Maternity continuum of care and associated factors among mothers in south Ethiopia: a community-based cross-sectional study
Leweyehu Alemaw Mengstie, Bethelehem Taye Mengistu, Fekadu Bekele, Wondimagegn Paulos Kumma, Biruk Tesfahun, Yihenew Ayehu Dessie, Wegayehu Zeneb Teklehaimanot, Amanuel Eshetu, Bekahegn Girma, Solomon Abreha, Mohammed Tesema Gebeyehu, Worku Abemie

TL;DR
This study finds that only 23.7% of mothers in south Ethiopia completed the maternity care continuum, with education, access, and awareness being key factors.
Contribution
The study identifies specific factors associated with maternity care continuity in a low-income Ethiopian setting.
Findings
Only 23.7% of mothers completed the maternity continuum of care.
Secondary education and shorter travel times to health facilities were strongly associated with care completion.
Family planning use and awareness of postpartum complications also significantly influenced care continuity.
Abstract
The maternity continuum of care (CoC) is crucial for improving maternal and neonatal health outcomes. Despite global initiatives like the SDGs and Every Woman Every Child, maternal health gaps remain in LMICs, especially sub-Saharan Africa, including Ethiopia. This study aims to assess the level of maternity CoC and identify factors associated with its utilization among mothers in Ethiopia. A community-based cross-sectional study was conducted between January 15 and February 15, 2024, using a random sample of 564 mothers. Data were collected using a pretested structured questionnaire. Data was entered by EpiData 4.6 and analyzed with SPSS 25. Bi-variable and multivariable logistic regression identified associations, reported with adjusted odds ratios and 95% confidence intervals, with p-values <0.05 indicating significance. Only 23.7% (95% CI: 19.6–27.6) of women completed the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
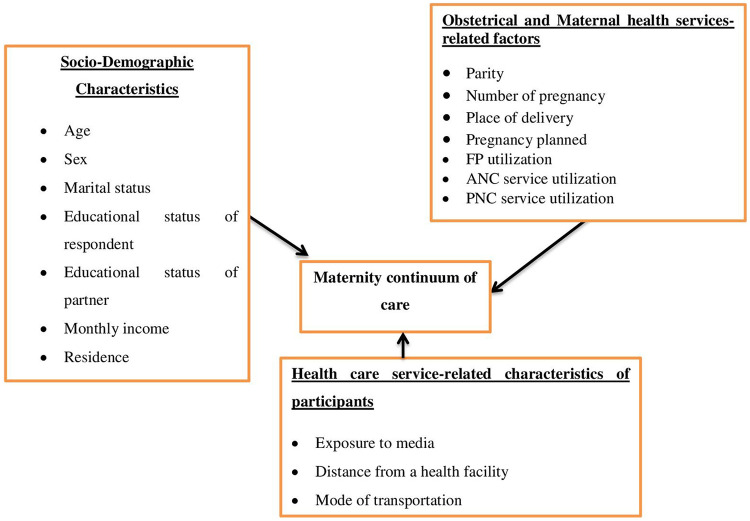 Figure 1
Figure 1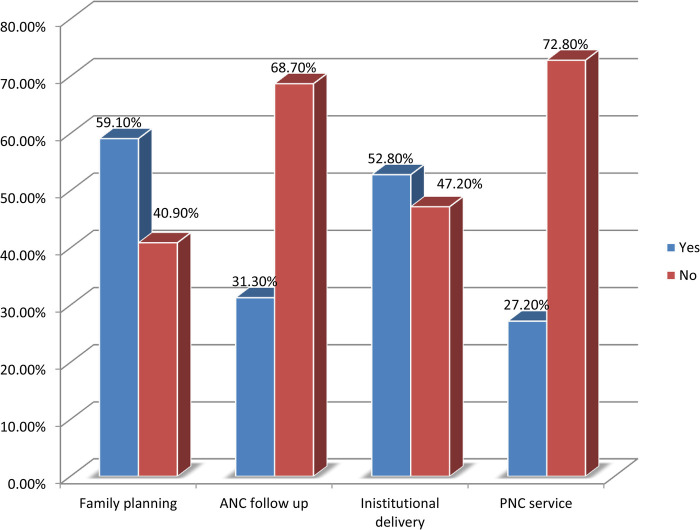 Figure 2
Figure 2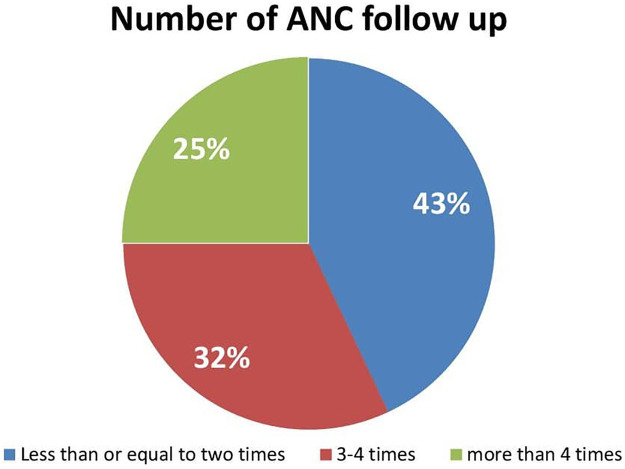 Figure 3
Figure 3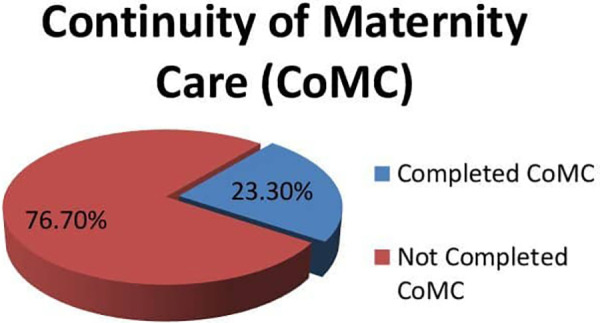 Figure 4
Figure 4| Variable | Category | Frequency | Percent |
|---|---|---|---|
| Age of Respondents | 15–19 | 0 | 0.0 |
| 20–24 | 29 | 5.9 | |
| 25–29 | 171 | 35 | |
| 30–34 | 203 | 41.5 | |
| ≥35 | 86 | 17.6 | |
| Educational status of a mother | Unable to read and write | 148 | 30.3 |
| Able to read and write | 116 | 23.7 | |
| Completed primary school | 86 | 17.6 | |
| Completed secondary | 72 | 13.7 | |
| Diploma/above | 67 | 14.7 | |
| Educational status of partner | Unable to read and write | 146 | 29.9 |
| Able to read and write | 80 | 16.4 | |
| Completed primary school | 109 | 22.3 | |
| Completed secondary | 104 | 21.3 | |
| Diploma and above | 50 | 10.0 | |
| Marital status of respondents | Married | 486 | 99.4 |
| Divorced | 0 | 0 | |
| Widowed | 3 | 0.6 | |
| Occupation of respondents | Housewife | 196 | 40.1 |
| Merchant | 119 | 24.3 | |
| Government employee | 124 | 25.4 | |
| Private employee | 50 | 10.2 | |
| Occupation of partners | Farmer | 292 | 59.7 |
| Merchant | 165 | 33.7 | |
| Government employee | 18 | 3.7 | |
| Private employee | 14 | 3.9 | |
| Family size | ≤5 | 435 | 89 |
| >5 | 54 | 11 | |
| Distance from health institution | ≤30 min | 180 | 36.8 |
| >30 min but <1 h | 190 | 38.9 | |
| ≥1 h | 119 | 24.3 |
| Variable | Category | Frequency | Percent |
|---|---|---|---|
| Number of pregnancy | Less than or equal to two | 205 | 41.92 |
| 3–4 pregnancy | 238 | 56.24 | |
| ≥4 pregnancy | 9 | 1.86 | |
| Number of live birth | ≤2 birth | 198 | 40.5 |
| 3–4 birth | 269 | 55.0 | |
| >4 birth | 9 | 1.8 | |
| Pregnancy planned | Yes | 483 | 98.8 |
| No | 6 | 1.2 |
| Variables | Completed
CoMC | Not completed
CoMC | COR [95% CI] | AOR [95% CI] | ||
|---|---|---|---|---|---|---|
| Residence | ||||||
| Urban | 13 (36.11%) | 23 (33.89%) | 0.073 | 1.92 [0.94–3.93]** | ||
| Rural | 103 (22.74%) | 350 (77.26%) | 1 | 1 | ||
| Maternal educational status | ||||||
| Can’t read and write | 25 (16.89%) | 123 (83.11%) | 1 | 1 | 1 | 1 |
| Can read and write | 22 (18.97%) | 94 (87.03%) | 0.662 | 1.15 [0.61–2.17] | 0.805 | 1.10 [0.52–2.32] |
| Completed primary school | 19 (22.09%) | 67 (77.91%) | 0.327 | 1.39 [0.72–2.72] | 0.320 | 1.46 [0.69–3.12] |
| Completed secondary school | 21 (29.17%) | 51 (70.83%) | 0.038 | 2.03 [1.04–3.94]** | 0.023 | 2.46 [1.13–5.37] |
| Diploma and above | 29 (43.28%) | 38 (56.72%) | <0.000 | 3.76 [1.97–7.17]** | <0.001 | 5.78 [2.63–12.76] |
| Occupation of respondent | ||||||
| Housewife | 46 (23.47%) | 150 (76.53%) | 1 | 1 | ||
| Merchant | 24 (20.17%) | 95 (79.83%) | 0.495 | 0.824 [0.47–1.44] | ||
| Private employee | 30 (24.19%) | 94 (75.81%) | 0.882 | 1.04 [0.61–1.76] | ||
| Government employee | 16 (32%) | 34 (68%) | 0.217 | 1.54 [0.78–3.03]** | ||
| Distance from health facility | ||||||
| ≤30 min | 68 (37.78%) | 112 (62.22%) | 1 | 1 | <0.001 | 3.71 [1.818–7.57] |
| >30 min but <1 h | 31 (16.32%) | 159 (83.68%) | <0.001 | 3.64 [2.01–6.61]** | 0.357 | 1.42 [0.67–2.99] |
| ≥1 h | 17 (14.29%) | 102 (85.71%) | 0.632 | 1.170 [0.62–2.22] | 1 | 1 |
| Family planning user | ||||||
| Yes | 97 (33.56%) | 192 (64.44%) | <0.001 | 4.81 [2.83–8.19]** | <0.001 | 5.13 [2.80–9.39] |
| No | 19 (9.5%) | 181 (90.5%) | 1 | 1 | 1 | 1 |
| Place of delivery | ||||||
| At health facility | 171 (66.28%) | 87 (33.72%) | <0.001 | 3.54 [2.22–5.65]** | <0.001 | 3.37 [1.97–5.76] |
| At home | 202 (87.45%) | 29 (12.55%) | 1 | 1 | 1 | |
| Counseled about post-partum complications | ||||||
| Yes | 95 (27.70%) | 248 (72.30%) | 0.002 | 2.28 [1.36–3.83]** | 0.003 | 2.49 [1.36–4.56] |
| No | 21 (14.38%) | 125 (85.62%) | 1 | 1 | 1 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Maternal and Child Health · Breastfeeding Practices and Influences · Maternal and Perinatal Health Interventions
Background
Continuity of maternity care is an essential program strategy that women have received as a continuation of care throughout the life cycle of pregnancy, childbirth, and postpartum periods and that supports the advancement of women's status and the neonatal health of these women in global health (1).
Globally, in 2020, the maternal mortality ratio was 152 deaths per 100,000 live births, slightly higher than 151 deaths in 2019. This trajectory further projects 133 deaths in 2030, nearly double the SDG target of 3.1 (2). In addition, in 2019, 2.4 million children died in their first month of life. Approximately 6,700 neonatal deaths occur every day. A third of deaths occur within the first 24 h of birth, and three-quarters (75%) occur in the first week of life (3).
In Ethiopia, the magnitude of the continuum of maternity care is 9.1%, according to a multi-level study from 2019 (4).
Studies suggest that a variety of factors influence how often women use different types of maternity healthcare services. Unwanted pregnancies, low educational status, being in the bottom quintile of wealth, not being exposed to the media, living in a rural area, traveling a greater distance to a health facility, being a farmer, starting ANC later than recommended, and not communicating with the husband or other family members were a few of these factors (5–7).
Promoting continuity of care throughout the lifecycle, including adolescence, pregnancy, childbirth, the postpartum period, and childhood, is crucial for maternal, infant, and child health. Continuum of care services helps reduce maternal, neonatal, and pediatric morbidity and mortality (4, 8).
There is currently an updated strategy called “cultivating the culture of completion of the maternity continuum of care,” which states that “each pregnant woman has four or more antenatal care (ANC) contacts, birth is attended by skilled health personnel, and receives early routine postnatal care within two days,” as this will determine the future of women's, neonates', and children's health and lives by 2030 (9).
Despite progress in maternal and child health in South Ethiopia, gaps in the continuum of maternity care persist. Most studies focus on antenatal, intrapartum, or postnatal care separately, lacking a comprehensive approach to coordinated, uninterrupted care from pre-pregnancy to the postnatal period. This study addresses this gap by investigating the factors influencing the seamless provision of maternity care, offering insights to improve maternal and neonatal health outcomes in South Ethiopia.
Methods
Study setting, design, and period
A community-based cross-sectional study design was conducted from January 15 to February 15, 2024. The study was conducted in the Damot Gale woreda, Wolaita Zone, South Ethiopia. Currently, there are 29 kebeles in Damot Gale Woreda. Based on the data reported from the Woreda health office, the total population was around 143,720 of those 70,423 were male, with 28,836 households. From the report of Damot Gale Woreda health office, there were 4,836 pregnant women with the first visit of antenatal care, 4,786 women delivered at the health facility and 4,131 women had post-partum care (both health facility delivery and home delivery).
Population
All mothers in the Damot Gale woreda, Wolaita Zone, South Ethiopia who gave birth within 1 year before data collection were considered the source population.
Selected Mothers gave birth in the last year preceding this study in Gale woreda, Wolaita Zone, South Ethiopia were the study populations.
Inclusion and exclusion criteria
All mothers who gave birth in the past year in Damot Gale Woreda were included. Moreover, all mothers who gave birth in another district and came to the study area and mothers critically ill and unable to respond to the interview were excluded from the study.
Sample size and sampling techniques
The sample size is calculated by using a single population proportion formula assuming that the prevalence of maternity continuum of care is 37.2% (10), a 5% marginal error with 95% confidence level, then the sample size is 358, by adding 5% of non-response rate and 1.5 design effect, the final sample size was 562.
The study included 8 Kebeles, chosen by a lottery method (simple random sampling) from 29 Kebeles. Study subjects were allotted to each Kebeles and selected using simple random sampling until the required sample size was met.
Operational definition
Completion of maternity continuum of care: magnitude of maternity continuum of care was defined as whether a post-partum period woman having one or more ANC visits at the health facility during pregnancy, childbirth aided by SBA (doctor, nurse, and midwife, health officer, and health extension worker), and having one or more PNC for the mothers within 6 weeks after viable childbirth based on self-reports (11).
Completion of Continuum of Care (CoC): It is defined by the completion of all recommended ANC visits (at least 4 ANC), institutional delivery (ID), and PNC services. A woman is said to have completed CoC, coded as “1” if she received all mentioned services, and incomplete CoC, coded as “0”, if she missed at least one of the recommended services. This outcome was used to see the effect of the place of the first ANC visit on the continuum of care (12).
Study variables
Dependent variables
Completion of the Maternity Continuum of Care.
Independent variables
Socio-demographic characteristics.
Healthcare service-related factors.
Obstetrical related factors.
Maternal health care service-related factors (Figure 1).
Conceptual frame work for factors associated with continuity of maternal care mothers in Damot Gale Wored Wolaiata Zone south Ethiopia, 2024.
Data collection and quality control
Data were collected using a structured interviewer-administered questionnaire developed from the different literature (1–14).
The questionnaire was initially prepared in English, then translated into Wolaytegna (the local language), and back-translated to English to ensure accuracy. The final version was in Wolaytegna for clarity and ease of understanding. Four data collectors (two midwives and two nurses) and two supervisors were recruited for data collection. They received 1 day of training. Principal investigators and supervisors reviewed the collected data daily for completeness and consistency.
Data processing and analysis
Data was cleaned, coded, and entered into Epidata version 4.6, then analyzed using SPSS version 25. Categorical variables were presented with frequency tables, percentages, pie charts, or bar graphs, while continuous variables were summarized using mean and standard deviation. The hosmer and lemeshow test assessed model fit, and variance inflation factors (VIF) checked for multicollinearity. Bi-variable logistic regression identified variables with p-values <0.25 for the final analysis. In the last model, variables with p-values <0.05 were deemed significant. Associations were reported using adjusted odds ratios (AORs) with 95% confidence intervals.
Results
Socio-demographic characteristics
Out of the 562 samples, 489 mothers participated in the interview, resulting in an 87% response rate. The study found that the average age of respondents was 30.39, with a standard deviation of ±4.07. Out of the respondents, 453 individuals (92.6%) were classified as rural residents. Approximately 148 (30.3%) of mothers and 146 (29.9%) of partners lacked literacy skills. About 196 (40.1%) of mothers were stay-at-home parents and 292 (59.7%) of partners were farmers (Table 1).
Maternal healthcare service utilization
All respondents have heard about maternal health care (MCH) service and about 289 (59.1%) of respondents use at least one family planning method. About one third 153 (31.3%) of mothers have had attended ANC follow-up at least once for their recent child, almost half 258 (52.8%), and 133 (27.2%) of mothers gave birth at health institutions and have got postnatal care (Figure 2).
Maternal health care service utilization of the respondents and their partners in Damot Gale Woreda, Wolaita South, Ethiopia, 2024 (N = 489).
Of the total mothers who have had ANC follow up only about one-fourth 38 (25%) followed more than four times (Figure 3).
Number of ANC follow up of the respondents in Damot Gale Woreda, Wolaita South, Ethiopia, 2024 (N = 489).
Obstetric-related characteristics
Of all the study participants, approximately 58 (11.9%) reported that this was their first pregnancy, while about half, 238 (48.7%), were experiencing their third pregnancy. Nearly all, 483 (98.8%), indicated that the pregnancy was planned, and around 269 (55%) of the mothers had three to four live births (Table 2).
Magnitude of continuity of maternity care
Of the total respondents who participated in the study, about 116 (23.7%, 95% CI, 19.6%–27.6%) mothers have completed their continuity of care, whereas the remaining 373 (76.3, 95% CI, 72.4%–78.4%) respondents haven't completed their care (Figure 4).
Continuity of maternity care among respondents in Damot Gale Woreda, Wolaita South, Ethiopia, 2024 (N = 489).
Factors associated with maternity continuum of care
Variables with a p-value of <0.25 in bi-variable logistic regression were candidate variables for the multi-variable logistic regression analysis model. Educational status (completing secondary school and above), time to reach the health facility (less than or equal to 30 min), family planning service utilization, giving birth at a health facility, and counseling about post-partum complications were significantly associated with continuity of maternity care.
Mothers who attended secondary school had 2.46 times higher odds of completing the continuity of maternity care (AOR = 2.46, 95% CI: 1.13–5.37) compared to mothers who could not read or write. Additionally, mothers with above secondary and above education had 3.76 times higher odds of completing the continuity of maternity care (AOR = 5.78, 95% CI: 2.63–12.76) compared to illiterate mothers. Moreover, mothers who took less than 30 min to reach the nearest health institution had 3.71 times higher odds of completing the continuity of maternity care (AOR = 3.71, 95% CI: 1.818–7.57) compared to their illiterate counterparts (Table 3).
Discussion
The study found that the overall completing continuity of maternal care was 23.7% [95% CI, 19.6%–27.6%)], this is comparable with a study conducted in North West Ethiopia at 21.6% (1), a systematic review and meta-analysis conducted in Ethiopia 25.5% (13), Pakistan 27% (15). But, lower than studies reported in some other studies, Debre Berhan 37.2% (10), North West Ethiopia reported completion rates of 37.6% (16, 17), 47% (18), Cambodia (60%) (19) and Egypt (50.4%) (20), and a study in Ghana reported a significantly higher rate of 66% (21).
However, the completion rate observed in this study is higher than those reported in other regions, North East Ethiopia, the completion rate was 11.2% (14), in Arbaminch, it was 9.7% (22), and in Ethiopian Demographic and Health Survey (EDHS) reported a national rate of 6.56% (23), and studies conducted in Ghana found completion rates of 8% a (24).
The disparities in these findings can be attributed to variations in healthcare infrastructure, effective maternal health programs, and higher levels of maternal awareness and education.
According to this study educational status was positively associated with continuity of maternal care which means more educated mothers are more likely to complete continuity of maternal care. Multiple studies conducted worldwide, including our country (2, 25, 26), support this claim. The scientific justification for this is that education enhances health literacy, enabling women to comprehend the benefits of regular healthcare visits and adherence to medical advice (18).
Moreover, mothers who use family planning services were more likely to complete continuity of maternal care compared to their counterparts. This is supported by a study conducted in South Wollo (27), North East Ethiopia (28), and Arbaminch (22). This might be because mothers who use family planning services have a chance to be counseled about ANC, delivery, and PNC services. Due to this may encouraged to complete the continuity of care.
This finding also found that mothers who were near health institutions were more likely to compete for continuity of maternal care compared to mothers who were far away from the health institutions. This finding is consistent with studies conducted in North West Ethiopia (18), North East Ethiopia (27), Gambia (29), and a study conducted in Gahanna (21).
This study also revealed that there is an association between completing continuity of maternal care and giving birth at a health institution as well as being counseled about post-partum complications. This is due to scientifically, counseling increases knowledge and preparedness, reducing the risk of complications (16).
Strength and limitation
This community-based study, with a large sample size and three home visits, improved response rates. However, recall and social desirability biases may have affected data accuracy.
Conclusion
The magnitude of completing continuity of maternal care is higher compared to the EDHS report. Significant factors associated with continuity of maternal care include maternal educational status (completing secondary school and obtaining a diploma or higher), using family planning services, giving birth at a health institution, living within 30 min of a health facility, and receiving counseling about post-partum complications.
Therefore, health leaders, policymakers, and all stakeholders should prioritize the continuity of maternal care when providing various services to mothers. Enhancing family planning service utilization, ensuring health facility deliveries, and offering counseling during service provision should be considered to improve the continuity of maternal care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tsega D Admas M Talie A Tsega TB Birhanu MY Alemu S Maternity continuum care completion and its associated factors in northwest Ethiopia. J Pregnancy. (2022) 2022:1309881. 10.1155/2022/130988135223099 PMC 8872697 · doi ↗ · pubmed ↗
- 2Mihret MS Alemu K Beshah DT Gezie LD Erlandsson K Lindgren H. Challenges of maternity continuum of care within the primary health care in northwest Ethiopia: interpretive description using a socio-ecological model. Front Public Health. (2024) 12:1401988. 10.3389/fpubh.2024.140198839722709 PMC 11668779 · doi ↗ · pubmed ↗
- 3UNICEF DATA. UNICEF DATA. Available online at: https://data.unicef.org/topic/child-survival/neonatal-mortality/ (Accessed November 29, 2021).
- 4Chaka EE Parsaeian M Majdzadeh R. Factors associated with the completion of the continuum of care for maternal, newborn, and child health services in Ethiopia. Multilevel model analysis. Int J Prev Med. (2019) 10:136. 10.4103/ijpvm.IJPVM_26_1931516677 PMC 6711120 · doi ↗ · pubmed ↗
- 5Khan MN Harris ML Loxton D. Assessing the effect of pregnancy intention at conception on the continuum of care in maternal healthcare services use in Bangladesh: evidence from a nationally representative cross-sectional survey. P Lo S One. (2020) 15(11):e 0242729. 10.1371/journal.pone.024426433216799 PMC 7678970 · doi ↗ · pubmed ↗
- 6Enos JY Amoako RD Doku IK. Utilization, predictors and gaps in the continuum of care for maternal and newborn health in Ghana. Int J MCH AIDS. (2021) 10(1):98. 10.21106/ijma.42533614225 PMC 7880832 · doi ↗ · pubmed ↗
- 7Tamang TM. Factors associated with completion of continuum of care for maternal health in Nepal. IUSSP XXVIII International Population Conference; Cape Town, South Africa (2017).
- 8Kerber KJ de Graft-Johnson JE Bhutta ZA Okong P Starrs A Lawn JE. Continuum of care for maternal, newborn, and child health: from slogan to service delivery. Lancet. (2007) 370(9595):1358–69. 10.1016/S 0140-6736(07)61578-517933651 · doi ↗ · pubmed ↗