Case Report: Challenges in the surgical treatment of Marfan-associated aortic aneurysms: a literature review starting from a clinical case
Ombretta Martinelli, Antonio Marzano, Valeria Gonta, Lucio Ferriero, Carola D’Amico, Simone Cuozzo, Maria Irene Bellini

TL;DR
A 55-year-old woman with Marfan syndrome underwent multiple surgeries for aortic aneurysms, leading to a literature review on treatment challenges and strategies.
Contribution
Presents a complex clinical case and literature review on surgical approaches for Marfan-associated aortic aneurysms.
Findings
Combining relining and CT stenting successfully managed a complex aortic aneurysm with endoleaks.
The patient showed no postoperative complications and had favorable 12-month follow-up results.
The case highlights the need for durable, combined surgical strategies in young MFS patients with aortopathy.
Abstract
Marfan syndrome (MFS) is a systemic connective tissue disease severely affecting the cardiovascular system. We present the case of a MFS 55-year-old woman who arrived at the emergency department with increasing chest pain. Over the past 25 years, this patient had undergone mitral valve annuloplasty, subsequent open surgical repair of a ruptured infrarenal abdominal aortic aneurysm followed by open surgery for a type I thoracoabdominal aortic aneurysm. She was also operated for fenestrated endovascular repair of a visceral aortic aneurysm using a ‘graft-to-graft’ approach. Upon the urgent admission, a multislice computed tomography angiography demonstrated an aortic aneurysm sac with a maximum diameter of 11.8 cm that was fed by a type IIIB endoleak, due to complete branch stent disconnection of the right renal artery (RRA) and by type IIIB/IIIC endoleaks secondary to stent fracture and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
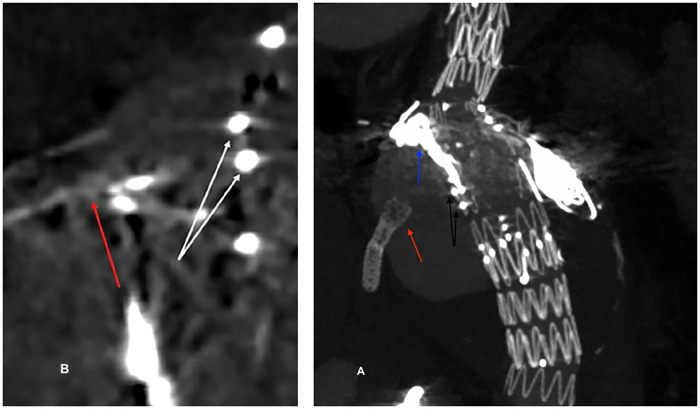 Figure 1
Figure 1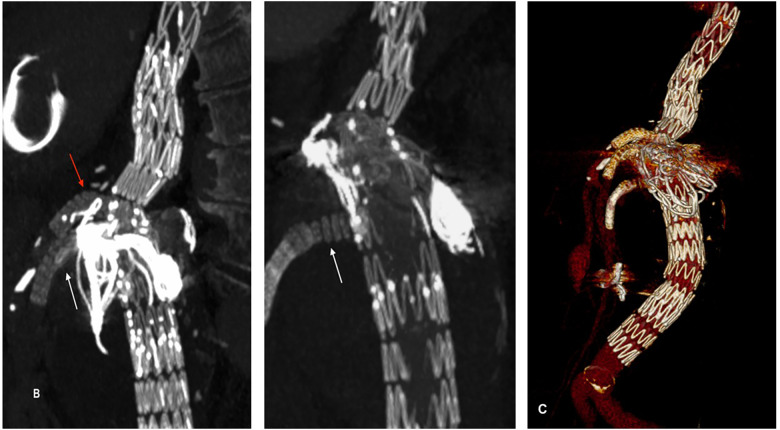 Figure 2
Figure 2| Study | Patients ( | Median follow-up, months | Endograft-related complications % | Reintervention in same aortic segment (Open) % | Reintervention in same aortic segment (Endovascular) % |
|---|---|---|---|---|---|
| Waterman et al. ( | 16 | 9.3 | 30 | 33 | 13 |
| Pacini et al. ( | 50 | 24 | 16 | 14 | 16 |
| Glebova et al. ( | 216 | 9.3–162 | 44 | 50 | 36 |
| Preventza et al. ( | 60 | 28 | 17 | 7 | 12 |
| Olsson et al. ( | 171 | 56.4 | Not specified | 39.8 | 8.2 |
| Conway et al. ( | 29 | 25.5 | 13.7 | 3.4 | 6.9 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAortic Disease and Treatment Approaches · Connective tissue disorders research · Aortic aneurysm repair treatments
Introduction
The Marfan syndrome (MFS) is one of the most common single-gene malformation syndrome predominantly due to fibrillin 1 gene (FBN1) mutations leading to the increase of TGF-beta and subsequent activation of matrix metalloproteinases (MMPs), particularly MMP-2 and MMP-9, cytokines, chemokines, prostaglandin derivatives (1), as well as affecting BMP signalling. These alterations cause elastin and collagen destruction which compromise the structural and functional integrity of all connective tissues, predisposing cardiac damages, among which mitral and tricuspid valve prolapse, cardiomyopathy, and dilatation of the aortic root (2). Moreover, there is extensive mitochondrial dysfunction, as a direct consequence of reduced FBN1 extracellular matrix, which exhausts the vascular cells. This connective disease also leads to progressive aortic dilatation and dissections which are important causes of decreased life expectancy, requiring treatment (3, 4).
Yet, the systemic nature of connective tissue weakening and the unpredictable progression of Marfan-associated aortic damages make their management challenging with a high risk of complications.
We report a case of MFS, which is extraordinary for the sequential dilation of different aortic segments in a single patient necessitating an increasingly complex management, not free from complications. We used such a complex case as a reference for literature review on current trends and perspectives in the treatment of aortic pathology related to MFS.
Case
A 55-year-old woman was admitted to our Emergency Department complaining of chest pain. The patient's medical history included MFS, arterial hypertension, obesity (class II, BMI 37,1 kg/m^2^), and laparocele with a hostile abdomen.
Due to her connective tissue disorder, over the past 25 years, the patient had undergone multiple cardiovascular surgeries carried out in various hospital centres.
The patient underwent mitral valve annuloplasty with a Carpentier-Edwards ring to treat major mitral valve prolapse at the age of 29 years. In 2001 she underwent open surgical repair via median laparotomy for a ruptured infrarenal abdominal aortic aneurysm (AAA) followed by open surgery via thoraco-phreno-laparotomy for a type I thoracoabdominal aortic aneurysm (TAAA) in 2003. In 2015, due to the subsequent development of a suprarenal abdominal aortic aneurysm, she was submitted to a fenestrated endovascular repair (FEVAR) using a ‘graft-to-graft’ approach with a custom-made stent-graft (Cook Medical Inc., Bloomington, IN, USA). At the time of the suprarenal aortic dilatation, endovascular intervention was justified regardless of long-term stability of the repair due to the patient's high operative risk and difficulties of a new open surgical approach.
The computed tomography angiography (CTA) carried out on emergency admission (Figure 1) showed a type IIIB endoleak caused by a complete stent disconnection of the right renal artery (RRA) and to a type IIIB/IIIC endoleak due to stent fracture and disconnection of the superior mesenteric artery (SMA); these endoleaks fed the aneurysm sac which had reached a maximum transverse diameter of 11.8 cm. On CTA, the bridging stent in the celiac trunk (CT) was not detected because of its absence or destruction; contemporarily, aneurysm of distal common hepatic artery, with a maximum transverse diameter of 2.29 cm, was also observed.
3D reconstruction of the preoperative CT scan. (A) Type IIIB endoleak due to a disconnection between the stent (red arrow) and the fenestration (black arrows) of the RRA. The coils within the aneurysmal sac are also visible (blue arrow). (B) Type IIIB/IIIC endoleak due to a disconnection and fracture between the stent (red arrow) and the fenestration (white arrows) of the SMA. RRA, right renal artery; SMA, superior mesenteric artery.
Under general anaesthesia and through bilateral percutaneous femoral access with a 16 F steerable catheter sheath (Aptus HeliFX, Medtronic, Minneapolis, USA) a relining of the RAA and of the SMA was performed with Ballon-expandable Gore Viabahn and VBX stent-grafts (W.L. Gore & Associates, Flagstaff, AZ, USA). Subsequently, CT stenting was successfully carried out. The bridging stents were intentionally positioned to protrude into the fenestrations, in order to ensure also sufficient overlap with the previously placed stent at the target vessel level.
There were no systemic complications during or after the procedure and the patient was discharged after 3 days under dual anti-platelet therapy. Duplex ultrasounds performed at 1, 3, 6 and 12 months and CTA performed in the first month and at 12 months of follow-up demonstrated the complete exclusion and shrinkage of the aneurysmal sac and the patency of the stented visceral and renal vessels (Figure 2). Consent was obtained from the patient for publication of the case report.
3D reconstructions of the 12-month CTA showing correct positioning and patency of the stents in the RRA, SMA, and CT, with no evidence of endoleaks. (A) relining of the RRA stent (white arrow). (B) relining of the SMA stent (white arrow) and placement of the stent in the CT (red arrow). (C) volume rendering. CT, celiac trunk; SMA, superior mesenteric artery; RRA, right renal artery.
Discussion
MFS is a serious chronic disorder involving multiple organ systems with no cure at present. In patients with MFS, FBN1 gene mutation leads to a structural weakness of connective tissue due to the elastin and collagen destruction, and predisposes to aortic root aneurysm and aortic aneurysm and dissection (5–7).
Life-threatening heart valve complications requiring replacement often occur at a younger age in MFS patients, compared to other degenerative aortic disease and involving the thoracic aorta, more frequently than abdominal aorta (8, 9).
Since, medical therapy of MFS with beta-blockers and type 1 angiotensin II receptor blockers can slow down aortic aneurysm progression but could not completely arrest aneurysmal growth, aortic surgery is still the only treatment to prevent aneurysmatic rupture (10, 11).
Therefore, MFS patient survival is closely related with the severity of aortic involvement and the timeliness of its diagnosis and treatment (12). Although true isolated abdominal aortic aneurysms (AAA) represent only 3% of initial aortic disease in MFS, this atypical manifestation of MFS must be carefully considered as early diagnosis and timely intervention influence long-term prognosis (13). The case presented herein is emblematic for the early onset and the possible atypical pattern of cardiovascular diseases in MFS patients: the patient required mitral valve surgery at 29 years and emergency open repair of a ruptured infrarenal AAA at the age of 31.
The fragility of the aortic wall and the young age of these patients with the inherent lifelong propensity toward progressive aortic dilation and dissection make repair selection particularly challenging (14). It is well known in fact that MFS patients continue to experience aortic degeneration throughout their lives and often require several sequential aortic surgical procedures (15). Consistently with the exceptional course of the disease, two years after infrarenal AAA replacement surgery, this patient had a type I TAAA and 12 years later she experienced a further progression of her aortic pathology, leading to dilatation of the remnant segment of the descending aorta. Both the ruptured AAA and subsequent type I TAAA were treated with open repair.
Although endovascular repair has become standard for many degenerative aneurysms due to lower early morbidity and mortality (16–18), it remains a controversial option in connective tissue disorders (19, 20). In MFS, open surgical repair remains the recommended treatment for aortic aneurysms, including thoracoabdominal aortic aneurysm, given the possibility to remove diseased tissue, thus providing the most durable long-term protection (21).
Highly satisfactory outcomes with open repair of aortic disease in MFS patients have been reported by several surgical centers (21, 22); in particular, Coselli et al. reported on the excellent survival and low re-operation rates after open surgery in connective tissue disorders, including MFS up to 8 years after thoracoabdominal aortic open repair (23).
A further consideration in favor of open surgery is younger age of MFS patients, in comparison to the general aortic diseases population. These patients usually have low operative risk, but the longest durability of the repair is crucial, given the life-expectancy.
The current propensity for open surgery also derives from the potential impact of persistent radial forces of a stent graft on a weak and progressively dilating aorta with subsequent risk of stent displacement, complications and need for open conversion repair (24).
Notwithstanding, the rapid technology evolution and improvement of the results in the endovascular treatment of aortic pathology have led to a reconsideration of its use for MFS patients (25–27). Multiple reports have described high technical success, low early mortality and good short-term results of aortic endo-grafting in these patients (28, 29).
From a literature review by Harky et al. 81% of the endovascular procedures were technically successful with a 1.9% risk of death, 1.9% risk of stroke, <2% risk of spinal ischaemia, and 3.7% rate of conversion to open surgery (30).
However, long-term data regarding the endovascular approach in MFS patients show markedly higher rates of endoleaks, device failure, reintervention, and late conversion to open repair, in comparison to aortic degenerative disease (15, 31–35) (Table 1).
Given the highly satisfactory results with open surgical repair reported over the last decade by several experienced surgical centres, at present, there is no justification for elective endovascular stenting in patients with Marfan syndrome and type B dissection (36) or with aneurysm in the absence of dissection. For these reasons, guidelines from the European Society of Cardiology (ESC), European Association for Cardio-thoracic surgery (EACTS), American Heart Association (AHA), and American College of Cardiology (ACC) restrict endovascular repair in MFS population only as bridge to definitive open surgical therapy or for emergency procedures (37–39).
However, it should be considered that MFS patients previously treated with open aortic surgery may experience progression of their aortic pathology over time requiring further treatments. In 20% of cases, in fact they require intervention on non-aortic arterial segments from 5 to 6 years after the first aortic repair. Surgery then becomes particularly challenging in the context of multiple operations (40). An exception to guidelines recommendation is the situation in which an endograft can be anchored both proximally and distally to previously placed synthetic grafts. Several studies have reported successful outcomes after previous open repair of thoracic or thoracoabdominal aortic aneurysms where the stent grafts were anchored proximally and distally into the preexisting graft (41, 42). In this case the risk of stent graft-induced damages to the friable aortic wall can be avoided. In line with this concept in the present case, the fenestrated endograft was deployed between two existing surgical grafts and this ‘graft-to-graft’ approach effectively circumvented the risk of landing zone enlargement and distal migration (43). However, the long-term remodelling of the aorta and visceral vessels led to instability at the bridging stent interfaces, resulting in type III endoleaks. This occurrence, as observed in the present case, required urgent endovascular relining for late type IIIB endoleak and a type IIIC secondary to the disconnection of the bridging stents inserted in the RRA and SMA.
This highlights a crucial vulnerability of fenestrated and branched repair systems: the connection between the main graft and bridging stents is a frequent failure point, even more likely in patients with connective tissue disorders. Beyond progressive aortic dilatation, patients affected by MFS frequently develop aneurysmal degeneration of the visceral and iliac arteries (44, 45).
Reported series describe a high prevalence of branch vessel aneurysms, reaching up to 27%, together with a markedly increased incidence of iliac aneurysmal progression after AAA repair (8, 46).
Such vascular changes heighten the risk of branch-related failure and endoleaks and predispose to extra-aortic aneurysms as exemplified by this case, which was further complicated by a concomitant common hepatic artery aneurysm managed under active surveillance.
Although ongoing advances in endograft design may ultimately mitigate the frequency or possibly eliminate the complications associated with currently available devices, their safety and effectiveness have yet to be conclusively demonstrated (47, 48). In the absence of robust clinical evidence establishing long-term safety and durability, the routine use of endovascular stent grafts in patients with MFS cannot be recommended and should be reserved for highly selected cases. Additionally, it would be desirable to combine surgical or endovascular treatment with effective medical therapies aiming to slow down aortic growth. About this, the current evidence of pharmacological treatment for MFS patients is conflicting due to the lack of large trials (49). Beta-blockers, and angiotensin receptor blockers are the only available treatments to reduce aortic growth (49). Currently, doxycycline, is under consideration but its use is controversial due to the negative effect on mitochondria. These structures are in fact of crucial importance to aneurysm formation in MFS, in fact the distortion of the extracellular matrix-mitochondrial homeostasis axis intensifies aortic wall reorganisation, evolving into aneurysmatic sac (50). On the contrary, nicotinamide riboside, shows promise in aneurysm animal models by boosting mitochondrial function, improving vascular smooth muscle cell health, and reversing aortic dilation (51). The same beneficial effect might be observed with resveratrol, a dietary supplement interfering with cellular metabolism, as it stabilises the aortic growth rate in adult patients with MFS, according to a recent clinical trial (52). Finally, growing interest is also toward allopurinol, normally used against gout, as it is proven to hamper aortic aneurysm progression in MFS mice by its antioxidant mechanisms (53). Thus novel pharmacological therapies seem upcoming.
Conclusions
The present case highlights several practical frameworks for managing complex or redo aortic pathology in MFS patients: open surgery remains the first-line therapy for most elective aortic aneurysms and the routine use of endovascular stent grafts is not recommended.
However, endovascular aortic repair cannot be considered a prohibitive indication, but it should be reserved for selected cases such as primarily emergencies, high-risk reoperations, or surgically challenging cases as part of a multistage aortic repair with graft-to-graft landing zones following prior open aortic repairs.
Visceral and iliac arteries must be carefully monitored, as their progressive dilation predispose to extra-aortic aneurysms and can compromise endograft stability.
Although current medical therapy remains limited in its capacity to alter long-term disease progression, emerging treatments show preliminary promise to be validated in large clinical trials. Combining improved medical therapy with tailored open or endovascular strategies may ultimately enhance the durability of repairs in the MFS population.
These observations support the necessity for rigorous, lifelong imaging surveillance of disease progression for timely, anatomy-driven reinterventions, in order to ensure durable management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Asta L D'Angelo GA Marinelli D Benedetto U. Genetic basis, new diagnostic approaches, and updated therapeutic strategies of the syndromic aortic diseases: Marfan, loeys-dietz, and vascular ehlers-danlos syndrome. Int J Environ Res Public Health. (2023) 20(16). 10.3390/ijerph 2016661537623198 PMC 10454608 · doi ↗ · pubmed ↗
- 2Takeda N Yagi H Hara H Fujiwara T Fujita D Nawata K Pathophysiology and management of cardiovascular manifestations in Marfan and loeys-dietz syndromes. Int Heart J. (2016) 57(3):271–7. 10.1536/ihj.16-09427181042 · doi ↗ · pubmed ↗
- 3Vanem TT Geiran OR Krohg-Sørensen K Røe C Paus B Rand-Hendriksen S. Survival, causes of death, and cardiovascular events in patients with Marfan syndrome. Mol Genet Genomic Med. (2018) 6(6):1114–23. 10.1002/mgg 3.48930393980 PMC 6305663 · doi ↗ · pubmed ↗
- 4Groth KA Stochholm K Hove H Andersen NH Gravholt CH. Causes of mortality in the Marfan syndrome(from a nationwide register study). Am J Cardiol. (2018) 122(7):1231–5. 10.1016/j.amjcard.2018.06.03430149886 · doi ↗ · pubmed ↗
- 5Milleron O Arnoult F Delorme G Detaint D Pellenc Q Raffoul R Pathogenic FBN 1 genetic variation and aortic dissection in patients with Marfan syndrome. J Am Coll Cardiol. (2020) 75(8):843–53. 10.1016/j.jacc.2019.12.04332130918 · doi ↗ · pubmed ↗
- 6den Hartog AW Franken R Zwinderman AH Timmermans J Scholte AJ van den Berg MP The risk for type B aortic dissection in Marfan syndrome. J Am Coll Cardiol. (2015) 65(3):246–54. 10.1016/j.jacc.2014.10.05025614422 · doi ↗ · pubmed ↗
- 7de Beaufort HWL Trimarchi S Korach A Di Eusanio M Gilon D Montgomery DG Aortic dissection in patients with Marfan syndrome based on the IRAD data. Ann Cardiothorac Surg. (2017) 6(6):633–41. 10.21037/acs.2017.10.0329270375 PMC 5721116 · doi ↗ · pubmed ↗
- 8Schoenhoff FS Yildiz M Langhammer B Jungi S Wyss TR Makaloski V The fate of nonaortic arterial segments in Marfan patients. J Thorac Cardiovasc Surg. (2019) 157(6):2150–6. 10.1016/j.jtcvs.2018.10.08930578062 · doi ↗ · pubmed ↗