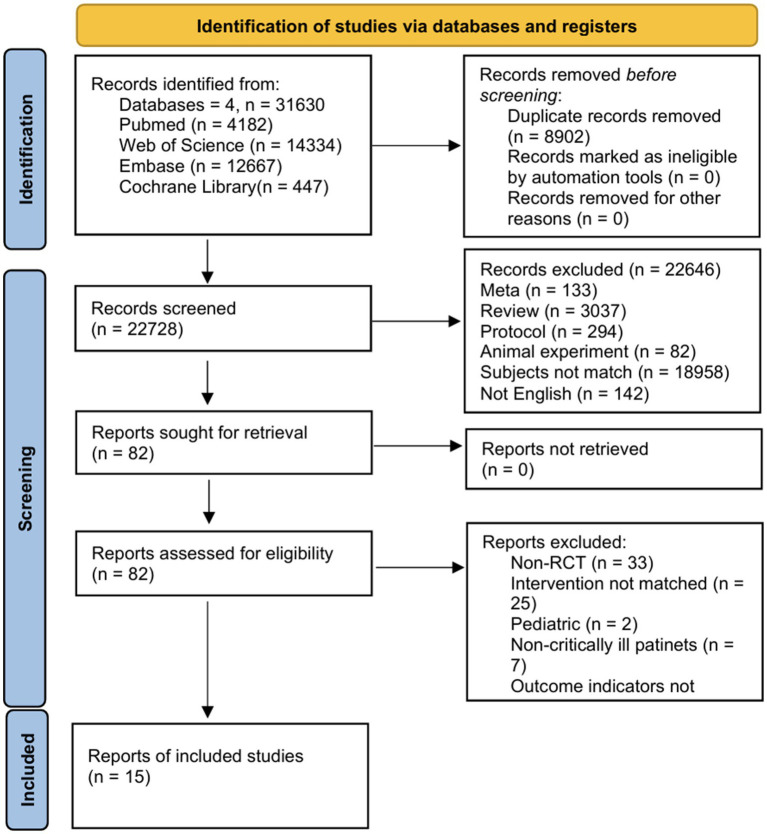 Figure 1
Figure 1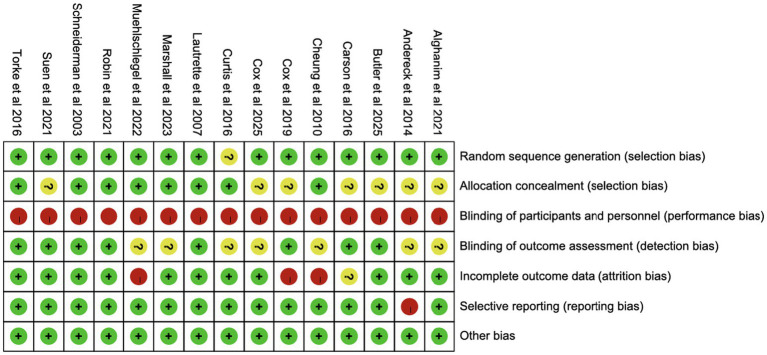 Figure 2
Figure 2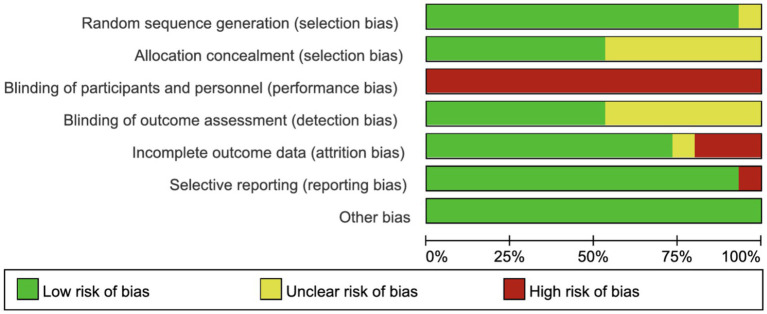 Figure 3
Figure 3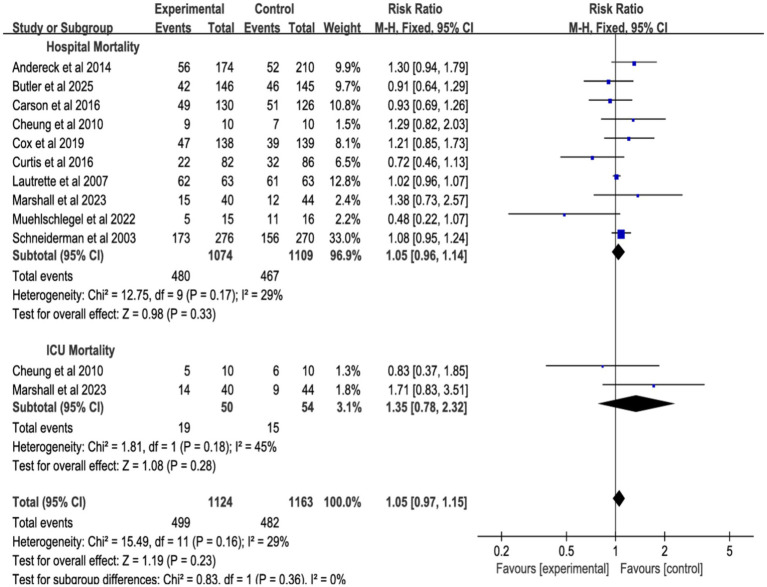 Figure 4
Figure 4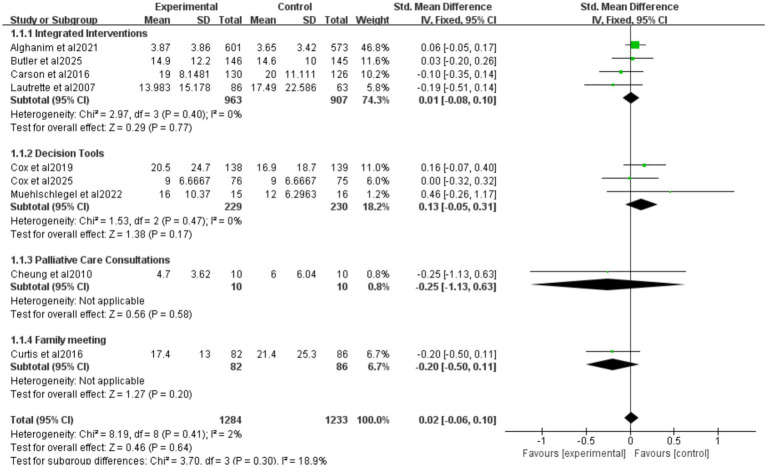 Figure 5
Figure 5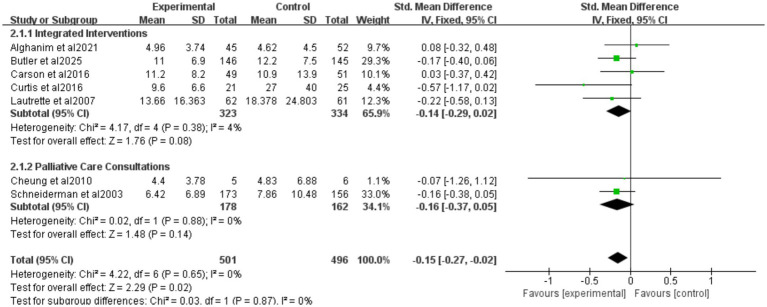 Figure 6
Figure 6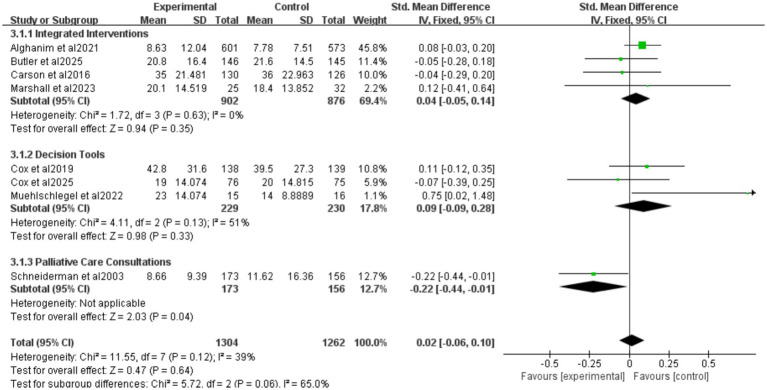 Figure 7
Figure 7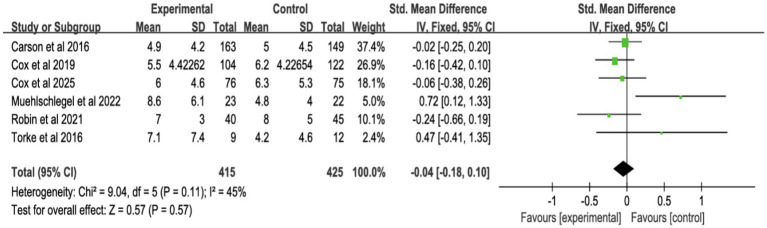 Figure 8
Figure 8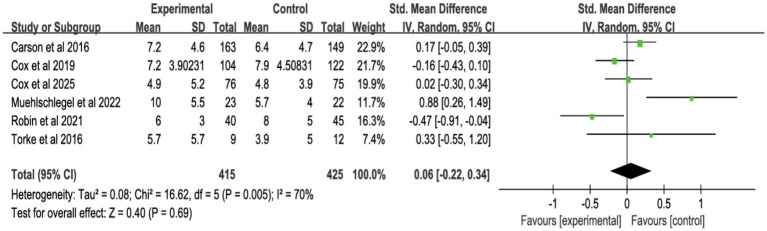 Figure 9
Figure 9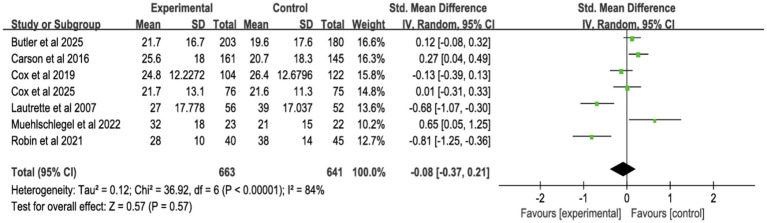 Figure 10
Figure 10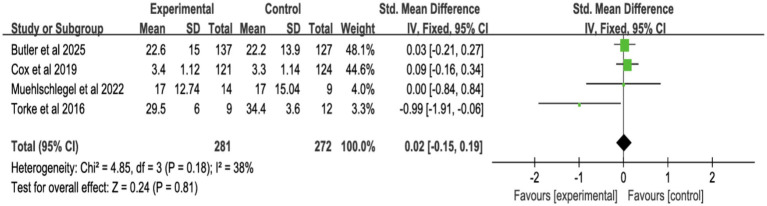 Figure 11
Figure 11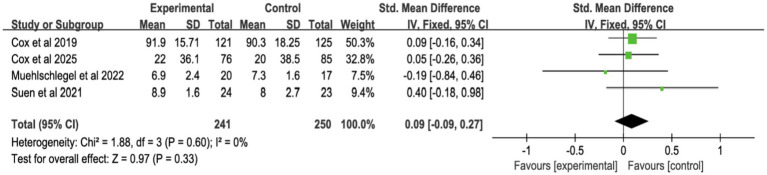 Figure 12
Figure 12| Author, year, country | Sites | Participants | Intervention | Types of interventions | No. of participants (experimental/control) | Age (years, experimental/control, mean ± SD) | Outcome and outcome measure | ||
|---|---|---|---|---|---|---|---|---|---|
| Patients (Male/Female) | Shared decision-makings (Male/Female) | Patients | Shared decision-makings | ||||||
| Cox et al. ( | Multicenter RCT of 6 ICUs | Critically ill older adult patients and their family members with elevated palliative care needs | An automated electronic health record–integrated, mobile application–based communication platform | Decision tools | 76(42/34)/75(44/31) | 76(22/53)/75(18/57) | 69.2 ± 9.8/70.5 ± 9.6 | 57.3 ± 12.9/57.4 ± 13.0 | Depression, anxiety, surrogates’ symptoms of posttraumatic stress disorder, ICU LOS (all patients), hospital LOS, overall QOC |
| Butler et al. ( | Multicenter RCT of 6 ICUs | Patients ≥21 years old, with >40% risk of in-hospital death or long-term impairment, dependent on >2 ADLs, and their surrogates | Four Supports intervention adds: emotional support; communication support; decisional support | Integrated interventions | 146(75/71)/145(88/57) | 233(55/168)/209(63/146) | 61.0 ± 17.1/62.2 ± 15.6 | 51.1 ± 15.0/53.4 ± 15.2 | Hospital mortality, surrogates’ symptoms of posttraumatic stress disorder, ICU LOS (all patients), ICU LOS (patients who died), hospital LOS, quality of decision-making surrogate |
| Marshall et al. ( | Multicenter RCT of 9 ICUs | ICU patients who were nutritionally high-risk and/or those at risk of dying in the ICU or during subsequent hospitalization and their adult family members | Nutrition intervention and decision support intervention | Integrated interventions | 40(25/15)/44(31/13) | 40(12/28)/44(11/33) | 73.0 ± 8.0/71.5 ± 8.2 | 56.4 ± 16.2/58.1 ± 16.1 | Hospital mortality, ICU mortality, hospital LOS |
| Muehlschlegel et al. ( | Multicenter RCT of 2 ICUs | Critically ill patients with severe acute brain injury and their surrogates | Provided a technical orientation of the decision-aid to the intervention group surrogates without any mention of medical information and reminded them to complete the worksheet | Decision tools | 20(11/9)/21(15/6) | 33(5/27)/33(11/22) | 58 ± 19/64 ± 21 | 51 ± 17/57 ± 15 | Hospital mortality, depression, anxiety, surrogates’ symptoms of posttraumatic stress disorder, ICU LOS (all patients), hospital LOS, quality of decision-making surrogate, overall QOC, length of mechanical ventilation |
| Suen et al. ( | Single center RCT of 2 ICUs | Critical patients in ICU and their surrogates | Surrogates complete Family Support Tool before meetings, provide summary to ICU team, and schedule family meetings | Structured communication or family meeting | 25(13/12)/25(11/14) | 23(6/17)/25(12/13) | 65.6 ± 17.7/69 ± 13.2 | 58.65 ± 12.62/54.28 ± 13.15 | Overall QOC |
| Robin et al. ( | Single center RCT of 3 ICUs | Adult patients for whom a decision to withhold and withdraw life-sustaining therapies in the ICU | Information pamphlet | Decision tools | 45(28/17)/45(29/16) | 45(20/25)/45(14/31) | 69 (62–77)/71 (59–80) | 54 (47–65)/54 (47–66) | Depression, anxiety, surrogates’ symptoms of posttraumatic stress disorder |
| Alghanim et al. ( | Single center RCT of 2 ICUs | Critical patients in MICU or CICU and their surrogates | Chaplain patient navigator served as a health liaison for patients and their families, elicited their values and preferences, and organized admission, follow-up, and | Integrated interventions | 601(334/266)/573(287/286) | Not mentioned | 63(53–76)/62(53–75) | Not mentioned | ICU LOS (all patients), ICU LOS (patients who died), hospital LOS |
| Cox et al. ( | Multicenter RCT of 5 hospital | Adult patients receiving prolonged mechanical ventilation and their surrogates | Web-based decision aid provided prognostic estimates, treatment options, and clarified patient values for family meetings. | Decision tools | 138(88/50)/139(89/50) | 137(41/96)/138(33/105) | 52.9 ± 17.9/54.0 ± 16.6 | 49.9 ± 13.5/52.6 ± 11.6 | Hospital mortality, depression, anxiety, surrogates’ symptoms of posttraumatic stress disorder, ICU LOS (all patients), hospital LOS, quality of decision-making surrogate, overall QOC, length of mechanical ventilation |
| Torke et al. ( | Single center RCT | Sedated or comatose ICU patients | Dedicated trained nurse acting as family navigator | Structured communication or family meeting | 13(4/9)/13(7/6) | 13(9/4)/13(3/10) | 53.27 (14.18)/57.42 (11.03) | 50.93 (12.01)/46.16 (17.36) | Depression, anxiety, quality of decision-making surrogate |
| Curtis et al. ( | Multicenter RCT of 2 ICUs | ICU patients and family members | A communication facilitator enhances ICU communication self-efficacy for families and clinicians through interviews, meetings, and follow-up | Structured communication or family meeting | 82(55/27)/86(53/33) | 131(38/93)/137(41/96) | 52.1 ± 17.2/55.3 ± 18.8 | 49.5 ± 12.0/52.4 ± 14.2 | Hospital mortality, ICU LOS (all patients), ICU LOS (patients who died) |
| Carson et al. ( | Multicenter RCT of 4 ICUs | Adult patients (≥21 years) requiring 7 days of mechanical ventilation, with their family surrogates enrolled in the study | At least 2 structured family meetings led by palliative care specialists and provision of an informational brochure | Integrated interventions | 130(64/66)/120(55/65) | 184(56/128)/181(50/131) | 58 (55.2–60.8)/57 (54.0–59.7) | 51 (48.8–52.8)/51 (48.6–52.7) | Hospital mortality, depression, anxiety, surrogates’ symptoms of posttraumatic stress disorder, ICU LOS (all patients), ICU LOS (patients who died), hospital LOS, length of mechanical ventilation |
| Cheung et al. ( | Single center RCT | Patients with terminal or preterminal conditions, where escalating or continuing treatment is unlikely to improve their clinical condition | A consultation and subsequent management by a palliative care team | Palliative care consultations | 10(5/5)/10(3/7) | 共9 | 72(20)/83(14) | Total 9 | Hospital mortality, ICU mortality, ICU LOS (all patients), ICU LOS (patients who died) |
| Andereck et al. ( | Single center RCT of medical/surgical ICU | Patients with ICU lengths of stay of 5 days or greater | Ethics: Proactive ethics intervention involves a trained bioethicist in the care of all ICU patients | Palliative care consultations | 174(83/91)/210(98/112) | 146/173 | 60 ± 15.8/61 ± 16.2 | Not reported | Hospital mortality |
| Lautrette et al. ( | Multicenter RCT of 22 ICUs | Patient would die within a few days | A proactive end-of-life conference and a brochure | Integrated interventions | 63(33/30)/63(37/26) | 57(17/40)/52(12/40) | 74(56–80)/68(56–76) | 54(47–58)/54(46–64) | Hospital mortality, surrogates’ symptoms of posttraumatic stress disorder, ICU LOS (all patients), ICU LOS (patients who died) |
| Schneiderman et al. ( | Multicenter RCT of 7 hospitals | Patient in whom treatment conflicts were identified | Ethics consultation offered | Palliative care consultations | 276(145/131)/270(148/122) | 262/263 | 67.5 ± 17.2/67.5 ± 17.4 | Not reported | Hospital mortality, ICU LOS (patients who died), hospital LOS, length of mechanical ventilation |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPalliative Care and End-of-Life Issues · Patient-Provider Communication in Healthcare · Intensive Care Unit Cognitive Disorders
Background
1
Shared decision-making, a collaborative process integrating clinical expertise with patient and surrogate values, seeks to align treatment choices with patient preferences while reducing decisional conflict (1). In critical care settings, where patients often lack decision-making capacity, physicians rely on proxies (e.g., family members) to facilitate shared decision-making (2). However, time constraints, prognostic uncertainty, and surrogate emotional burdens frequently compromise shared decision-making effectiveness in intensive care units (ICUs) (3). Institutional barriers, including clinician time limitations, inadequate training, and suboptimal communication environments, further hinder implementation (4).
Shared decision-making interventions, ranging from structured family conferences and decision aids to ethics consultations and palliative care guidance (5, 6)—aim to reconcile treatment plans with patient values and alleviate surrogate distress. Despite improving transparency, shared decision-making often struggles to address the urgency and complexity of ICU decisions. For instance, surrogate decision-makers for patients with severe acute brain injury requiring prolonged mechanical ventilation report persistent anxiety and depression (7), while those managing chronic critical illness face elevated post-traumatic stress disorder (PTSD) risks (8). Although some evidence suggests shared decision-making may reduce ICU length of stay (LOS), findings remain inconsistent.
Prior meta-analyses report conflicting outcomes: ICU-focused shared decision-making interventions may shorten ICU stays without affecting mortality (9), whereas others propose mortality and hospital LOS reductions (10). Paradoxically, decision aids might prolong hospitalization despite enhancing surrogate knowledge (11). These discrepancies likely stem from heterogeneous study designs, populations, and outcome measures. To resolve this uncertainty, we systematically analyzed randomized controlled trials (RCTs) evaluating shared decision-making’s impact on mortality, psychosocial outcomes, and healthcare utilization in critically ill patients and their surrogates.
Methods
2
This study followed the Cochrane Handbook for Systematic Reviews of Interventions (12) and was reported in accordance with the PRISMA guidelines (13). The protocol is registered with the International Prospective Register of Systematic Reviews (CRD420251013215).1
Data sources and search strategy
2.1
A comprehensive search was conducted in March 2025 across PubMed, EMBASE, Web of Science, and Cochrane databases, from inception to March 2025. Search terms included Medical Subject Headings (MeSH) and key terms such as “critical illness,” “shared decision-making,” “decision aids,” and “family.” The full search strategy is detailed in Supplementary Tables S1–S4. We also manually searched reference lists of relevant studies and reviews (14–16).
Inclusion and exclusion criteria
2.2
Eligible studies were screened based on the following criteria:
Population: Critically ill patients (≥18 years) or their surrogates (e.g., family members).
Intervention: Any form of shared decision-making between patients, doctors, and family members.
Control: Routine care or no intervention.
Outcomes: All-cause mortality, ICU length of stay (LOS), hospital LOS, depression, anxiety, PTSD symptoms, decision-making quality and communication quality.
Study Design: Randomized controlled trials (RCTs) published in English, with no date restrictions.
Studies were excluded if they: (1) Interventions targeted only at healthcare professionals (doctors or nurses); (2) Qualitative studies, protocols, conference abstracts, case reports, letters, reviews; (3) Cross-over controlled RCTs; (4) Absence of the outcomes of interest; (5) Lack of the full text or the relevant complete study.
Study selection
2.3
Two reviewers (WYY and LJQ) independently screened all titles and abstracts, resolving discrepancies through consensus with a third reviewer. Only studies meeting all inclusion criteria proceeded to full-text review and data extraction.
Data extraction
2.4
Two reviewers (WYY and LJQ) independently extracted data using standardized forms, with a third reviewer (ZJ) verifying accuracy. Any discrepancies were resolved through discussion. Data collected included study characteristics (author, year, country, design, sample size), participant characteristics, intervention details, and outcome data.
Intervention categorization and rationale for synthesis
2.5
We recognized that the shared decision-making intervention measures included in the studies were heterogeneous in form and implementation. To address this issue and provide a basis for data pooling, we classified the intervention measures into four categories based on their core components.
Structured communication or family meeting
2.5.1
Interventions involving dedicated, protocol-driven meetings or communication support led by trained personnel (for example, nurses, palliative care specialists, ethics consultants) to facilitate family-clinician dialogue.
Decision tools
2.5.2
Interventions employing paper-based or electronic tools (for example, pamphlets, worksheets, web-based platforms) designed to provide prognostic information, clarify patient values, and prepare surrogates for decision-making.
Integrated interventions
2.5.3
Interventions combining elements of structured communication with additional supportive components, such as family navigation, spiritual care, or specific clinical management guidance.
Palliative care consultations
2.5.4
Formal consultations conducted by an institutional ethics committee or a specialized palliative care team to address treatment conflicts or goals-of-care discussions.
Risk of bias
2.6
The Cochrane Risk of Bias tool (17) was used by two reviewers to assess the methodological quality of each study. The assessment covered random sequence generation, allocation concealment, blinding, outcome assessment, incomplete data, selective reporting, and other potential biases. Discrepancies were resolved by a third reviewer.
Data synthesis and analysis
2.7
Meta-analysis was performed using Review Manager 5.4. Binary outcomes were expressed as Risk Ratios (RR) with 95% confidence intervals (CI), while continuous outcomes were reported as mean difference (MD) or standardized mean difference (SMD) with 95% CI. For continuous outcomes, if different studies used the same unit of measurement but different scales, or different units of measurement, SMD was selected as the effect size indicator; SMD was calculated based on the mean, standard deviation, and sample size of each study through the built-in algorithm of Review Manager 5.4 software, reflecting the standardized difference in outcome indicators between the intervention group and the control group. For studies reporting only median and interquartile range, raw data were sought from authors, and where unavailable, McGrath’s method was used to convert medians to means and standard deviations (18, 19). Handling of studies with multiple time points: If the included studies reported the same outcome indicator at multiple time points, the time point consistent with the definition of the study’s primary outcome, was prioritized for data extraction and pooling; if the study did not clearly define the primary time point, the time point closest to the end of the intervention was selected. All 15 randomized controlled trials included in this study were two-arm trials, and no multi-arm trials were involved, so no data processing related to multi-arm trials was required. Fixed-effect models were used when I^2^ < 50% and p ≥ 0.1, indicating low heterogeneity. For significant heterogeneity (I^2^ > 50% or p < 0.1), random-effects models were applied, and subgroup analyses were conducted to explore sources of heterogeneity. Subgroup variables included all-cause mortality, surrogate symptoms (depression, anxiety, PTSD), ICU and hospital LOS, decision-making and communication quality, and mechanical ventilation duration. A p-value < 0.05 was considered statistically significant in subgroup analyses. A sensitivity analysis was performed to assess result robustness by sequentially excluding studies, and publication bias was evaluated using Egger’s test, with a p > 0.05 considered as no significant publication bias. The results of Egger’s test for each outcome are reported in the corresponding result sections (Supplementary Figures S2, S7).
Assessment of the quality of evidence
2.8
We used the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach to assess the quality of evidence of the included studies (20) (Supplementary Table S5).
Results
3
Literature selection process
3.1
The initial search identified 31,630 records, supplemented by 3 additional articles from manual searching. After screening, 15 RCTs were included in the final analysis (Figure 1).
Flow chat for selecting the articles in this systematic review.
Study characteristics
3.2
Table 1 presents the characteristics of the 15 RCTs. These studies, published between 2003 and 2025, involved 3,678 ICU patients and 2,777 surrogates. Eleven studies (14, 15, 21–29) were conducted in the U.S., two (30, 31) in Australia, and two (16, 32) in France. The studies included both single-center (6) and multi-center (9) settings, with patient ages ranging from 34.9 to 97 years and surrogates’ ages from 34 to 74.2 years. Various outcomes were reported, including mortality, surrogate depression, anxiety, PTSD, ICU and hospital length of stay, quality of decision-making, and mechanical ventilation duration.
Three studies (25, 28, 29) employed structured communication or family meetings as the intervention methods, four studies (22, 24, 27, 32) employed decision Tools, five studies (16, 21, 23, 26, 31) employed Integrated Interventions, three studies (14, 15, 30) employed palliative care consultations.
Risk of bias
3.3
Except for one study lacking details on random sequence generation, most studies reported adequate randomization. Eight studies exhibited low risk of selection bias, while seven did not specify allocation concealment. None of the trials blinded participants or staff, but eight blinded outcome assessments. Three studies had high follow-up loss, and one study did not report follow-up rates. One study lacked information on public registration or protocol availability (Figures 2, 3).
Risk of summary.
Risk of graph.
Meta-analysis
3.4
All-cause mortality in different environments
3.4.1
The meta-analysis, incorporating 10 studies (Figure 4; Supplementary Figure S1), 10 studies showed no significant effect of shared decision-making on hospital mortality (RR = 1.05, 95% CI = 0.96–1.14, p = 0.33, I^2^ = 29%), 2 studies showed no significant effect of ICU mortality (RR = 1.35, 95% CI = 0.78–2.23, p = 0.28, I^2^ = 45%), 10 studies showed no significant effect of or overall mortality (RR = 1.05, 95% CI = 0.97–1.15, p = 0.23, I^2^ = 0%). Heterogeneity was low (<50%), and a fixed-effect model was used.
Forest plot of the effect of all-cause mortality in different environments.
Length of stay
3.4.2
Nine studies reported ICU length of stay (LOS) for all patients (Figure 5), seven for patients who died (Figure 6), and eight for hospital LOS (Figure 7). Shared decision-making did not reduce ICU LOS for all patients (SMD = 0.02, 95% CI = −0.06 to 0.10, p = 0.64, I^2^ = 18.9%) or hospital LOS (SMD = 0.02, 95% CI = −0.06 to 0.10, p = 0.64, I^2^ = 65%). However, for patients who ultimately died, shared decision-making was associated with a statistically significant reduction in ICU LOS (SMD = −0.15, 95% CI = −0.27 to −0.02, p = 0.02, I^2^ = 0%). Indicating that the relative impact of shared decision-making on this outcome is minimal and may not have practical clinical significance. Excluding any one of the studies has little influence on the total result, indicating good stability of the findings. No publication bias was detected in all the results as assessed by Egger’s test, suggesting that the pooled results are reliable (Supplementary Figures S2, S4).
Forest plot of the effect of ICU LOS of all patients.
Forest plot of the effect of ICU LOS of patients who died.
Forest plot of the effect of ICU LOS of hospital length of study.
Intervention categorization of ICU LOS for all patients
3.4.2.1
Four studies reported integrated interventions of ICU LOS for all patients (SMD = 0.01, 95% CI = −0.08 to 0.10, p = 0.77, I^2^ = 0%), three studies reported decision tools of ICU LOS for all patients (SMD = 0.13, 95% CI = −0.05 to 0.31, p = 0.17, I^2^ = 0%), one study reported palliative care consultations of ICU LOS for all patients (SMD = −0.25, 95% CI = −1.13 to 0.63, p = 0.58), and one study reported family meeting of ICU LOS for all patients (SMD = −0.20, 95% CI = −0.50 to 0.11, p = 0.20) (Figure 5). The results were all without statistical significance. This indicates that, despite the different forms of intervention, the directional effect of shared decision-making on the length of stay in the ICU for all patients is consistent.
Intervention categorization of ICU LOS for patients who died
3.4.2.2
Five studies reported integrated interventions of ICU LOS for patients who died (SMD = −0.14, 95% CI = −0.29 to 0.02, p = 0.08, I^2^ = 4%), two studies reported palliative care consultations (SMD = −0.16, 95% CI = −0.37 to 0.05, p = 0.14, I^2^ = 0%) (Figure 6). Neither subgroup was statistically significant. The “decision tools” and “family meeting” subgroups were not included in the analysis, because among the original studies included in this research, studies adopting these two intervention measures did not report data on ICU LOS for deceased patients, resulting in a lack of valid data for analysis.
Intervention categorization for hospital LOS
3.4.2.3
Four studies reported integrated interventions of ICU LOS for hospital LOS (SMD = 0.04, 95% CI = −0.05 to 0.14, p = 0.35, I^2^ = 0%), three studies reported decision tools of ICU LOS for hospital LOS (SMD = 0.09, 95% CI = −0.09 to 0.28, p = 0.33, I^2^ = 51%), one study reported palliative care consultations of ICU LOS for hospital LOS (SMD = −0.22, 95% CI = −0.44 to 0.01, p = 0.04) (Figure 7). The “integrated intervention” and “palliative care consultation” subgroups were not included because the original studies adopting these two types of interventions did not report data on surrogate anxiety scores, resulting in a lack of valid data for analysis.
Surrogates’ symptoms
3.4.3
Six studies assessed surrogate depression (Figure 8), six assessed anxiety (Figure 9), and seven assessed PTSD (Figure 10). Shared decision-making had no significant impact on surrogate depression (SMD = −0.04, 95% CI = −0.18 to 0.10, p = 0.57, I^2^ = 45%), anxiety (SMD = 0.06, 95% CI = −0.22 to 0.34, p = 0.69, I^2^ = 70%), or PTSD symptoms (SMD = −0.08, 95% CI = −0.37 to 0.21, p = 0.57, I^2^ = 84%). Sensitivity analyses confirmed the stability of these findings. No publication bias was detected by Egger’s test (all p > 0.05), indicating that the results of this study are true and reliable (Supplementary Figures S5, S7).
Forest plot of depression symptoms.
Forest plot of anxiety symptoms.
Forest plot of posttraumatic stress disorder.
Quality of decision-making and communication
3.4.4
Four studies reported surrogate decision-making quality (Figure 11; Supplementary Figure S8), and four reported communication quality (Figure 12; Supplementary Figure S9). Shared decision-making had no significant effect on decision-making quality (SMD = 0.02, 95% CI = −0.15 to 0.19, p = 0.81, I^2^ = 38%) or communication quality (SMD = 0.09, 95% CI = −0.09 to 0.27, p = 0.33, I^2^ = 0%).
Forest plot of quality of decision-making by surrogates.
Forest plot of overall quality of communication.
Discussion
4
This review assessed the impact of shared decision-making interventions on 3,678 critically ill patients and 2,777 surrogate decision-makers across 15 RCTs. The findings indicate that shared decision-making reduced ICU LOS for deceased patients compared to standard care, consistent with previous research (33). However, shared decision-making did not significantly affect patient mortality, decision quality, or communication effectiveness, likely due to difficulties in translating shared decision-making principles into measurable clinical outcomes in the high-pressure ICU environment. By incorporating a substantial number of RCTs and larger sample sizes, this analysis strengthens the evidence base for shared decision-making’s role in improving outcomes for ICU patients and their families.
The study indicates that shared decision-making has no impact on in-hospital, ICU-specific, or all-cause mortality. A previous meta-analysis examining surrogate decision-making in critical care also found no significant effect of shared decision-making on hospital mortality rates (9). Several factors contribute to this result. ICU physicians’ prognostic inaccuracies may lead to premature withdrawal of life-sustaining treatments for patients who could recover (34). Additionally, while shared decision-making promotes collaborative decision-making, it does not fundamentally change medical protocols or treatment approaches. It mainly integrates surrogate input into existing frameworks, limiting its ability to alter care plans or mortality outcomes (35). Mortality in critically ill patients is primarily influenced by disease progression, treatment efficacy, and resource availability (36), factors largely independent of shared decision-making. Variability in intervention duration, frequency, and delivery across studies may further reduce its impact on mortality. For example, nurse-led tele-ICU support systems have been more successful in reducing ICU mortality and LOS than remote specialist consultations (10), suggesting the need for further RCTs to explore the best shared decision-making delivery models.
Our analysis reveals that shared decision-making is associated with a reduction in ICU LOS for deceased patients (SMD = −0.15), with no significant effect on overall hospital LOS. Indicating that overall shared decision-making has little or no practical impact on all these outcomes, which is contrary to the traditional common belief. A systematic review of ICU decision-making strategies also supports shared decision-making’s potential to shorten LOS specifically for non-survivors (33). However, this small difference may have limited clinical and economic significance. Regular family meetings, ethics consultations, and palliative care integration appear to improve surrogate understanding of prognosis, facilitating earlier consensus on end-of-life decisions. For patients who die, shared decision-making may prompt timely withdrawal of futile interventions, reducing unnecessary resource use. However, for surviving patients, shared decision-making’s primary value lies in enhancing collaborative decision-making rather than directly accelerating discharge. The unpredictable clinical course of critically ill patients (37) and surrogates’ varied understanding of shared decision-making, shaped by education, communication quality, and emotional stress, introduce additional complexities into LOS outcomes (38). ICU workload pressures (39), time-sensitive decisions, and surrogates’ cognitive overload may further compromise decision quality, leading to suboptimal choices (40). The importance of this finding may lie not in the importance of the effect but in its direction and consistency, it suggests that the shared decision-making process may help avoid non-beneficial life-sustaining treatments in appropriate situations, thereby achieving more efficient and patient-aligned resource utilization at the end of life. These highlight the need for shared decision-making models tailored to the stressors present in ICU settings.
As a patient-centered communication model, shared decision-making is underutilized in mental health contexts (41). A meta-analysis of shared decision-making in breast reconstruction surgery found no significant impact on anxiety levels (42), and decision aids showed limited long-term psychological benefits (11). This study confirms shared decision-making’s limited effect on surrogate mental health outcomes, including depression, anxiety, or PTSD. Surrogates’ emotional burden from poor prognoses, inconsistent clinician communication, and the psychological weight of decision-making responsibility contribute to these outcomes (43, 44). Despite these limitations, shared decision-making remains central to patient-centered care by aligning treatment plans with patient values (45). Personalized, technology-enhanced interventions and trust-building efforts within healthcare teams could optimize shared decision-making’s implementation (4), though these approaches may introduce new operational challenges for providers.
Current evidence suggests shared decision-making does not consistently improve surrogate understanding of medical decisions or enhance communication quality (46), a conclusion supported by this analysis. The complexity of shared decision-making reflects broader systemic factors: institutional culture, resource allocation, and leadership priorities shape its effectiveness (47). Clinicians often lack training in empathy and trust-building, focusing on technical discussions rather than exploring patient values (4). Heavy workloads and the lack of standardized decision aids hinder the in-depth communication needed for effective shared decision-making (5). While palliative care integration in critical care nephrology has shown benefits in decision-making quality (48), inconsistent implementation practices continue to undermine shared decision-making’s potential. Standardized protocols and rigorous outcome measures are needed to resolve ongoing debates about shared decision-making’s role in healthcare communication.
This study exclusively includes RCTs, offering robust evidence that shared decision-making reduces ICU LOS for deceased patients. However, this review has several limitations: (1) The included studies exhibited heterogeneity in the format and delivery of SDM interventions. We proactively addressed this by categorizing interventions and conducting subgroup and sensitivity analyses. These analyses indicated that while operational methods varied, the core SDM components across different intervention types yielded directionally consistent effects on primary outcomes, supporting the rationale for our pooled analysis to estimate the overall effect of the SDM process. Nevertheless, this heterogeneity underscores the need for future trials to provide more detailed descriptions of intervention components to facilitate the identification of the most effective active ingredients; (2) Excluding crossover-design RCTs may limit the comprehensiveness of outcomes due to simplified inclusion criteria; (3) The predominance of U. S.-based trials (11/15 studies) restricts generalizability to regions with distinct decision-making norms, such as Asia or Africa; (4) Including only English-language publications risks overlooking studies in other languages, which may affect the universality of our findings.
Conclusion
5
This systematic review suggests that implementing shared decision-making in critically ill patients may be associated with a minimal reduction in ICU length of stay for those who die, but it does not significantly improve all-cause mortality, surrogate mental health, or the quality of decision-making and communication. This finding challenges the common perception that shared decision-making yields broad benefits. Culturally adapted protocols and standardized implementation frameworks are essential to optimize shared decision-making’s role in high-stakes critical care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chen M Sepucha K Bozic KJ Jayakumar P. Value-based healthcare: integrating shared decision-making into clinical practice. Clin Orthop Relat Res. (2023) 481:448–50. doi: 10.1097/CORR.0000000000002580, 36735904 PMC 9928684 · doi ↗ · pubmed ↗
- 2Kawamoto E Ito-Masui A Esumi R Imai H Shimaoka M. How ICU patient severity affects communicative interactions between healthcare professionals: a study utilizing wearable sociometric badges. Front Med Lausanne. (2020) 7:606987. doi: 10.3389/fmed.2020.606987, 33344484 PMC 7744931 · doi ↗ · pubmed ↗
- 3Goostrey K Muehlschlegel S. Prognostication and shared decision making in neurocritical care. BMJ. (2022) 377:e 060154. doi: 10.1136/bmj-2021-060154, 35696329 · doi ↗ · pubmed ↗
- 4Stalnikowicz R Brezis M. Meaningful shared decision-making: complex process demanding cognitive and emotional skills. J Eval Clin Pract. (2020) 26:431–8. doi: 10.1111/jep.13349, 31989727 · doi ↗ · pubmed ↗
- 5Baik D Cho H Masterson Creber RM. Examining interventions designed to support shared decision making and subsequent patient outcomes in palliative care: a systematic review of the literature. Am J Hospice Palliat Care. (2019) 36:76–88. doi: 10.1177/1049909118783688, 29925244 PMC 6056336 · doi ↗ · pubmed ↗
- 6Vidal E I de O Kovacs M J Silva J Jda Silva L. M. d. Sacardo D. P. Bersani A. L. d. F. . Position statement of ANCP and SBGG on shared decision-making in palliative care Cad Saude Publica 2022 38:e 00130022. doi: 10.1590/0102-311xen 130022, 36169516 · doi ↗ · pubmed ↗
- 7Wendlandt B Olm-Shipman C Ceppe A Hough CL White DB Cox CE . Surrogates of patients with severe acute brain injury experience persistent anxiety and depression over the 6 months after ICU admission. J Pain Symptom Manag. (2022) 63:e 633–9. doi: 10.1016/j.jpainsymman.2022.02.336, 35595376 PMC 9179180 · doi ↗ · pubmed ↗
- 8Wendlandt B Ceppe A Cox CE Hanson LC Nelson JE Carson SS. The association between patient health status and surrogate decision maker post-traumatic stress disorder symptoms in chronic critical illness. Ann Am Thorac Soc. (2021) 18:1868–75. doi: 10.1513/Annals ATS.202010-1300 OC 33794122 PMC 8641832 · doi ↗ · pubmed ↗