Long-term outcomes of pseudomyxoma peritonei after cytoreductive surgery and hyperthermic intraperitoneal chemotherapy and its relevant risk factors in China: a retrospective study
Shuncai Gao, Xiang Zhang, Ziyang Yu, Junwei Zhang

TL;DR
This study examines long-term survival and risk factors for pseudomyxoma peritonei patients treated with surgery and chemotherapy in China.
Contribution
The study identifies key prognostic factors in a large Chinese cohort of PMP patients treated with CRS-HIPEC.
Findings
Median survival was 56 months for overall survival and 45 months for event-free survival.
Preoperative tumor markers, CC-score, and high-grade PMP were independent predictors of poorer outcomes.
Intraoperative hypotension and hyperthermia did not affect survival or event-free survival.
Abstract
Pseudomyxoma peritonei (PMP), generally spread of low grade appendiceal mucinous neoplasm (mucinous appendix neoplasms) into the abdominal cavity, is conventionally treated with cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (CRS-HIPEC). Prognostic factors of small cohort sizes remain incomplete and conflicting. This large-scale study aimed to characterize long-term survival outcomes and identify prognostic factors in PMP patients following CRS-HIPEC. We conducted a retrospective cohort study of 432 consecutive PMP patients treated with CRS-HIPEC at Aerospace Center Hospital (Beijing, China) from June 2014 to December 2020. Overall survival (OS) served as the primary endpoint, with event-free survival (EFS) as the secondary endpoint. Multivariable Cox proportional hazards models were employed to identify independent prognostic factors. With median survival…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
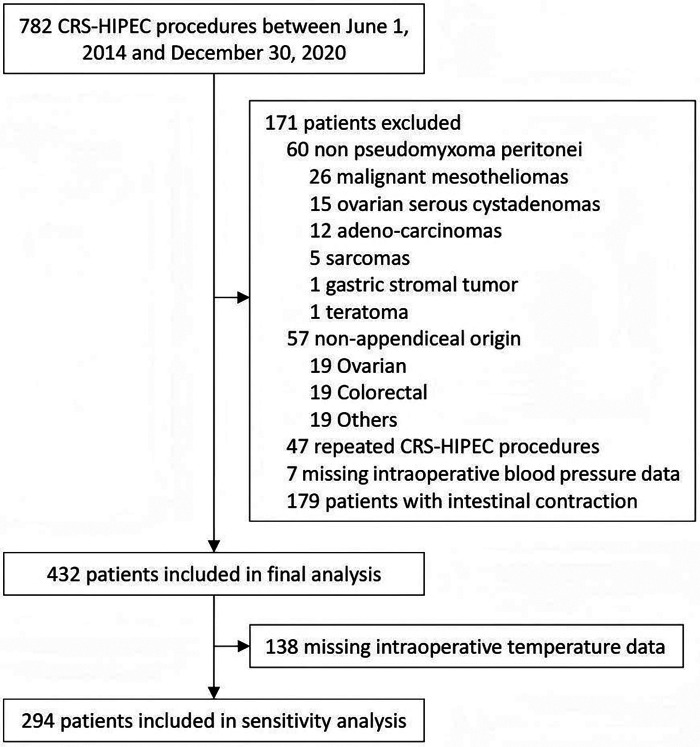 Figure 1
Figure 1| Characteristics | Statistical description | Overall survival | Event-free survival | ||
|---|---|---|---|---|---|
| Hazard ratio (95% CI) | Hazard ratio (95% CI) | ||||
| Demographic characteristics | |||||
| Age, year | 57 ± 11 | 1.02 (1.00, 1.04) | 0.040 | 1.01 (0.99, 1.03) | 0.243 |
| Female sex | 281 (65.0%) | 1.11 (0.72, 1.69) | 0.642 | 0.99 (0.70, 1.39) | 0.931 |
| Body mass index, kg/m2 | 23.2 (21.2, 26.0) | 0.96 (0.90, 1.02) | 0.191 | 1.00 (0.95, 1.05) | 0.909 |
| General status | |||||
| Charlson comorbidity index | 8.0 (8.0, 8.0) | 0.92 (0.61, 1.39) | 0.685 | 1.06 (0.79, 1.42) | 0.702 |
| ASA physical status | |||||
| I-II | 241 (55.8%) | Ref. | Ref. | ||
| III-IV | 191 (44.2%) | 1.43 (0.95, 2.15) | 0.086 | 1.32 (0.95, 1.85) | 0.098 |
| Barthel index | 10.0 (9.5, 10.0) | 0.84 (0.73, 0.97) | 0.017 | 0.84 (0.75, 0.95) | 0.005 |
| History of previous therapy | |||||
| Prior surgical score | |||||
| 0–2 | 312 (72.2%) | Ref. | Ref. | ||
| 3 | 120 (27.8%) | 1.39 (0.90, 2.16) | 0.143 | 1.40 (0.98, 2.00) | 0.065 |
| Prior chemotherapy | 83 (19.2%) | 1.44 (0.92, 2.26) | 0.115 | 1.84 (1.28, 2.65) | 0.001 |
| Prior HIPEC exposure | 88 (20.4%) | 1.43 (0.87, 2.35) | 0.162 | 1.42 (0.96, 2.12) | 0.084 |
| Preoperative laboratory tests | |||||
| Hemoglobin, g/L | 117 ± 18 [14] | 0.99 (0.97, 1.00) | 0.011 | 0.99 (0.98, 1.0) | 0.003 |
| Albumin, g/L | 37 ± 4 [10] | 0.94 (0.90, 0.98) | 0.007 | 0.92 (0.89, 0.96) | <0.001 |
| Tumor markers (CA125, CA199, CEA) | |||||
| Normal | 106 (24.5%) | Ref. | Ref. | ||
| 1 raised | 113 (26.2%) | 6.88 (1.63, 29.0) | 0.009 | 4.17 (1.78, 9.85) | 0.001 |
| 2 raised | 98 (22.7%) | 10.25 (2.41, 43.6) | 0.002 | 6.04 (2.56, 14.28) | <0.001 |
| All raised | 115 (26.6%) | 20.9 (5.05, 86.27) | <0.001 | 9.19 (3.95, 21.37) | <0.001 |
| Characteristics | Statistical description ( | Overall survival | Event-free survival | ||
|---|---|---|---|---|---|
| Hazard Ratio (95% CI) | Hazard Ratio (95% CI) | ||||
| Intraoperative data | |||||
| Peritoneal cancer index | |||||
| 0–10 | 105 (24.3%) | Ref. | Ref. | ||
| 11–20 | 58 (13.4%) | 4.59 (1.63, 12.90) | 0.004 | 2.46 (1.22, 4.96) | 0.012 |
| 21–30 | 153 (35.4%) | 5.44 (2.17, 13.64) | <0.001 | 2.97 (1.67, 5.27) | <0.001 |
| 31–39 | 116 (26.9%) | 5.71 (2.17, 15.01) | <0.001 | 2.85 (1.54, 5.28) | <0.001 |
| Completeness of cytoreduction score | |||||
| 0 | 102 (23.6%) | Ref. | Ref. | ||
| 1 | 120 (27.8%) | 4.79 (1.98, 11.57) | <0.001 | 2.36 (1.31, 4.25) | 0.004 |
| 2 | 117 (27.1%) | 4.41 (1.87, 10.42) | <0.001 | 2.51 (1.44, 4.37) | 0.001 |
| 3 | 93 (21.5%) | 5.09 (2.04, 12.68) | <0.001 | 2.71 (1.46, 5.02) | 0.002 |
| Complete cytoreduction | 222 (51.4%) | 0.62 (0.41, 0.95) | 0.028 | 0.65 (0.46, 0.92) | 0.014 |
| Duration of surgery, h | 8.0 (6.5, 9.6) | 1.08 (0.98, 1.19) | 0.129 | 1.08 (1.00, 1.17) | 0.063 |
| Artificial colloid, per 500 mL | 5.2 (4.0, 6.4) | 1.16 (1.05, 1.29) | 0.005 | 1.13 (1.04, 1.23) | 0.005 |
| Crystalloid, per 500 mL | 6.8 (5.2, 8.4) | 1.14 (1.03, 1.25) | 0.008 | 1.09 (1.01, 1.18) | 0.026 |
| Blood transfusion | 244 (56.5%) | 2.67 (1.58, 4.52) | <0.001 | 1.97 (1.33, 2.90) | <0.001 |
| Estimated blood loss, per 500 mL | 3.0 (1.0, 3.2) | 1.202 (1.09, 1.31) | <0.001 | 1.14 (1.06, 1.23) | <0.001 |
| Area under threshold of MAP | |||||
| <75 mmHg | 89 (45, 142) | 1.00 (1.00, 1.01) | 0.083 | 1.00 (1.00, 1.01) | 0.056 |
| <70 mmHg | 43 (18, 80) | 1.00 (1.00, 1.01) | 0.075 | 1.00 (1.00, 1.01) | 0.056 |
| <65 mmHg | 14 (4, 33) | 1.00 (1.00, 1.01) | 0.071 | 1.00 (1.00, 1.01) | 0.077 |
| Intraperitoneal chemotherapy regimens | |||||
| Intraperitoneal chemotherapy | |||||
| HIPEC alone | 106 (24.5%) | Ref. | Ref. | ||
| HIPEC plus EPIC | 326 (75.5%) | 0.49 (0.32, 0.76) | 0.001 | 0.64 (0.45, 0.92) | 0.017 |
| Combinations of intraperitoneal chemotherapy-1 | |||||
| Non-cisplatin containing | 147 (34.0%) | Ref. | Ref. | ||
| Cisplatin containing | 285 (66.0%) | 0.73 (0.46, 1.16) | 0.178 | 0.76 (0.53, 1.08) | 0.130 |
| Combinations of intraperitoneal chemotherapy-2 | |||||
| 5-fluorouracil/mitomycin C | 147 (34.0%) | Ref. | Ref. | ||
| Cisplatin only | 75 (17.4%) | 0.93 (0.49, 1.77) | 0.833 | 0.81 (0.48, 1.37) | 0.440 |
| Cisplatin plus another | 173 (40.0%) | 0.64 (0.37, 1.13) | 0.122 | 0.74 (0.49, 1.11) | 0.142 |
| Cisplatin plus two others | 37 (8.6%) | 0.49 (0.07, 3.61) | 0.488 | 0.73 (0.23, 2.35) | 0.600 |
| Postoperative data | |||||
| Histopathology subtype | |||||
| Low-grade | 323 (74.8%) | Ref. | Ref. | ||
| High-grade | 109 (25.2%) | 2.61 (1.74, 3.92) | <0.001 | 1.81 (1.27, 2.56) | <0.001 |
| Tumor markers (CA125, CA199, CEA) | |||||
| Normal | 198 (45.8%) | Ref. | Ref. | ||
| 1 raised | 109 (25.2%) | 1.58 (0.92, 2.73) | 0.099 | 1.58 (1.02, 2.46) | 0.040 |
| ≥2 raised | 125 (28.9%) | 3.19 (1.94, 5.23) | <0.001 | 2.77 (1.86, 4.13) | <0.001 |
| Acute kidney injury | 43 (10.0%) | 1.26 (0.61, 2.60) | 0.540 | 1.25 (0.70, 2.21) | 0.452 |
| Other major complications within 30 days | 93 (21.5%) | 1.49 (0.94, 2.36) | 0.087 | 1.30 (0.88, 1.91) | 0.190 |
| Characteristics | Statistical description ( |
|---|---|
| Duration of follow-up, month | 40 (25, 55) |
| Re-hospitalization for PMP | 129 (29.9%) |
| Scheduled re-hospitalization | 247 (57.2%) |
| Number of deaths during follow-up | 94 (21.8%) |
| Number of events during follow-up | 140 (32.4%) |
| Event-free survival, month | 45 (40, 51) |
| Overall survival, month (all-cause death) | 56 (50, 61) |
| Parameter | Overall survival | Event-free survival | ||
|---|---|---|---|---|
| Hazard ratio (95% CI) | Hazard ratio (95% CI) | |||
| Age, year | 1.01 (0.99, 1.04) | 0.267 | 1.00 (0.98, 1.01) | 0.589 |
| Body mass index, kg/m2 | 0.98 (0.92, 1.05) | 0.621 | 1.03 (0.97, 1.08) | 0.330 |
| ASA physical status | ||||
| I-II | Ref. | Ref. | ||
| III-IV | 1.24 (0.76, 2.01) | 0.395 | 1.07 (0.72, 1.59) | 0.736 |
| Barthel index | 0.97 (0.81, 1.16) | 0.201 | 0.86 (0.74, 0.98) | |
| Prior surgical score | ||||
| 0–2 | Ref. | Ref. | ||
| 3 | 0.80 (0.47, 1.35) | 0.397 | 0.96 (0.64, 1.43) | 0.831 |
| Prior chemotherapy | 1.22 (0.71, 2.09) | 0.474 | 1.40 (0.91, 2.14) | 0.126 |
| Prior HIPEC exposure | 1.05 (0.59, 1.85) | 0.873 | 1.13 (0.72, 1.78) | 0.586 |
| Preoperative hemoglobin, g/L | 0.99 (0.98, 1.01) | 0.482 | 1.00 (0.99, 1.01) | 0.975 |
| Preoperative albumin, g/L | 1.01 (0.94, 1.08) | 0.763 | 0.95 (0.90, 1.00) | 0.071 |
| Preoperative tumor markers (CA125, CA199, CEA) | ||||
| Normal | Ref. | Ref. | ||
| 1 raised | 4.90 (1.11, 21.61) | 2.92 (1.15, 7.41) | ||
| 2 raised | 5.67 (1.22, 26.42) | 3.94 (1.48, 10.48) | ||
| All raised | 10.20 (2.23, 46.67) | 5.97 (2.22, 16.07) | ||
| Completeness of cytoreduction score | ||||
| 0 | Ref. | Ref. | ||
| 1 | 3.37 (1.05, 6.04) | 1.87 (0.89, 2.40) | 0.077 | |
| 2 | 5.62 (2.15, 10.64) | 3.79 (1.54, 5.57) | ||
| 3 | 9.41 (3.77, 16.37) | 4.24 (2.40, 9.57) | ||
| Duration of surgery, h | 0.98 (0.86, 1.13) | 0.797 | 0.97 (0.87, 1.09) | 0.626 |
| Blood transfusion | 1.09 (0.53, 2.24) | 0.817 | 1.18 (0.67, 2.05) | 0.572 |
| Aera under MAP < 65 | 1.01 (0.99, 1.01) | 0.770 | 1.00 (0.99, 1.01) | 0.883 |
| Intraperitoneal chemotherapy | ||||
| HIPEC alone | Ref. | Ref. | ||
| HIPEC plus EPIC | 0.67 (0.35, 1.26) | 0.213 | 0.75 (0.44, 1.28) | 0.291 |
| Combinations of intraperitoneal chemotherapy-2 | ||||
| 5-fluorouracil/mitomycin C | Ref. | Ref. | ||
| Cisplatin only | 0.70 (0.30, 1.61) | 0.396 | 0.57 (0.29, 1.15) | 0.116 |
| Cisplatin plus another | 0.97 (0.50, 1.88) | 0.918 | 0.88 (0.54, 1.44) | 0.613 |
| Cisplatin plus two others | 0.83 (0.11, 6.41) | 0.861 | 0.95 (0.28, 3.21) | 0.940 |
| Histopathology | ||||
| Low-grade | Ref. | Ref. | ||
| High-grade | 1.80 (1.10, 2.93) | 1.93 (1.15, 2.80) | ||
| Other major complications within 30 days | 0.98 (0.59, 1.64) | 0.941 | 0.96 (0.63, 1.46) | 0.837 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntraperitoneal and Appendiceal Malignancies · Ovarian cancer diagnosis and treatment · Appendicitis Diagnosis and Management
Introduction
1
Pseudomyxoma peritonei (PMP) is a rare condition, with reported epidemiological variations across regions. In urban China, its estimated prevalence is 2.47 per million person-years, and the incidence is 1.19 per million person-years (1). In contrast, European data suggest a higher prevalence of 22 cases per million per year and an incidence of 3.2 per million per year (2). PMP is generally spread of low-grade mucinous appendix neoplasms into the abdominal cavity (3, 4). Currently, cytoreductive surgery combined with hyperthermic intraperitoneal chemotherapy (CRS-HIPEC) was endorsed by the Peritoneal Surface Oncology Group International as first-line therapy (5). Studies demonstrated that CRS-HIPEC at experienced centers with improved surgical techniques and integrated hemostasis techniques was safe (6) and could achieve 5- and 10-year survival rates of 74%–87% and 63%–73% in PMP patients, respectively (7, 8). Outcomes with CRS-HIPEC for PMP have been outstanding in prior studies because this disease is rather indolent with little metastatic and upstage potential. But, relapse after CRS-HIPEC was common, with the peritoneum being the most commonly relapse site, and the surgical resection of relapse disease could result in prolonged survival (9).
Prognostic factors for PMP after CRS-HIPEC remained incompletely characterized within limited studies except those concentrating on relapse of PMP (9) and perioperative safety after CRS-HIPEC (6). Key determinants included tumor-related factors (histologic grade, disease extent, peritoneal cancer index) (7, 10, 11), treatment-related parameters (completeness of cytoreduction, major postoperative complications, center experience) (12), and tumor markers (elevated CEA/CA199) (13). Current evidence showed conflicting results, with some studies emphasizing histologic grade alone while others highlighting multifactorial influences (7). Research progress is limited by PMP's rarity, resulting in small cohort sizes and unvalidated long-term outcomes (14).
Actually, aside from surgery-related factors, increasing studies demonstrated that anesthesia-related factors were also associated with surgical outcomes, as exemplified by intraoperative blood pressure management, especially hypotension (15–23). And in patients with cancer, evidence of relationship between intraoperative hypotension and long-term survival also had been proved (24–26). However, study reported the association between anesthesia-related factors and the long-term outcomes of PMP patients remained scarce.
Herein, this large-scale study aimed to investigate the long-term outcomes in PMP patients after CRS-HIPEC and the risk factors for long-term outcomes.
Materials and methods
2
Study design and patients
2.1
This retrospective cohort study included patients diagnosed with PMP confirmed by both surgical specialists and pathologists who underwent CRS-HIPEC at the Aerospace Center Hospital in Beijing, China, between June 2014 and December 2020. The study was approved by the Ethics Committee of the Aerospace Center Hospital (approval #2021-QT-014). Informed consent for the surgical specimens, imaging data, medical records used for academic exchange, scientific research, and teaching purposes was obtained from all patients and recorded in the Surgical Consent Form before all surgeries in our hospital in accordance with the local legislation and institutional requirements.
The inclusion criteria included patients aged ≥18 years and PMP originated from mucinous appendix neoplasms. The exclusion criteria included patients with missing intraoperative data, incomplete outcome data, repeated CRS-HIPEC procedure, or combined with intestinal contraction.
Perioperative procedures
2.2
All patients received standard intraoperative monitoring including electrocardiogram, invasive arterial blood pressure, pulse oximetry, end-tidal carbon dioxide, inhalational anesthetic concentration, nasopharyngeal temperature, and urine output measurement. General anesthesia was administered using a combination of propofol, volatile anesthetics (primarily sevoflurane), opioids, and muscle relaxants. Temperature management followed institutional protocols: employing an underbody warming blanket was used during CRS to prevent hypothermia (discontinued 30 min before HIPEC); while ice packs were applied to the head and neck region during HIPEC to mitigate systemic hyperthermia.
The CRS was performed according to Sugarbaker's technique (27), with surgical decisions made based on intraoperative findings. Following CRS, HIPEC was conducted using a closed-abdomen technique involving four catheters (two inflow/two outflow) connected to a perfusion system (RHL-2000B, Jilin Maida Technology Development Co., Ltd., China) that circulated chemotherapeutic agents (typically cisplatin 50–90 mg, 5-fluorouracil 1 g, and mitomycin C 10–40 mg) at 43.5 °C inflow/42.0 °C outflow temperatures, with perfusion rates of 600–1,000 mL/min for 60–90 min according to the Chinese Expert Consensus (28). After HIPEC, the abdomen was reopened for reconstruction and drainage. Postoperatively, selected patients received early postoperative intraperitoneal chemotherapy (EPIC, days 2–6) with 5-fluorouracil (1 g) ± cisplatin (40–100 mg) or raltitrexed (4–5 mg) per clinical judgment and guidelines.
Data collection
2.3
The preoperative data were gathered from a CRS-HIPEC database, encompassing demographic details (age, sex, and body mass index), overall health status [Charlson comorbidity index (29), American Society of Anesthesiologist classification (30), and Barthel index (31)], history of previous treatments [prior surgical score (PSS), prior chemotherapy, and HIPEC exposure], and preoperative laboratory findings (hemoglobin levels, and tumor markers including CA125, CA199, CEA).
The surgery-related data on the peritoneal cancer index (PCI) (32), the Completeness of Cytoreduction (CC) score (32), the duration of surgery, blood transfusion, estimated blood loss, and intraperitoneal chemotherapy regimens (chemotherapeutics of HIPEC and EPIC) were collected.
The postoperative information included tumor characteristics (origin, histology, and tumor markers), the incidence of acute kidney injury within 7 days (defined according to the KDIGO criteria) (33), and major complications within 30 days postoperative (classified as grade 3 or greater according to the Clavien-Dindo classification) (34). Histology of PMP was classified according to the 2016 Peritoneal Surface Oncology Group International consensus (35).
The intraoperative data were collected from the anesthesia information management system, including the volumes of artificial colloid and crystalloid infusion, mean arterial pressure (MAP), and core body temperature. Invasive MAP data were captured and stored at 30-seconds or 5-minutes intervals, and nasopharyngeal temperature data at a 5-min interval throughout the whole CRS-HIPEC procedure.
Postoperative follow-up information included postoperative computed tomography scans of the abdomen and pelvis), subsequent therapies for PMP, re-hospitalizations (with reasons and treatments), and patient survival status (with death dates confirmed against death certificates). The follow-up was censored at November 9, 2021. The data were from the medical charts including outpatient interviews or telephone interviews, following a schedule of every 3–6 months in the first 5 years post-surgery and then annually. For patients lost to follow-up, the date of the last hospital visit post-surgery was recorded as the censoring time.
Outcomes
2.4
The primary outcome was the overall survival (OS), defined as the interval from surgery to the date of death. The secondary outcome was event-free survival (EFS), defined as the interval from surgery to the date of PMP recurrence (for patients who achieved CC-0/1) or progression (for patients who achieved CC-2/3) (7), unplanned re-hospitalization for non-PMP diseases, or death, whichever occurred first. PMP recurrence/progression was defined as the reappearance/progression of the same local-regional peritoneal disease, on the evidence of computed tomography scans of the abdomen and pelvis.
Sample size
2.5
Owing to the rarity of this disease, the sample size was not calculated beforehand. We screened all the available patients during the study period in our center.
Statistical analysis
2.6
In order to reflect the fluctuation of MAP, the area under thresholds (AUT) of <MAP 75, 70, and 65 mmHg was calculated, respectively. The area under a specialized threshold was calculated by summarizing all areas (a_1_ + a_2_ + a_3_…) above the curve below the given thresholds. Each area was calculated according to the trapezoid rule and linear interpolation between adjacent measurements. As sensitive analyses, we also calculated the area above thresholds of nasopharyngeal temperature >38.0, 37.5, and 37 °C. All calculations were performed using the Python 3.10 software.
All analyses were performed using SPSS 27.0 (IBM SPSS, Armonk, NY, USA). The continuous data were presented as means ± standard deviations (SDs) for normally distributed data and as medians [interquartile ranges (IQRs)] for non-normally distributed data (according to the Kolmogorov–Smirnov test). The categorical data were presented as n (%). Pre-/perioperative variables, along with AUT of MAP, were explored for associations with OS and EFS using a univariable Cox proportional hazards regression model. The variables with P < 0.20 in the univariable analyses and AUT of MAP < 65 mmHg were included in a multivariable Cox proportional hazards regression model. Two-sided P values <0.05 were deemed statistically significant. Sensitivity analyses were performed after excluding patients missing intraoperative temperature data.
Results
3
The study screened 782 PMP patients undergoing CRS-HIPEC. Patients were excluded for the following reasons: 60 cases with non-confirmatory PMP diagnosis, 57 cases with non-appendiceal origins, 47 cases having multiple procedures, 7 cases missing MAP data, and 179 cases with intestinal contraction, leaving 432 patients for the final analyses (Figure 1).
Study flowchart. CRS-HIPEC: combination of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy.
In this cohort, 65.0% (281/432) were female, with mean age 57 ± 11 years (Table 1). Complete cytoreduction was achieved in 222 patients (51.4%), including 102 cases with CC-0 and 120 cases with CC-1. Intraperitoneal chemotherapy was administered as HIPEC alone (24.5%, n = 106) or HIPEC + EPIC (75.5%, n = 326). Intraoperative hypotension was ubiquitous: 431 (99.8%) patients experienced MAP < 75 mmHg, 427 (98.8%) patients MAP < 70 mmHg, and 405 (93.8%) patients MAP < 65 mmHg (Table 2 and Supplementary Table S5).
With 40-month median follow-up (IQR 25, 55), cumulative mortality was 21.8% (94/432) and event incidence was 32.4% (140/432). Readmissions for PMP occurred in 29.9% (129/432) vs. 57.2% (247/432) for planned interventions. Median survival durations were 56 (95% confidence interval [95% CI]: 50, 61) months for OS and 45 (95% CI: 40, 51) months for EFS (Table 3).
Univariable analyses identified 24 candidate factors with P < 0.20 (Tables 1, 2) those associated with survival. After excluding factors that had correlation with others, 18 factors including AUT of MAP < 65 mmHg were included in the multivariable regression model. The multivariable analysis revealed that preoperative raised tumor markers (hazard ratio [HR] = 4.90–10.20; 95% CI: 1.11–46.67; P < 0.05), CC-score (HR = 3.37–9.41; 95% CI: 1.05–16.37; P < 0.05), and high-grade PMP (HR = 1.80; 95% CI: 1.10, 2.93; P = 0.019) were independently associated with OS. Similarly, the multivariable analysis identified that preoperative raised tumor markers (HR = 2.92–5.97; 95% CI: 1.15–16.07; P < 0.05), CC-score (HR = 1.87–4.24; 95% CI: 0.89–9.57; P < 0.05), and high-grade PMP (HR = 1.93; 95% CI: 1.15, 2.80; P = 0.022) were independently associated with EFS; otherwise, preoperative Barthel index (HR = 0.86; 95% CI: 0.74, 0.98; P = 0.019) was found to be associated with EFS (Table 4). Intraoperative hypotension was not associated with both OS and EFS.
Sensitivity analyses in 294 cases with intraoperative temperature did not change our results. All raised tumor markers (HR = 10.32; 95% CI: 2.13, 50.02; P = 0.004), the CC-score (HR = 3.18–11.22; 95% CI: 1.12–29.41; P < 0.05), and high-grade PMP (HR = 2.72; 95% CI: 1.88, 3.75; P = 0.005) remained associated with OS; Barthel index (HR = 0.87; 95% CI: 0.74, 0.92; P = 0.042), preoperative 2 or 3 raised tumor markers (HR = 4.86–7.54; 95% CI: 1.45–24.97; P < 0.05), CC-score (HR = 3.42–4.77; 95% CI: 1.54–8.91; P < 0.05), and high-grade PMP (HR = 2.88; 95% CI: 1.52, 3.37; P = 0.004) remained associated with EFS; both intraoperative hypotension and intraoperative hyperthermia were not associated with OS or EFS (Supplementary Tables S1–S4).
Discussion
4
After CRS-HIPEC, preoperative tumor marker levels, Barthel index, CC-score, and PMP histology were independently associated with OS or EFS in patients with PMP from mucinous appendix neoplasms. The results may help improve the perioperative management of patients with PMP.
After a median follow-up of 40 months, the median OS was 56 (95% CI: 50, 61) months and the median EFS was 45 (95% CI: 40, 51) months in our study, shorter than other authors from China previous reported (12). That might be due to the different characteristics between the cohort patients: the PCI scores of our patients (75.7% of the patients with PCI ≥11) were much higher compared with the study from Yan et al. (52.8% of the patients with PCI >12) (12).
Of note, only 51.4% of our patients achieved complete cytoreduction (CC-0/1), substantially lower than the 66% to 93% reported by authors from other regions (36, 37). It was easily to be explained as following: firstly, a significant proportion (72.2% patients with PSS 0–2) of the patients came to our institution for CRS-HIPEC after unsuccessful previous surgical interventions; secondly, nearly half of the patients awaited professional CRS-HIPEC for more than 6 months from diagnosis; thirdly, factors such as higher PCI, male gender, and high pathological grade could also decrease the likelihood of complete cytoreduction (38).
Unsurprisingly, consistent with the other studies (7, 8, 10, 37, 39), our study also identified CC-score and PMP pathology associated with OS and EFS. Complete cytoreduction is probably the strongest prognostic factor in PMP by reducing the negative prognostic impact of histological grade (10, 38). And consistent with our result, many studies have showed that an increase in one or more of tumor markers was associated with poorer prognosis in PMP patients (13, 40).
In this study, a lower Barthel index weas found to be associated with a poorer EFS. Usually, a patient with lower Barthel index had a worse function status, with more comorbidities and a poorer health status, consequently more frequent postoperative complications (41) and even shorter survival (42).
93.8% of our patients experienced hypotension (MAP < 65 mmHg) during CRS-HIPEC, but it was not associated with OS and EFS in PMP patients. This raises concern regarding the special significance and innovation of this retrospective study. However, accumulating evidence showed that intraoperative blood pressure management was associated with long-term survival (23–26). Nearly all our patients experienced hypotension, which might limit the power of the statistical analyses. In addition, hypotension with different underlying pathophysiological causes might have different effects on organ perfusion and outcomes. Hemodynamic changes during HIPEC are complex due to heat stress, including increased cardiac output and heart rate, decreased stroke volume, MAP, and systemic vascular resistance (43). As we known, organ perfusion is proportional to the perfusion pressure and inversely proportional to the local vascular resistance. Depending on the relative extent of the changes in local vascular resistance compared to perfusion pressure, organ perfusion might remain stable or even increase, irrespective of decreased MAP, thereby leading to different effects on surgical outcomes (44). More studies are warranted to explore the relationship between intraoperative blood pressure management and long-term outcomes in PMP patients undergoing CRS-HIPEC.
The strength of this study was that the patients were from a single center, minimizing potential bias due to differences in local practice among hospitals. In addition, the study center is specialized in CRS-HIPEC. A French multicenter study of 301 patients with PMP showed that centers with less experience had poorer survival results (10). Still, this study also had limitations. The retrospective study design inherently limited data collection to information documented in medical records, and data such as primary tumor histology and prior chemotherapy were not recorded in detail. Furthermore, this study did not find significant associations between intraoperative hypotension/hyperthermia and OS/EFS. Notably, important factors including cardiac output, vascular resistance, and intraoperative hypotension interventions were not be analyzed. Although it was declared as a strength, the single-center nature of the study also limits generalizability because of the local protocols. Because CRS-HIPEC for PMP is standard in our center, no contemporary control group could be included. These shortcomings highlighted the critical need for multicentric studies with larger size and control groups to corroborate and broaden the insights into the prognostic factors for both short- and long-term outcomes in PMP.
Conclusions
5
After CRS-HIPEC, preoperative tumor marker levels, Barthel Index, CC-score, and PMP histology were independently associated with OS or EFS; intraoperative hypotension and hyperthermia were not associated with both OS and EFS.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Feng JN Hu AJ Xu L Liu LL Liu GZ Wang JX Prevalence and incidence of pseudomyxoma peritonei in urban China: a nationwide retrospective cohort study. Eur J Surg Oncol. (2022) 48(10):2226–32. 10.1016/j.ejso.2022.06.01335764460 · doi ↗ · pubmed ↗
- 2Patrick-Brown T Carr NJ Swanson DM Larsen S Mohamed F Flatmark K. Estimating the prevalence of pseudomyxoma Peritonei in Europe using a novel statistical method. Ann Surg Oncol. (2021) 28(1):252–7. 10.1245/s 10434-020-08655-832488520 PMC 7752784 · doi ↗ · pubmed ↗
- 3Moran BJ Cecil TD. The etiology, clinical presentation, and management of pseudomyxoma peritonei. Surg Oncol Clin N Am. (2003) 12(3):585–603. 10.1016/S 1055-3207(03)00026-714567019 · doi ↗ · pubmed ↗
- 4Memon AA Godbole C Cecil T Dayal S Moran B Tzivanakis A Overall survival is more closely associated with peritoneal than primary appendiceal pathological grade in pseudomyxoma Peritonei with discordant pathology. Ann Surg Oncol. (2022) 29(4):2607–13. 10.1245/s 10434-021-10994-z 34731401 · doi ↗ · pubmed ↗
- 5Govaerts K Lurvink RJ De Hingh I Van der Speeten K Villeneuve L Kusamura S Appendiceal tumours and pseudomyxoma peritonei: literature review with PSOGI/EURACAN clinical practice guidelines for diagnosis and treatment. Eur J Surg Oncol. (2021) 47(1):11–35. 10.1016/j.ejso.2020.02.01232199769 · doi ↗ · pubmed ↗
- 6Li XB Ma R Ji ZH Lin YL Zhang J Yang ZR Perioperative safety after cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy for pseudomyxoma peritonei from appendiceal origin: experience on 254 patients from a single center. Eur J Surg Oncol. (2020) 46(4 Pt A):600–6. 10.1016/j.ejso.2020.01.01731973925 · doi ↗ · pubmed ↗
- 7Chua TC Moran BJ Sugarbaker PH Levine EA Glehen O Gilly FN Early- and long-term outcome data of patients with pseudomyxoma peritonei from appendiceal origin treated by a strategy of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. J Clin Oncol. (2012) 30(20):2449–56. 10.1200/JCO.2011.39.716622614976 · doi ↗ · pubmed ↗
- 8Ansari N Chandrakumaran K Dayal S Mohamed F Cecil TD Moran BJ. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy in 1000 patients with perforated appendiceal epithelial tumours. Eur J Surg Oncol. (2016) 42(7):1035–41. 10.1016/j.ejso.2016.03.01727132072 · doi ↗ · pubmed ↗