Symptomatic sinus bradycardia during the recovery phase of high-altitude pulmonary edema: a case report
Jiale Xie, Weiping Li, Jia Luan, Zhibiao Cai, Haijun Miao

TL;DR
A healthy man developed severe slow heart rate after recovering from high-altitude pulmonary edema, likely due to a rebound in vagal tone and steroid withdrawal.
Contribution
Highlights a novel clinical observation linking HAPE recovery with symptomatic sinus bradycardia due to vagal rebound and steroid withdrawal.
Findings
Symptomatic sinus bradycardia occurred during HAPE recovery with heart rate as low as 37 bpm.
Intravenous potassium and fluid resuscitation resolved the bradycardia, restoring heart rate to 59 bpm.
Rebound vagal tone and steroid withdrawal are suggested as contributing factors to the bradycardia.
Abstract
This case report describes a 28-year-old healthy male who developed high-altitude pulmonary edema (HAPE) after a rapid ascent. While his condition improved with standard therapy (including corticosteroids, diuretics, and supplemental oxygen), he developed symptomatic sinus bradycardia (heart rate nadir: 37 bpm) 2 days after discontinuation of these medications. The bradycardia resolved with intravenous potassium supplementation and fluid resuscitation, and his heart rate recovered to 59 bpm. This case highlights that a rebound in vagal tone and steroid withdrawal may contribute to severe bradycardia during the HAPE recovery phase, warranting heightened clinical vigilance.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
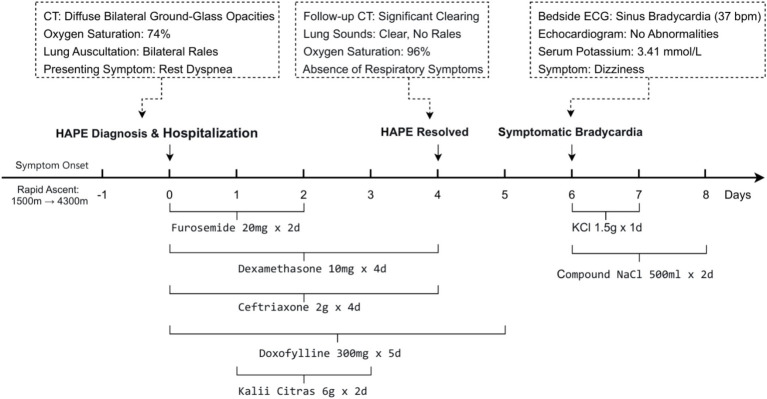 Figure 1
Figure 1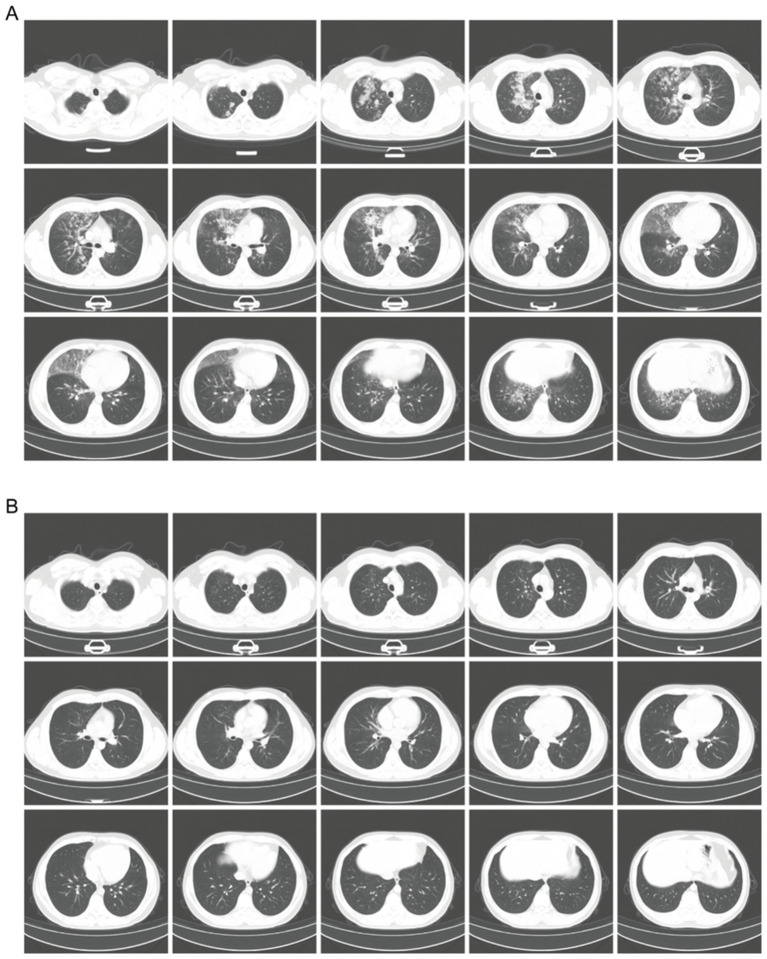 Figure 2
Figure 2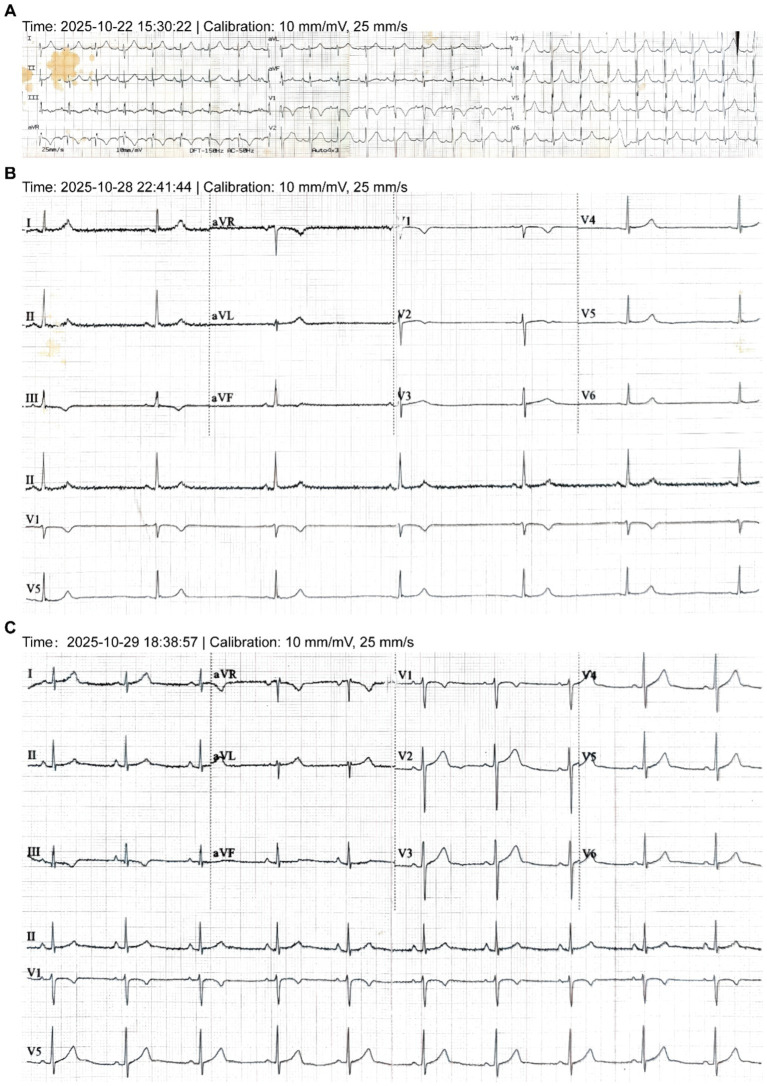 Figure 3
Figure 3| Clinical parameters | On admission (day 0) | Upon HAPE resolution (day 4) | Onset of symptomatic bradycardia (day 6) | After bradycardia resolution (day 7) |
|---|---|---|---|---|
| Symptoms | Cough | Resolution of respiratory symptoms | Dizziness | Asymptomatic |
| Physical signs | Bilateral wet rales | No significant rales | HR: 35–40 bpm | HR: 60–65 bpm |
| Oxygen saturation (%) | 74% | 96% | 95% | 97% |
| Heart rate (bpm) | 96 | 70 | 37 | 59 |
| Blood pressure (mmHg) | 98/77 | 100/60 | 117/78 | 108/62 |
| Serum potassium (mmol/L) | 3.81 | – | 3.41 | 4.81 |
| Serum magnesium (mmol/L) | 1.10 | – | 1.20 | 1.11 |
- —Gansu Provincial Natural Science Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHigh Altitude and Hypoxia · Cardiovascular Syncope and Autonomic Disorders · Restraint-Related Deaths
Introduction
HAPE is a well-known acute complication of rapid ascent, characterized by hypoxic pulmonary vasoconstriction and non-cardiogenic edema. While its acute management is standardized, the recovery phase is less well-characterized and is often assumed to be uneventful. We report a unique case of a healthy male who developed severe, symptomatic sinus bradycardia during recovery from successfully treated HAPE. This dramatic shift from initial tachycardia to a heart rate of 37 bpm occurred after discontinuing corticosteroids and diuretics, highlighting the recovery period as a potential window of vulnerability for autonomic dysfunction and serious arrhythmias. This case underscores the need for sustained vigilance beyond the resolution of pulmonary symptoms.
Case presentation: from HAPE to unexpected bradycardia
A 28-year-old male with no significant past medical history presented to our temporary high-altitude medical station due to severe dyspnea. He had ascended rapidly by air from 1,500 meters to 4,300 meters for work. Shortly after arrival, he reported a worsening cough and shortness of breath, which progressed to dyspnea at rest by the following day (Figure 1).
- Initial Presentation and Diagnosis of HAPE: Upon admission (Day 0), the patient was in severe respiratory distress. Vital signs revealed critical hypoxemia with an oxygen saturation of 74%, tachycardia (96 bpm), and a blood pressure of 98/77 mmHg. Physical examination confirmed bilateral pulmonary rales. Laboratory studies were significant for leukocytosis (12.0 × 10^9^/L) and serum potassium (3.81 mmol/L). A chest CT scan revealed bilateral patchy infiltrates, which were characteristic of acute high-altitude pulmonary edema (HAPE, Figure 2A), thereby confirming the diagnosis.
- Successful Treatment and Initial Recovery: The patient was initiated on a standard HAPE treatment protocol, which included intravenous furosemide (20 mg daily for 2 days), dexamethasone (10 mg daily for 4 days), and doxofylline (300 mg daily for 5 days), along with oral potassium citrate (2 g three times daily for 2 days, total 12 g) and prophylactic antibiotics. Following this regimen, his clinical condition improved markedly. A follow-up chest CT on Day 4 demonstrated near-complete resolution of the pulmonary edema (Figure 2B), and discharge was planned.
- Unexpected Clinical Deterioration: Symptomatic Bradycardia: On the second day after the discontinuation of diuretics and corticosteroids (Hospital Day 6), the patient developed a new-onset headache and was found to have profound symptomatic sinus bradycardia with a heart rate of 37 bpm (Figure 3B). This represented a dramatic shift from his initial presentation tachycardia (96 bpm) (Figure 3A). The evolution of these key signs and objective findings across critical time points is summarized in Table 1.
Clinical timeline from HAPE to symptomatic bradycardia and recovery.
Comparative chest CT imaging before and after treatment for HAPE. (A) Admission CT (day 0) reveals extensive bilateral ground-glass opacities with a peri-hilar and peripheral predominance, accompanied by coarse pulmonary markings, reticulations, and areas of traction bronchiectasis, consistent with diffuse interstitial involvement and highly suggestive of HAPE. (B) Post-treatment CT (day 4) reveals significant clearing of the infiltrates, illustrating the rapid radiological response to therapy.
Evolution of electrocardiographic findings. (A) Sinus tachycardia (96 bpm) recorded at admission. (B) Symptomatic sinus bradycardia (37 bpm) captured on Day 6. (C) Restoration of sinus rhythm (59 bpm) following therapeutic intervention. All tracings are shown at the standard calibration of 10 mm/mV and 25 mm/s.
Final diagnoses
- Acute Phase: High-altitude pulmonary edema.
- Recovery Phase: Symptomatic sinus bradycardia.
Assessment and exclusion of secondary causes
Upon the emergence of bradycardia, a focused evaluation was conducted to rule out common secondary causes. A detailed medication and exposure history revealed no use of bradycardia-inducing agents in the preceding month except for ibuprofen prior to admission. Following descent, comprehensive evaluation at a tertiary center was performed. A 24 h Holter monitor documented a minimum heart rate of 31 bpm, a 24 h average heart rate of 55 bpm, and a longest R-R interval of 2.078 s, with no other significant arrhythmias. Thyroid function tests and cardiac biomarkers were within normal limits. These objective findings support the diagnosis of a transient, context-driven autonomic dysfunction.
Management and outcome of bradycardia
Management shifted abruptly from HAPE to the life-threatening bradycardia. The patient was placed on continuous cardiac monitoring and supplemental oxygen. He received intravenous potassium chloride (1.5 g) via an infusion pump, diluted in 500 mL of normal saline (final concentration ≈ 0.3%), at a controlled rate of approximately 5 mL/min, along with intravenous fluid resuscitation using compound sodium chloride injection (500 mL daily for 2 days). A comprehensive panel of serum electrolytes was obtained approximately 12 h after initiating this intravenous potassium therapy. His heart rate recovered to a stable range of 50–67 bpm within 24–48 h (Figure 3C).
Follow-up and outcomes
Subsequent follow-up revealed no recurrence of cardiac symptoms. A 24 h Holter monitor performed at a tertiary center showed no significant arrhythmias, confirming the transient nature of the event. Two weeks after discharge, a telephone follow-up confirmed that the patient remained asymptomatic, with self-reported heart rates ranging from 65 to 110 bpm during daily activities, further supporting a full and sustained recovery.
Discussion
During the acute phase of HAPE, severe hypoxia and stress lead to extreme sympathetic activation, resulting in compensatory tachycardia (1, 2). The profound hypoxia triggers intense pulmonary vasoconstriction, significantly increasing pulmonary vascular resistance and right ventricular afterload. Upon rapid correction of hypoxia and pulmonary edema with effective treatment, the abrupt withdrawal of sympathetic tone, particularly after furosemide cessation and stabilization of volume status, may lead to a relative predominance of vagal tone (3, 4). Concomitantly, the rapid resolution of hypoxia leads to a sudden decrease in pulmonary vascular resistance and right ventricular load. This acute shift in cardiopulmonary hemodynamics may further perturb the autonomic balance, potentially via cardiopulmonary baroreceptor mechanisms, and contribute to the depression of sinoatrial node automaticity. This can profoundly depress the automaticity of the sinoatrial node, causing a sharp decrease in heart rate. In our patient, the heart rate was 96 bpm at admission during the acute HAPE phase. The symptomatic bradycardia occurred on day 6, during the recovery phase after discontinuing primary medications. This temporal pattern strongly supports the hypothesis of autonomic rebound as a primary mechanism.
Corticosteroid-induced bradycardia has been previously documented. For instance, Alvin Oliver Payus et al. (5) reported a case of severe sinus bradycardia in a patient with lupus nephritis following high-dose IV hydrocortisone. Similarly, Mohammed Ahmed et al. (6) described bradycardia in a Crohn’s disease patient after hydrocortisone administration. Our patient received 10 mg of dexamethasone daily for 4 days. Unlike previous reports, bradycardia occurred 2 days after discontinuation. We postulate that short-term, high-dose exogenous glucocorticoids may have transiently suppressed the hypothalamic–pituitary–adrenal (HPA) axis. The subsequent withdrawal led to a state of relative endogenous cortisol insufficiency. Given cortisol’s role in maintaining vascular tone and potentiating catecholaminergic effects, its abrupt decline may have reduced basal sympathetic tone and vascular responsiveness, synergizing with vagal rebound to promote bradycardia. It must be acknowledged, however, that serum cortisol levels were not measured in our patient during the bradycardic episode, which limits the direct biochemical confirmation of this hypothesis.
Hypokalemia significantly affects myocardial excitability. While mild hypokalemia often presents with tachycardia, severe depletion can depress automaticity (7). The mechanism involves altered myocardial membrane potentials, reducing the rate and amplitude of phase 0 depolarization, which can decrease the excitability of sinoatrial pacemaker cells (8). Our patient’s serum potassium dropped from 3.81 mmol/L on admission to 3.41 mmol/L on the day of the bradycardic event, despite oral potassium supplementation. This significant hypokalemia likely exacerbated the bradycardia by further depressing SA node function in the setting of already elevated vagal tone.
This case underscores that the recovery phase from HAPE constitutes a vulnerable window for profound autonomic instability, during which severe bradycardia can occur. This paradoxical shift from near-universal acute-phase tachycardia to profound bradycardia upon recovery suggests a critical and under-recognized transition period. The pathophysiology likely involves a triad of extrinsic, reversible factors acting in concert: abrupt sympathetic withdrawal following rapid hypoxia correction, relative endogenous cortisol insufficiency after exogenous steroid cessation, and hypokalemia. The concurrent precipitous drop in pulmonary vascular resistance after HAPE resolution may further perturb cardiopulmonary coupling and baroreceptor feedback, favoring vagal predominance. Although no identical cases are reported, this multifactorial mechanism aligns with reversible sinoatrial node dysfunction seen in other critical illnesses. Consequently, in resource-limited high-altitude settings, clinical vigilance must extend well beyond the resolution of pulmonary symptoms. Close monitoring of heart rate, blood pressure, and electrolytes remains crucial even after primary medications are discontinued and imaging shows significant improvement.
Patient perspective
The patient reported having minimal prior understanding of high-altitude pathology. He described the sequential onset of severe dyspnea followed by acute dizziness during recovery as a profoundly alarming experience. He expressed sincere appreciation for the coordinated care provided under resource-limited conditions. This episode has fundamentally altered his risk perception regarding high-altitude travel.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rani R Kutum R Punera DS Yadav AP Bansal V Prasher B. Physiological, biochemical, and genome-wide expression patterns during graded normobaric hypoxia in healthy individuals. Physiol Genomics. (2025) 57:49–64. doi: 10.1152/physiolgenomics.00056.2024, 39716895 · doi ↗ · pubmed ↗
- 2Mi YM Hu WL Chao HM Hua CZ Chen ZM. Pediatric high-altitude pulmonary edema and acute mountain sickness: clinical features and risk determinants. Pediatr Pulmonol. (2024) 59:2614–20. doi: 10.1002/ppul.27101, 38837645 · doi ↗ · pubmed ↗
- 3Aksu T Brignole M Calo L Debruyne P Di Biase L Deharo JC . Cardioneuroablation for the treatment of reflex syncope and functional bradyarrhythmias: a scientific statement of the European heart rhythm association (EHRA) of the ESC, the Heart Rhythm Society (HRS), the Asia Pacific Heart Rhythm Society (APHRS) and the Latin American Heart Rhythm Society (LAHRS). Europace. (2024) 26:euae 206. doi: 10.1093/europace/euae 206, 39082698 PMC 11350289 · doi ↗ · pubmed ↗
- 4Aggarwal K Pathan MS Dhalani M Kaur IP Anamika F Gupta V . Elevated perspectives: unraveling cardiovascular dynamics in high-altitude realms. Curr Cardiol Rev. (2025) 21:e 1573403 X 308818. doi: 10.2174/011573403 X 308818241030051249, 39506447 PMC 12060922 · doi ↗ · pubmed ↗
- 5Payus AO Chai AC Mustafa N. An uncommon side effect of a very commonly used medication: a case report on hydrocortisone-induced bradycardia. Clin Case Rep. (2021) 9:e 04678. doi: 10.1002/ccr 3.4678, 34430027 PMC 8365536 · doi ↗ · pubmed ↗
- 6Ahmed M Oyibo ST Dalvi S Cowell R. Hydrocortisone-induced symptomatic sinus bradycardia. BMJ Case Rep. (2022) 15:e 252878. doi: 10.1136/bcr-2022-252878, 36375852 PMC 9664291 · doi ↗ · pubmed ↗
- 7Whittaker DG Colman MA Ni H Hancox JC Zhang H. Human atrial Arrhythmogenesis and sinus bradycardia in KCNQ 1-linked short QT syndrome: insights from computational modelling. Front Physiol. (2018) 9:1402. doi: 10.3389/fphys.2018.01402, 30337886 PMC 6180159 · doi ↗ · pubmed ↗
- 8Turner D Kang C Mesirca P Hong J Mangoni ME Glukhov AV . Electrophysiological and molecular mechanisms of sinoatrial node Mechanosensitivity. Front Cardiovasc Med. (2021) 8:662410. doi: 10.3389/fcvm.2021.662410, 34434970 PMC 8382116 · doi ↗ · pubmed ↗