Promises and challenges of AI-enabled methods for myocardial characterisation in cardiovascular magnetic resonance
N. McWilliams, M. Varela, G. Joy

TL;DR
This paper reviews how AI can improve heart disease diagnosis using magnetic resonance imaging, but faces challenges like data access and regulatory approval.
Contribution
The paper provides a comprehensive overview of AI applications in CMR tissue characterization and identifies barriers to clinical adoption.
Findings
AI improves motion correction and image reconstruction in CMR.
AI enables contrast-free scar characterization using native CMR signals.
AI can derive high-dimensional tissue phenotypes beyond expert analysis.
Abstract
Cardiac magnetic resonance (CMR) tissue characterisation is central to the diagnosis and risk stratification of myocardial disease. However, for certain techniques tissue characterisation CMR is limited by reliance on contrast agents, sensitivity to motion, prolonged acquisition times, and time- and labour-intensive image reconstruction and analysis. Artificial intelligence (AI) has emerged as a promising approach to address these challenges by enhancing and accelerating multiple stages of the CMR workflow. Deep learning methods can automate LGE segmentation, improve motion correction and image reconstruction for parametric mapping, and enable contrast-free characterisation of scar by exploiting native CMR signals, including myocardial motion and native T1 mapping. AI has also accelerated emerging techniques such as cardiac magnetic resonance fingerprinting and diffusion tensor imaging.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2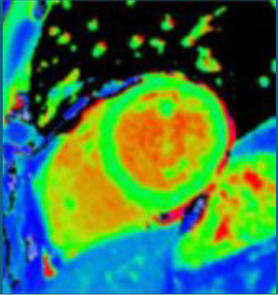 Figure 3
Figure 3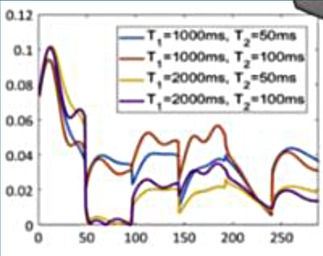 Figure 4
Figure 4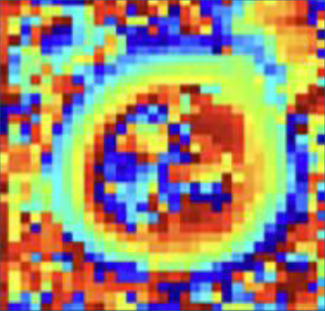 Figure 5
Figure 5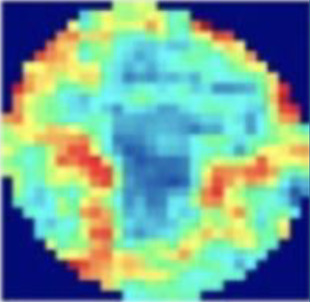 Figure 6
Figure 6| Domain | AI techniques | CMR applications | Key advantages and challenges |
|---|---|---|---|
| Late gadolinium enhancement segmentation | Convolutional Neural Networks (CNNs) |
Automated scar segmentation (ischaemic & non-ischaemic) scar burden quantification in hypertrophic cardiomyopathy (HCM) and ischaemic cardiomyopathy (ICM) |
AI LGE segmentation Reduce inter-/ intra-observer variability Enables rapid analysis at scale Limited by a lack of standardized ground truth & large scale external validation |
|
| Fully Convolutional Networks (FCNs) | ||
| Long Short-Term Memory Recurrent Neural Networks (LSTM-RNNs) | |||
| Autoencoders | |||
| Gradient weighted Class activation mapping (GradCAM) interpretability/weak-supervision method | |||
| Vision Foundation Models self-supervised large-scale pretraining | |||
| Synthetic Post-contrast Imaging | Generative Adversarial Networks (GANs) |
Contrast-free detection of focal fibrosis in HCM, myocardial infarction (MI) | Virtual LGE |
|
|
Virtual Native Enhancement (VNE) Cine-Generated Enhancement (CGE) |
Improves accessibility (renal failure, allergy) only in proof-of-concept stage Needs validation in multiple diseases, scanners, sequences and externally on diverse clinical datasets | |
| Recurrent neural networks long-short term memory | |||
| Parametric Mapping (T1/T2/T2*/ECV) | CNN-based motion correction (MOCO) | -Motion correction in mapping acquisitions | AI MOCO and reconstruction |
|
| End-to-end DL reconstruction frameworks |
Rapid 3D whole-heart T1/T2 mapping Artefact suppression Virtual ECV mapping from native T1 input |
Improves reproducibility & quantitative accuracy and reduces reconstruction times Needs to be applied in-line across scanners and vendors for widescale adoption |
| Generative Adversarial Networks | vECV | ||
|
Proof-of concept stage but current risks include missing of focal mapping lesions and GAN based hallucinations | |||
| Cardiac Magnetic Resonance Fingerprinting | Neural networks for dictionary-free reconstruction |
Simultaneous acquisition of T1/T2 mapping Potential to map other tissue characteristics (e.g., perfusion/scar) | cMRF: |
|
|
Single acquisition for multiple tissue characteristics Robustness against cardiac rhythms Potential for standardization across scanner vendors. Only in proof-of-concept stage | ||
| Diffusion Tensor Cardiac MRI | Accelerated acquisition through CNN based denoising and diffusion-tensor quantification from undersampled data (reduced averaging/repetitions required) |
Contrast-free detection of microstructural alteration (e.g., subclinical HCM, post-MI remodelling) | AI denoising and reconstruction |
|
|
Overcomes intrinsic low signal-to-noise ratio (SNR) encountered by the technique Improves acquisition speed and therefore clinical translation | ||
| Radiomics and Deep-learning feature extraction | Unsupervised ML methods (clustering, principal component analysis, support vector machines) |
Disease discrimination [e.g., HCM vs. hypertension (HTN)] Risk stratification Detection of subtle tissue changes [e.g., chronic inflammation in dilated cardiomyopathy (DCM)] Texture analysis-based contrast-free rule-out of LGE Integration with phenome wide-associations in large-scale population studies | Radiomics |
|
|
Conventional CMR can be used—no additional acquisition required Challenge: domain shift caused by influence of scanner type, vendor and sequence parameters in training Larger prospective studies are needed | ||
|
Vision neural networks | |||
|
Lack of large labelled datasets for training and validation |
| Study | Aims | Methods | Main findings |
|---|---|---|---|
| Late Gadolinium enhancement segmentation | |||
| Fahmy et al. ( |
Develop and evaluate performance of automated LGE segmentation in patients with HCM |
3D CNN Train Multi-site, multi-vendor Stratified internal validation Compared to manual quantification & 2D CNN |
Rapid acquisition (0.15s per image) Good agreement with manual LGE quantification Outperformed 2D CNN for agreement with manual LGE |
| Ghanbari et al. ( |
Develop and evaluate automated LGE segmentation in patients with IHD |
FCN Train Internal validation Compared to manual quantification |
Good agreement with manual LGE quantification Outperformed clinicians in predicting arrhythmic events |
| Moccia et al. ( |
Test feasibility of automated LGE segmentation of infarcts Compare whole LGE images vs. LV only input |
FCN Train/test Internal validation Compared to manual quantification |
Feasible for LGE detection Limiting search area to LV improved performance |
| Cui et al. ( |
Perform unsupervised LGE segmentation by leveraging labelled cine images through domain adaptation |
Train a cine-labelled segmentation network and adapt it to LGE by aligning their image features using a variational autoencoder-based unsupervised domain adaptation framework |
Technique improved unsupervised LGE segmentation Outperformed existing methods tested across public datasets |
| Lalande et al. ( |
eMEDIC challenge results described |
A contest where several CNNs evaluated for discrimination between LGE images with & without infarct & extent of infarct |
CNN accurately discriminates infarct from non-infarct Segmentation of areas of infarct remains challenging |
| Jacob et al. ( |
Perform scar burden quantification for detecting myocardial pathologies (normal, dilated, hypertrophic, ischaemic) |
Foundational model pre-trained on millions of unlabelled images DL method, train external validation |
Scar segmentation model trained without labelling is feasible Clinically valuable |
| Parametric mapping and synthetic post-contrast imaging | |||
| Zhang et al. ( |
In patients with HCM Generate LGE-like scar images from non-contrast images (native T1 maps + cines), termed virtual native enhancement (VNE) |
Conditional generative adversarial network: Train internal validation Blinded assessors graded the image quality of LGE and VNE and quantified both using standard techniques |
VNE images had better quality than LGE images. VNE scar had good visuospatial and quantitative agreement with LGE |
| Zhang et al. ( |
In patients with chronic MI Generate LGE-like scar images from non-contrast images (native T1 maps + cines), termed virtual native enhancement |
Conditional generative adversarial network: Train internal validation Blinded assessors graded the image quality of LGE and VNE and quantified both using standard techniques |
VNE: 84% accuracy in detecting MI (LGE ground truth), 100% specificity Better image quality than LGE Good agreement in infarct quantification and transmurality Validated in porcine models |
| Qi et al. ( |
In patients with acute MI Generate and evaluate LGE-like scar images from cine images (CGE-cine-generated enhancement) |
Generative adversarial network Train CGE images were compared with LGE for quality using blinded observers and scar quantification (CGE/LGE using standard manual techniques) |
CGE: Superior image quality to LGE Accurate scar quantification compared to LGE ground truth |
| Xu et al. ( |
In patients with suspected MI Detect MI from non-contrast cine MRI by learning abnormal motion patterns |
DL combined LV-focused ROI cropping Local spatiotemporal (LSTM) and global optical-flow motion features Train/test LGE-segmented infarct as the gold standard provided by two expert radiologists. |
Good accuracy compared to manual ground truth |
| Gonzales et al. ( |
Motion artefact correction in native T1 maps |
DL-MOCO CNN Train Internal validation. DL MOCO compared to standard image registration |
Fast (<1s per T1 map) Suppressed a wide range of motion artefacts Better MOCO compared to traditional methods. |
| Felsner et al. ( |
To assess an end-to-end DL algorithm to accelerate free-breathing 3D whole heart joint T1/T2 mapping. |
Non-rigid motion-corrected reconstruction network was used to estimate reconstructions of highly undersampled data Train |
Highly accelerated MOCO reconstruction (370x) Good agreement with reference standard (HDPROST) |
| Nowak et al. ( |
Generate contrast-free virtual ECV (vECV) from native T1 maps to discriminate disease (myocarditis/amyloidosis) from health |
GAN Train External validation vECV was compared against true ECV values and assessed for diagnostic performance in myocarditis and amyloidosis |
vECV: good discrimination Strong agreement between quantification in vECV and true ECV in normal studies and myocarditis Limited quantitative agreement in amyloidosis |
| Cardiac Magnetic Resonance Fingerprinting | |||
| Hamilton et al. ( |
DL to rapidly reconstruct T1 and T2 maps from undersampled ECG-triggered cMRF data. |
CNN trained to output T1/T2 from cMRF signal-time course + RR intervals Train: 8 million signals across 4,000 cardiac rhythms, test |
Low error (robust) Good 700x acceleration |
| Eck et al. ( |
cMRF for rapid, simultaneous myocardial T1/T2 mapping to detect cardiac amyloidosis |
Prospectively gated 3 T cMRF; tissue classification using linear discriminant analysis (LDA) applied to either native T1/T2 or full cMRF signal timecourses Study cohort: 9 cardiac amyloidosis patients, 5 controls |
Elevated myocardial T1 and T2 in CA vs. controls Signal-timecourse-based LDA showed markedly improved group separability compared to native T1/T2 |
| Cavallo et al ( |
CMR Fingerprinting (cMRF) for simultaneous myocardial T1, T2, and ECV quantification in non-ischaemic cardiomyopathy |
Evaluated in patients with nonischemic cardiomyopathy vs. controls |
Demonstrated feasibility of joint T1/T2/ECV quantification in a clinical cohort |
| Diffusion Tensor Imaging | |||
| Phipps et al. ( |
Accelerate DTI by reducing signal averaging in participants living with obesity |
Residual denoising CNN Tested on 20 healthy volunteers, 6 with obesity DTI reconstructed using 8 averages (reference standard) and accelerated: 4, 2, and 1 average(s) image quality and DTI parameters compared-train, |
DL reconstructed 4 average no different to 8 average in image quality and DTI parameters Differences between health and patients with obesity were preserved 2x acceleration |
| Ferreira et al. ( |
Accelerate DTI and reduced breath-holds (BH) for acquisition |
U-net reconstruction DTI parameters predicted from reduced diffusion-weighted acquisitions (5BH, 3BH, 1BH) Train DL performance compared to reference standard (LLS) conventional tensor fitting |
Small differences in DTI parameters between LLS and U-Net methods U-Net outperformed LLS for reduced datasets U-net preserved clinically relevant metrics with fewer-breath-holds |
| Wang et al. ( |
Correct interframe motion in DTI |
Unsupervised DL framework Total dataset ( Trained by optimising a registration objective directly on the data (no ground truth) Tensor aware cascade alignment correcting in-plane and through-plane motion Compared three traditional and two DL methods |
Improved tensor accuracy with DL Best helix-angle agreement with DL Rapid execution |
| Radiomics and Deep-learning feature extraction | |||
| Neisus et al ( |
Differentiate hypertensive heart disease (HHD) from HCM Radiomics-based texture analysis (no deep learning) |
Handcrafted texture features extracted from native T1 maps Classifier: support vector machine (SVM) Cohort: Train/test split: 4:1 within each disease group |
Radiomics outperformed global native T1 in discrimination between HHD from HCM |
| Fan et al. ( |
Differentiate area-at-risk (AAR) from infarct and remote myocardium in Acute MI Radiomics-based texture analysis |
Handcrafted texture features extracted from T2-mapping Cohort: reperfused AMI patients ( |
Texture features outperformed mean T2 for distinguishing AAR from infarct and remote zones No association with functional recovery (EF, strain, LV remodelling) |
| Fahmy et al. ( |
Screen for scar absence in HCM (to avoid unnecessary GBCA) |
CNN based feature extraction from bSSFP cines Comparison of radiomics vs. DL vs. DL-radiomics combined Train + internal test ( External validation ( |
DL-Radiomics outperformed DL only and Radiomics only for discriminating scar absence Overall moderate discrimination only Improved model performance required before clinical utility |
| Nakamori et al. ( |
Investigate whether CMR radiomics can distinguish between non-collagen and inflammation from collagen in DCM. |
Radiomics-based classification framework Handcrafted (no DL) feature extraction from native T1, ECV and LGE Dimensionality reduction using PCA to derive principal radiomics Biopsy validated in DCM ( |
Radiomics outperformed T1/ECV for distinguishing non-collagenous vs. mild-moderate collagen expansion Radiomics associated with inflammatory phenotype not detected by conventional CMR |
| Xiang et al. ( |
Explore risk stratification after reperfused STEMI using radiomics applied to conventional ECV maps |
Supervised radiomics-based prognostic model Handcrafted radiomics features (no DL) Training ( |
ECV-Radiomics-based scoring outperformed conventional metrics for MACE prediction Incremental to clinical markers |
| Raisi-Estabragh et al. ( |
Estimate biological heart age using radiomics |
Handcrafted radiomics features capturing ventricular shape and myocardial texture Bayesian ridge regression with 10-fold cross validation UKB ( Heart age = predicted age—chronological age |
Sex-specific radiomics associated with heart age Phenome-wide association with obesity, cardiometabolic risk, multimorbidity and socioeconomic factors |
| Inacio et al. ( |
Estimate biological heart age from cardiac motion |
Supervised DL using graph neural networks (cardiac surface motion modelled as a graph over time) Train: |
GNN outperformed dense neural network and boosting models Improved age prediction accuracy |
| Mancio et al. ( |
Identification of HCM patients at low likelihood of LGE to enable avoidance of GBCA |
Cine-derived radiomics combined with regional wall thickness and thickening using XGBoost ML Training |
High negative predictive value for LGE Supporting a cine-only rule-out strategy in HCM when combined with radiomics |
| Challenges of translating current AI-enabled methods of tissue characterisation into clinical practice | |||
| Puyol-Anton et al. ( |
Assess sex and racial bias in AI segmentation of cine CMR |
CNN based automated segmentation tool (train ∼4k) for biventricular volumes, mass and EF assessed Bias analysis by Dice scores and volumes errors |
Racial bias detected Not explained by confounders |
| Zhang et al. ( |
Develop automated quality control for T1 mapping |
CNN to detect motion artefacts on T1 maps Attention supervision to focus the network on artefactual segments Trained |
CNN outperformed human artefact detection |
| Augusto et al. ( |
Develop automated MWT measurement in HCM (Laplace WT estimation) |
2D CNN Train Data was compared to measurements of MWT made by 11 experts. |
ML superior MWT precision (test: re-test) compared with clinician experts. |
| Xue et al. ( |
Automated inline (during scan acquisition) myocardial perfusion segmentation |
CNN model was trained to segment the LV, myocardium and RV on perfusion scans. Train Model outputs were compared with manual segmentation. |
High ML segmentation accuracy Real-time inference (<1s) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Imaging and Diagnostics · Cardiovascular Disease and Adiposity · Radiomics and Machine Learning in Medical Imaging
Introduction
Clinical importance of tissue characterisation CMR
The role of Cardiac MRI (CMR) in guiding care has expanded in recent years due to its unique ability to characterise key myocardial disease processes. Central to the diagnostic power of CMR is the characterisation of focal fibrosis (scar) by late gadolinium enhancement (LGE) which employs gadolinium-based contrast agent (GBCA) (1, 2). LGE transmurality due to myocardial infarction was thought to predict recovery of function through revascularisation (3) although this paradigm has recently been challenged (4). In hypertrophic cardiomyopathy (HCM), a high burden of LGE (defined as >15% of myocardium) influences risk stratification (5). In non-ischaemic cardiomyopathy (NICM), specific scar patterns may be suggestive of underlying genetic substrate (6). Furthermore, the presence of LGE appears to predict arrhythmic risk (7), and may therefore guide the implantation of devices in the future (8). Other myocardial processes can be characterised using quantitative parametric mapping [T1, T2/T2* and extracellular volume (ECV)], which plays a key role in phenotyping myocardial disease and guiding treatment (9). T1 maps can quantify myocardial diffuse fibrosis in multiple diseases and infiltration such as amyloid deposition and detect storage disorders such as Fabry's disease (9). Post-contrast T1 mapping allows calculation of the extracellular volume fraction (ECV) (10) which is particularly useful in detecting cardiac amyloidosis and monitoring its response to treatment (10). T2 maps allows detection of active inflammation in myocarditis, cardiac sarcoidosis, and Takotsubo cardiomyopathy (9, 11, 12). T2* mapping is the standard method for detecting and quantifying myocardial iron overload, and guiding chelation therapy (13).
Challenges in tissue characterisation CMR and the promise of AI
Challenges remain across several stages of workflow in tissue characterisation CMR. Reliance on GBCA excludes certain patients, including those with severe renal impairment, needle phobia, or contrast allergy (1, 2). Image quality is variable, often degraded by cardiac and respiratory motion, and some techniques are inherently low-signal or require long acquisition and reconstruction times, increasing resource demands. Manual segmentation to delineate and quantify scar in LGE is time-consuming and prone to observer variability (14).
Artificial intelligence (AI) offers several advantages to address these challenges. AI can exploit and enhance native signals in non-contrast imaging to generate contrast-free scar mapping; automate labour-intensive tasks throughout the imaging pipeline including image acquisition, reconstruction and segmentation; align (register) images to address cardiac and breathing motion; enhance signal and resolution in under-sampled low-signal-to-noise datasets; and automate and enable novel feature extraction and predictive modelling (1, 2, 11, 14–27).
Most existing reviews of AI in CMR have centred on automation or acceleration of cardiac function assessment and general image analysis. In this review, we focus specifically on AI applied to left ventricular tissue characterisation (Table 1).
Late gadolinium enhancement segmentation
LGE interpretation currently relies on expert identification of abnormal hyperintense regions and, as such, is time consuming, suffers from high inter-observer variability and is challenging due to heterogenous acquisition and analysis techniques; deep-learning AI has shown potential in overcoming this challenge.
In HCM, a three-dimensional convolutional neural network (CNN) showed good agreement with manual quantification, providing segmentation at high speed and maintained high performance across multiple scanner vendors (14). Automated LGE quantification of ischaemic scar using CNNs surpassed clinicians in prediction of arrhythmic events in an ischaemic cardiomyopathy cohort (18).
Other neural network architectures that have been explored for LGE segmentation include fully convolutional networks (FCNs) (19) and autoencoders (20). FCNs have been less explored than CNNs but have demonstrated good accuracy in a small study on ischaemic scar (19). Autoencoders have been applied to align features between cine (bSSFP) and LGE images thereby enabling more accurate scar segmentation (where annotations are sparse) by leveraging well annotated cine CMR (20). Another approach includes slice-level identification of the presence of scar accompanied by probabilistic scar localisation using interpretability techniques such as GradCAM (28).
The inclusion of LGE segmentation tasks in international medical imaging challenges has spurred the development of benchmarked segmentation and classification methods for this application (29). Moreover, LGE segmentation performed using a vision foundational model pretrained on millions of unlabelled images has shown promising performance and a potential means to overcome the shortage of large labelled LGE datasets (30).
However, a challenge in developing AI methods for LGE segmentation is the lack of standardised analysis criteria that can be used as ground truth for AI models. Large scale external validation of these methods is also required before widespread adoption into clinical care.
Parametric mapping
Parametric mapping techniques (T1, T2, T2* and ECV mapping) traditionally involve mathematical fitting of different cardiac images acquired with different acquisition parameters. Appropriate alignment (registration) is essential, as unaccounted cardiac or respiration motion will reduce image quality and parameter quantification accuracy. AI has been applied to mapping techniques such as T1 to improve motion correction. For example, CNN approaches like MOCOnet, trained on over 1,500 UK Biobank T1 maps with artificially generated motion artefacts, achieved rapid (<1 s) and robust suppression of artefacts in native T1 maps from 200 test subjects, outperforming traditional methods in both visual quality and reproducibility (31). More recently, deep learning–based end-to-end reconstruction frameworks have integrated motion estimation and correction into a single pipeline for 3D whole-heart T1/T2 mapping, reducing reconstruction times from hours to seconds while preserving quantitative accuracy (11). These techniques demonstrate how deep learning can enhance motion correction, enabling more rapid and accurate mapping quantification. Commonly motion correction is applied in-line for clinical scans, and therefore work is needed for deployment across scanners and vendors.
Synthetic post-contrast imaging
Contrast-free “synthetic LGE” has been developed through the use of generative adversarial networks (GANs). Two leading techniques have been developed: “virtual native enhancement (VNE)” (1, 2), which has native T1 maps and cine MRI as inputs, and has been applied to chronic myocardial infarction (MI) (2) and HCM (1), and “cine-generated enhancement (CGE)”, which identifies LGE from cine MRI only and has been applied to acute MI (16). Both techniques demonstrated potential to detect the respective pathologies tested. Furthermore, infarct VNE has been validated ex-vivo in porcine models (2).
The success of the synthetic LGE methods suggests that enough information to identify scar or fibrosis is likely to exist in contrast-free images which may be conceptually challenging for CMR operators. This scar identification may be suitable for AI only and difficult for human operators. The propensity of GANs for hallucinations makes it critical to validate this concept in large diverse datasets, especially in the presence of poor image quality (often degraded due to patient factors) found in the clinical arena (1, 32).
An alternative to GANs to synthesise LGE from cine CMR is the analysis of local motion biomarkers (such as displacements and local strains) in cine MRI. Here, scar is identified due to its different biomechanical properties (e.g., stiffness) when compared to healthy myocardium. In a small study, a motion-feature learning framework based on long-short term memory (LSTMs) applied to cine CMR identified myocardial infarction, achieving a high accuracy when evaluated against the manual segmentation ground-truth (21).
Despite modest patient numbers used to train these models (1, 2, 16), initial proof-of-concept work could support contrast-free identification of scar. Ruling out scar may be useful to negate the use of GBCA in patients with low pre-test probability. Further, as opposed to replicating LGE, these techniques may even provide incremental information, giving additional trust to LGE findings or even detecting subtle abnormalities missed by LGE alone.
Moreover, as for LGE, GANs have also been used to generate virtual contrast-enhanced T1 maps using native (contrast-free) T1 map inputs for virtual ECV mapping (vECV). vECV showed good agreement with conventional ECV in healthy volunteers and myocarditis but was more modest in cardiac amyloidosis. Authors also noted some focal mapping abnormalities were not recapitulated using vECV and some lesions were “hallucinated” a known hazard of GAN based deep learning. Nevertheless, the study determined proof-of-principle for virtual ECV to expand this valuable diagnostic tool to patients otherwise precluded from GBCA and faster and cheaper CMR (27).
Cardiac magnetic resonance fingerprinting
Cardiac magnetic resonance fingerprinting (MRF) is an advanced MRI approach that simultaneously characterises several MR parameters (e.g., T1, T2, T2*, proton density, fat fraction, flow parameters) using a different paradigm to conventional MRI (33). In MRF, the application of MR pulses is not designed to create a human-interpretable image, but instead to match the response of the tissue in each voxel to a pre-existing database (dictionary) of properties (33). This approach has several advantages over conventional mapping including inherent co-registration of all parameter maps, avoidance of confounding based on system hardware, sequence, heart rate and arrhythmia (22). This technique has shown its ability to discriminate health from disease in proof-of-concept work in cardiac amyloidosis (34) and also has shown feasibility in non-ischaemic cardiomyopathy (35).
Artificial intelligence can be used to optimise MRF acquisition sequence design and to perform dictionary generation, reconstructions and post-processing at a small fraction of the time of traditional MRFs (22). For example, neural network approaches to cardiac MRF have demonstrated good reproducibility, robustness to cardiac rhythm variability, and the ability to reconstruct quantitative maps in under 400 ms (22). This has potentially laid the foundations for accelerating development in other tissue characteristics such as focal fibrosis and perfusion, and more widespread clinical implementation (34). AI-based methods are likely to accelerate cardiac MRF and improve its practical feasibility, supporting its future adoption in routine clinical practice.
Diffusion tensor cardiac MRI
Cardiac diffusion tensor imaging (cDTI) measures the diffusion of water within an imaging voxel thereby characterising the myocardial microstructural environment and microstructural alteration (36, 37). Its high sensitivity has been utilised to detect microstructural alteration in subclinical HCM (individuals with sarcomeric mutations but without overt left ventricular hypertrophy) and early adverse remodelling in acute MI (36). DTI is an inherently low-signal-to-noise technique as it relies on diffusion-induced signal dephasing. Signal averaging from multiple repeated raw images is therefore used to overcome this, but leads to long scan-times which reduces ability for clinical translation. Moreover, DTI is highly sensitive to motion (cardiac or respiratory).
Denoising convolutional neural networks have been developed to subtract noise from cardiac DTI, needing two-/ four-fold fewer signal averages while preserving image quality and accurate parametric differences between healthy volunteers and individuals with obesity—a challenging patient group in this domain due to lack of surface-coil proximity to the heart (15). Deep learning has also been applied to reconstruct quantitative maps from undersampled data, reducing the number of breath-holds required in DTI (23). Further, AI methods have also been used to correct inter-frame motion in cardiac DTI with promising results (38).
Radiomics and deep-learning feature extraction
Radiomics is an image analysis framework that extracts voxel-level features (quantitative properties) to characterise tissue phenotypes. Radiomics features can include intensity-based statistics, spatial texture metrics, tissue morphological parameters, and features derived from the application of image filters. Feature extraction is typically preceded by segmentation, i.e., by the identification of the desirable regions of interest in the image. Machine learning algorithms are then employed to select and non-linearly combine radiomic features in the optimal combination for a given task (e.g., the identification of pathology).
Feature selection and dimensionality reduction are typically performed with unsupervised machine learning methods such as principal component analysis or minimum redundancy maximum relevance techniques. Classification can then be performed using machine learning techniques such as support vector machines or random forests. Proof-of-concept studies have shown potential applications in disease discrimination, risk stratification and non-contrast identification of scar (39). Texture analysis has been applied to T1 mapping to enhance discrimination between HCM and hypertensive heart disease beyond T1 mapping alone (40). Further work in HCM has demonstrated the potential to combine texture analysis with regional wall thickening derived from cine imaging to identify patients without focal fibrosis, thereby avoiding unnecessary GBCA exposure. A particular strength of this study was the use of multi-centre external validation, supporting its generalisability and scalability (41). Texture analysis applied to T2 mapping permitted visualisation of “area-at-risk” in reperfused MI—an ability historically restricted to LGE—but this parameter did not translate into prognostication of functional recovery at convalescence (42). Furthermore, radiomics analysis of ECV mapping in reperfused ST-segment elevation myocardial infarction (STEMI) demonstrated incremental prognostic value for adverse events beyond conventional markers and ECV alone, potentially reflecting discrimination between intramyocardial haemorrhage and myocardial necrosis, which exert divergent effects on ECV (25). These findings highlight the ability of radiomics-based texture analysis to capture tissue heterogeneity and disease biology that are not apparent on conventional imaging. This concept is further supported by a recent study validating radiomics features derived from T1 and ECV mapping against septal myocardial biopsy histology, demonstrating the detection of chronic myocardial inflammation in dilated cardiomyopathy (24).
An important advantage of radiomics is that it can use conventional CMR to build models that provide disease insights unavailable from conventional radiological analysis. For example, a UK Biobank study developed a heart-age estimation model using radiomics features as inputs and chronological age as the output, deriving a “delta-heart-age” that was then associated with multi-organ, metabolic, and socioeconomic markers in a phenome-wide analysis (43).
However, direct analysis of cardiac MRI using neural networks (NNs), such as 2D and 3D convolutional neural networks or vision transformers, has the potential to outperform machine learning methods based on radiomics features (44). This is because, given enough data, these architectures can extract powerful imaging features for clinical tasks, at the expense of human interpretability. A bottleneck to the implementation of these NN methods, which traditional radiomics approaches do not suffer from, is the lack of large labelled datasets for training and validation. Another approach in this area is the combination of deep learning features with radiomics ones (17). Further work is needed to explore the clinical applicability of these techniques, especially their accuracy for diagnostic purposes. A challenge in translating radiomics and NN methods is domain shift due to differences in scanner type, field strength, and sequence parameters, highlighting the need for reproducible feature selection and robust network design and training.
Challenges of translating current AI-enabled methods of tissue characterisation into clinical practice
Despite the substantial advantages afforded by AI, several challenges in widespread adoption remain. A major barrier to AI model development is the shortage of well-curated datasets with reliable clinical labels. Foundational models—large AI models pretrained using self-supervised learning on unlabelled data—offer a promising strategy to address this limitation, as they can be adapted to multiple downstream tasks using comparatively small labelled datasets (30, 45) This framework also supports integration of multi-imaging and multi-modal data, including genomics and medical reports analysed using large language models, enabling more complex clinical learning tasks.
Nevertheless, model generalisability remains a key challenge. AI models are often trained on relatively small datasets and perform poorly in out-of-distribution settings, such as external validation cohorts. This is particularly problematic in CMR due to variation in scanner hardware, imaging protocols, and patient populations, which also complicates benchmarking across models. In addition, AI tissue characterisation models are frequently trained on research datasets with higher image quality than encountered in routine clinical practice, often excluding patients with arrhythmias, implantable devices, or limited breath-hold capacity. Ensuring training datasets capture real-world acquisition variability is therefore a priority. Access to diverse clinical data is further constrained by patient confidentiality concerns (46). Federated learning offers a solution, enabling collaborative model development across institutions without direct data sharing. In this paradigm, training occurs locally and only model parameters (gradients,weights) are shared and aggregated centrally (47). Data imbalance also raises fairness concerns, as models trained on skewed datasets may underperform in under-represented groups, including by race and sex, potentially exacerbating health disparities. For example, cine segmentation models trained on UK Biobank data—where over 80% of participants are White—perform less well in more diverse populations (48). Furthermore, it is possible to identify race from cine images due to areas outside the heart such as subcutaneous fat, leading to potential for misuse (26). Proposed mitigation strategies include improving dataset balance—although this may be challenging in rare diseases—as well as generative data augmentation and group-specific model training (48). Furthermore, outputs from deep learning models are often difficult for humans to interpret (“black box”), creating additional barriers to clinical adoption. Explainable artificial intelligence (XAI) methodologies can, in some circumstances, be employed to enhance user trust and are likely to feature in next-generation AI models applied to tissue characterisation (49). For example, saliency mapping and Grad-CAM can identify image regions that contribute most strongly to model predictions and have been applied to tasks such as quality control in T1 mapping (50) and LGE classification (28). However, as demonstrated in AI-ECG applications, improvements in explainability must be balanced against potential reductions in predictive performance (51).
Safe deployment of AI tools will also require adherence to evolving regulatory standards. The US Food and Drug Administration (FDA) has issued Good Machine Learning Practice (GMLP) guidelines to promote transparency, robustness, and quality control in medical AI systems (52). Importantly, regulatory frameworks may need to evolve further to accommodate adaptive or continuously learning AI tools, which differ fundamentally from static, “locked” algorithms. Successful integration of AI-based tissue characterisation into clinical workflows will depend on deployment through accessible open-source frameworks or seamless incorporation into vendor platforms, ensuring usability, interoperability, and clinician uptake. One promising approach is the real-time deployment of AI models during clinical MR image acquisition, enabling radiographers and clinicians to identify adverse features before the patient leaves the scanner bore, tailor imaging protocols, and reduce the need for repeat scans (53, 54). Such frameworks are also amenable to continuous learning through the ongoing acquisition of labelled clinical data, supporting iterative improvements in model performance.
Future perspective
AI offers substantial advantages for tissue characterisation in CMR, with the potential to enhance diagnostic accuracy, improve risk modelling, and deepen disease understanding (Table 2). Direct clinical benefits include real-time quality control during image acquisition (55) and real-time detection of pathology. AI-based reconstruction using undersampling strategies can markedly accelerate acquisition and may be particularly impactful for low-field CMR systems, whose lower cost, reduced resource requirements, and improved safety profile offer a more scalable route to expanding access to cardiac MRI (56).
Future developments may include AI-driven co-registration of multiple CMR modalities—such as cines, LGE, DTI, and parametric maps—into a unified and more coherent three-dimensional representation. End-to-end deep learning approaches for probabilistic risk prediction from CMR images are also likely to expand, with explainable AI supporting interpretability and clinician trust. Finally, just as clinicians integrate clinical variables, ECG, and imaging to guide care, multimodal AI is expected to enable integration of these data at greater dimensionality and scale, supporting more accurate risk stratification and personalised therapy than previously possible. Clinicians alongside scientific and technical experts will be central to overseeing this evolution, ensuring fairness, generalisability, and robust performance for clinical care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zhang Q Burrage MK Lukaschuk E Shanmuganathan M Popescu IA Nikolaidou C Toward replacing late gadolinium enhancement with artificial intelligence virtual native enhancement for gadolinium-free cardiovascular magnetic resonance tissue characterization in hypertrophic cardiomyopathy. Circulation. (2021) 144(8):589–99. 10.1161/CIRCULATIONAHA.121.05443234229451 PMC 8378544 · doi ↗ · pubmed ↗
- 2Zhang Q Burrage MK Shanmuganathan M Gonzales RA Lukaschuk E Thomas KE Artificial intelligence for contrast-free MRI: scar assessment in myocardial infarction using deep learning–based virtual native enhancement. Circulation. (2022) 146(20):1492–503. 10.1161/CIRCULATIONAHA.122.06013736124774 PMC 9662825 · doi ↗ · pubmed ↗
- 3Kim RJ Wu E Rafael A Chen EL Parker MA Simonetti O The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N Engl J Med. (2000) 343(20):1445–53. 10.1056/NEJM 20001116343200311078769 · doi ↗ · pubmed ↗
- 4Perera D Clayton T O’Kane PD Greenwood JP Weerackody R Ryan M Percutaneous revascularization for ischemic left ventricular dysfunction. N Engl J Med. (2022) 387(15):1351–60. 10.1056/NEJ Moa 220660636027563 · doi ↗ · pubmed ↗
- 5Ommen SR Ho CY Asif IM Balaji S Burke MA Day SM 2024 AHA/ACC/AMSSM/HRS/PACES/SCMR guideline for the management of hypertrophic cardiomyopathy: a report of the American heart association/American college of cardiology joint committee on clinical practice guidelines. Circulation. (2024) 149(23):e 1239–311. 10.1161/CIR.000000000000125038718139 · doi ↗ · pubmed ↗
- 6Augusto JB Eiros R Nakou E Moura-Ferreira S Treibel TA Captur G Dilated cardiomyopathy and arrhythmogenic left ventricular cardiomyopathy: a comprehensive genotype-imaging phenotype study. Eur Heart J Cardiovasc Imaging. (2020) 21(3):326–36. 10.1093/ehjci/jez 18831317183 · doi ↗ · pubmed ↗
- 7Klem I Klein M Khan M Yang EY Nabi F Ivanov A Relationship of LVEF and myocardial scar to long-term mortality risk and mode of death in patients with nonischemic cardiomyopathy. Circulation. (2021) 143(14):1343–58. 10.1161/CIRCULATIONAHA.120.04847733478245 · doi ↗ · pubmed ↗
- 8Flett A Cebula A Nicholas Z Adam R Ewings S Prasad S Rationale and study protocol for the BRITISH randomized trial (using cardiovascular magnetic resonance identified scar as the benchmark risk indication tool for implantable cardioverter defibrillators in patients with nonischemic cardiomyopathy and severe systolic heart failure). Am Heart J. (2023) 266:149–58. 10.1016/j.ahj.2023.09.00837777041 · doi ↗ · pubmed ↗