Outcomes of Bovine Jugular Vein Versus Porcine Valved Conduits for Right Ventricle to Pulmonary Artery Connection
Bahar Temur, Ibrahim Gokce, Yakup Tire, Zeynep Sila Ozcan, Selim Aydin, Tugcin Bora Polat, Ersin Erek

TL;DR
This study compares bovine and porcine conduits for heart surgery in children, finding better survival and fewer reinterventions with the bovine option.
Contribution
The study provides new comparative evidence on the long-term outcomes of two xenograft conduits used in right ventricle to pulmonary artery connections.
Findings
Contegra (bovine) conduits showed significantly higher 10-year survival rates (90% vs. 33.9%) compared to Biointegral (porcine) conduits.
Fewer reinterventions were needed with Contegra conduits (30.5% overall vs. 33.3% in Biointegral group).
Contegra conduits demonstrated superior freedom from reintervention at 10 years (47.1% vs. 0% in Biointegral).
Abstract
Homografts conduits has been the gold standard for right ventricle to pulmonary artery (RV-PA) conduit. Several different types of xenograft valved conduits have been used as an alternative to homografts, due to their limited availability. In this single center, retrospective study, we analyzed the outcomes of patients with bovine jugular vein conduit (Contegra) and porcine valved conduit (Biointegral) in terms of survival and reintervention rate. Between 2012 and 2023, 44 children underwent surgical repair with RV-PA conduits using Contegra (n = 20) or Biointegral (n = 24). Patients with truncus arteriosus and patients who underwent unifocalization and Ross procedures were excluded. The operations in which other RV-PA conduits such as homografts, Gore-Tex grafts with PTFE handmade valved were used, were also excluded from the study. The median age of the patients was 19 (3–60) months…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
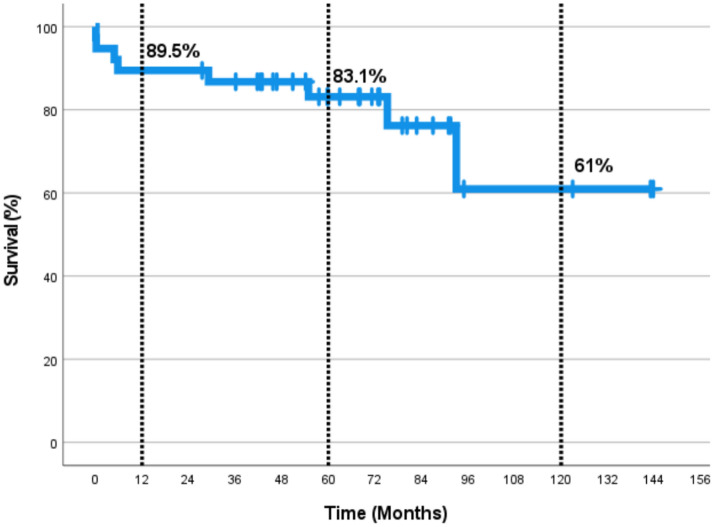 Figure 1
Figure 1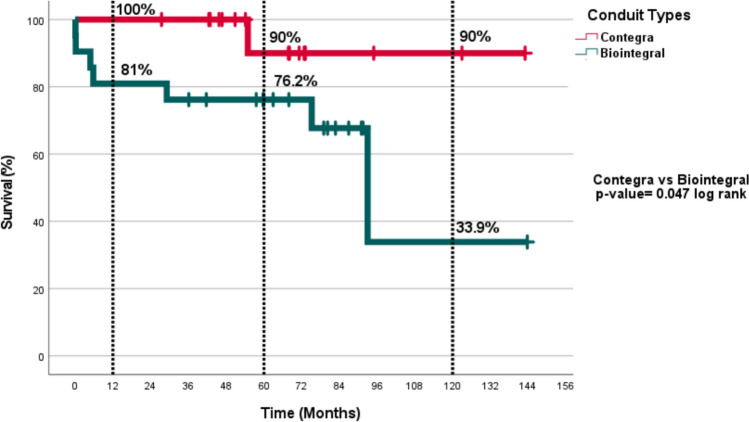 Figure 2
Figure 2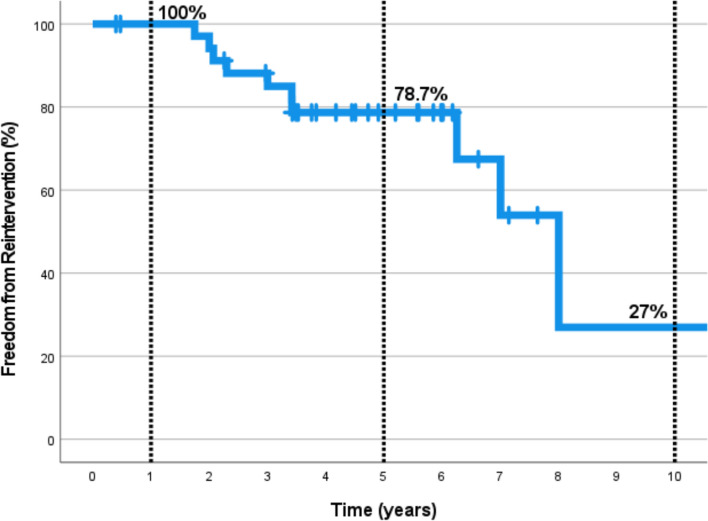 Figure 3
Figure 3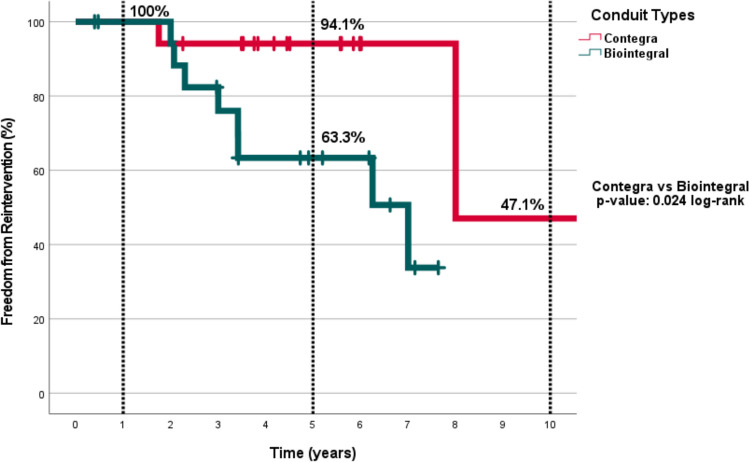 Figure 4
Figure 4- —Acibadem Mehmet Ali Aydinlar University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Heart Disease Studies · Mechanical Circulatory Support Devices · Vascular anomalies and interventions
Introduction
Right ventricle to pulmonary artery (RV-PA) valved conduits are necessary for right ventricular outflow tract (RVOT) reconstruction of some congenital heart anomalies. Homografts, harvested from the human pulmonary artery have been the gold standard as a RV-PA conduit ever since its inception in 1966 [1, 2]. Several different types of xenograft valved conduits are used as an alternative to homografts due to their limited availability [3, 4]. The most common xenograft conduits are bovine jugular vein (Contegra; Medtronic Inc, Minneapolis, Minn) and porcine (Biointegral; Biointegral Surgical Inc, Ontario, Canada) pulmonary valved conduits. Contegra is a natural valved conduit, treated with glutaraldehide whereas Biointegral has a porcine semilunar valve, implanted in a porcine pericardial tube graft treated with No-React technology [5]. Both conduits are available in a wide range of sizes (Contegra: 12–22 mm; Biointegral 15–31 mm) and their accessibility is the main advantage of them. No currently available valved conduit option is optimal and all patients with a conduit may need reinterventions at multiple times throughout their lifetime, not only due to a lack of growth potential, but also degeneration and calcification [6, 7]. Reinterventions whether surgical or catheter based, may cause mortality or morbidity. Apart from these, conduit failure itself, either conduit stenosis or valvular insufficiency may cause right ventricle dysfunction, dilatation, hypertrophy, tricuspid valve insufficiency, arrhythmias, and even sudden death [8].
Contegra was introduced to the market in 1999. Since then a lot of promising reports about it have been published. Some comparative studies have delineated similar mid- to long-term results for homografts and Contegra. Nevertheless, stenosis in distal anastomosis, aneurysmal dilatation when exposure to high pressure and a high rate of valvular insufficiency are some drawbacks of Contegra [9, 10]. Although porcine valves have been used for years in cardiac surgery in aortic, mitral or tricuspid valve replacements, reports about mid- to long-term performance of Biointegral pulmonary conduits are very limited. No studies to date have compared Biointegral pulmonary conduit with Contegra or homografts. Glutaraldehyde pretreatment of bioprosthetic heart valves is the major pathogenic factor for calcific degeneration [5]. Several pre-treatment methods are developed to abbreviate degeneration process. No-React process applied to the Biointegral conduit was developed by Biocar, Belo Horizonte, Brazil in 1996, for the purpose of delineating the merits of aldehyde detoxification process in preventing xenograft dystrophic calcification [5]. To date, there has been no convincing evidence for superiority or effectiveness of one method over the others.
In this single-center, retrospective study, we analyzed the outcomes of patients with Contegra or Biointegral pulmonary conduits in terms of survival and freedom from reintervention.
Materials and Methods
RV-PA conduits were implanted in 50 children during the repair of congenital heart defects between 2012 and 2023. Patients who underwent truncus arteriosus repair, unifocalization, Ross and Yasui procedures were excluded from the study for uniformity of the patients. Data- including medical histories of the patients, preoperative demographic characteristics, operative details, postoperative outcomes, and follow-up information - were retrieved from the institutional database retrospectively. All patients or their families were contacted by telephone and the patient’s history and functional class, as well as the last postoperative examinations such as echocardiography and angiography results, were obtained. Approval from the institutional ethics committee was taken before establishing the study (ATADEK 2023-21/742). RV-PA conduit types were Contegra in 20 cases (40%), Biointegral in 24 cases (48%), handmade ePTFE valved Gore-Tex graft in 3 cases (6%) and homograft in 3 cases (6%). The patients with handmade valved ePTFE conduits and homografts were also excluded from the study. The remaining 44 patients were divided into two groups according to the conduits used (Table 1).Table 1. Demographic parameters of the patientsGroup contegra (n = 20)Group biointegral (n = 24)p valueAge (months)(Median;min–max)19 (3–36)18.5 (10–60)0.687Female sex (%)6 (30)10 (41.7)0.428TGA-VSD-PS (%)4 (20)2 (8.3)0.387VSD-PA (%)16 (80)22 (91.7)Previous intervention (%)18 (90)19 (79.2)0.333Conduit size (median; min–max)18 (16–20)17 (13–21)0.671CPB time (mean ± SD)112 ± 21141 ± 670.311X Clamp time (mean ± SD)60 ± 1380 ± 360.069ICU time (median; min–max)5.5 (2–36)4.5 (2–63)0.600Hospital time (median; min–max)19.5 (5–63)18.5 (2–145)0.804Complications (%)4 (20)11 (45)0.075In-hospital mortality (%)0 (0)2 (8.3)0.191
The median age of the patients was 19 months (3–60 months). The diagnoses of the patients were transposition of the great arteries with ventricular septal defect and pulmonary stenosis (TGA-VSD-PS) in 6 patients (13.6%) and ventricular septal defect with pulmonary atresia (VSD-PA) in 38 patients (86.4%). A history of previous interventions were present in 37 patients (84%); systemic-to-pulmonary (S-P) shunt operation in 26 patients, ductal stenting in 4 patients, both ductal stenting and S-P shunt in 4 patients, pulmonary banding in 2 patients and RVOT stenting in 1 patient.
Surgical Technique
All operations were performed by means of a midline sternotomy using conventional cardiopulmonary bypass (CPB) with bicaval cannulation, intermittent tepid blood cardioplegia and moderate hypothermia. Any systemic-to-pulmonary artery shunts were ligated immediately after the initiation of CPB. VSD was closed to direct left ventricular blood flow to the aorta with a Dacron patch. RV-PA connection was reconstructed with a valved conduit. Pulmonary artery reconstruction if needed and distal conduit to pulmonary artery anastomoses were performed after aortic cross clamping while the heart was beating to reduce the ischemic myocardial period. The choice of conduit was based on the availability and cost.
Statistical Analysis
Continuous parameters are presented as median and range (minimum–maximum), while categorical parameters are shown as counts and percentages. All statistical analyses were performed using IBM SPSS Statistics software package 29.0. The Student’s t test was used for comparisons between different groups of normally distributed quantitative variables, and the Mann–Whitney U test was used to compare non-normally distributed quantitative variables between groups. Chi-square (χ^2^) test was used for the comparison of categorical variables between groups. Kaplan–Meier survival analysis was performed for the two conduit groups to assess 1-, 5-, and 10-year survival and freedom of reintervention. A *p-value of * < 0.05 was considered statistically significant.
Results
In-hospital mortality occured in two patients (4.5%). One of these patients underwent extracorporeal membrane oxygenation (ECMO) support due to an inability to wean from CPB. This patient died under ECMO support due to multiorgan failure. The other patient had a prolonged intensive care unit stay, underwent tracheostomy, and died of sepsis.
The mean cardiopulmonary bypass and aortic cross-clamp times were 128 ± 53 minutes and 71 ± 29 minutes, respectively. The median durations of intensive care unit and hospital stays were 5 days (2–63 days) and 19 days (2–145 days), respectively.
Postoperative complications were evaluated, and it was determined that 29 patients (66%) could be discharged without complications. The most common complications were as follows: four patients (9%) underwent postoperative re-exploration for bleeding; four patients (9%) required ECMO support; two patients (4.5%) required permanent pacemaker implantation; one patient (2.3%) experienced low cardiac output syndrome; and one patient (2.3%) had a postoperative stroke. Six patients (13.6%) required prolonged mechanical ventilation support and two patients (4.5%) underwent tracheostomy. Temporary dialysis was performed in four patients (9%). There was no statistically significant difference between the two groups in terms of postoperative complications (p = 0.075) (Table 1).Table 2. Follow-up dataReoperations/reinterventionsGroup Contegra (n = 17)%Group biointegral (n = 19)%Reoperations Conduit replacement15.9210.5Reinterventions Transcatheter pulmonary valve replacement15.9210.5 Conduit balloon angioplasty15.9315.8 Conduit stenting0015.3
Thirty-six patients were followed up for a median of 68 months (4.8–143.7 months). Six patients were lost to follow-up. There were six late deaths. Three of them were due to sudden cardiac arrest at home. One of these three patients had protein C deficiency and died as a result of acetylsalicylic acid-induced major bleeding. The other two had conduit failure and were awaiting intervention. The remaining three deaths were caused by cerebral ischemia following conduit re-replacement, pneumonia, and ventricular dysfunction. In the Kaplan–Meier survival analysis, the 1-, 5-, and 10-year survival rates for the entire population were 89.5%, 83.1%, and 61%, respectively (Fig. 1).Fig. 1. Actuarial survival of all population
The two in-hospital deaths in the entire population occured in the Biointegral group. There was one late death in the Contegra group and five late deaths in the Biointegral group. According to the Kaplan–Meier survival analysis, 1-, 5-, and 10-year survival rates for the Contegra and Biointegral groups were 100%, 90%, and 90%; and 81%, 76.2%, and 33.9%, respectively (Fig. 2). The difference in survival rates between the groups was statistically significant (p = 0.047).Fig. 2. Actuarial survival rates according to the conduit types
During the follow-up period, 11 patients (30.5%) required reintervention. All reinterventions were related to conduit or right-sided heart problems. The indication for reintervention of the RV-PA conduit was either stenosis or regurgitation leading to hemodynamic problems, symptoms, or reduced exercise capacity. Reintervention for stenosis was considered in the presence of any of the following: RV systolic pressure > 60–80 mmHg; progressive RV systolic dysfunction; RV/LV systolic pressure ratio > 0.66; RVOT gradient > 25 mmHg; decreased exercise capacity; or significant arrhythmias. Reintervention for regurgitation was considered in cases of significant pulmonary regurgitation with clinical symptoms (New York Heart Association [NYHA] class III or IV). In asymptomatic patients, reintervention was indicated by progressive right ventricle dilatation or dysfunction, new-onset arrythmias and the developement or progression of tricuspid valve regurgitation. If there is a risk for coronary compression in percutaneous pulmonary valve replacement or if conduit stenosis can not be relieved by high-pressure balloon angioplasty and subsequent stenting, then surgical reoperation is considered.
Three patients (8.3%) underwent conduit replacement while four patients (11%) underwent balloon angioplasty for the RV-PA conduit; three patients (8.3%) underwent transcatheter pulmonary valve replacement (TPVR), and one patient (2.7%) had conduit stenting. The procedures of reoperation and reintervention are summarized in Table 2. In the Kaplan–Meier analysis of freedom from reintervention , the 1-, 5-, and 10-year freedom from reintervention rates for the entire population were 100%, 78.7% and 27%, respectively (Fig. 3).Fig. 3. Actuarial freedom from reintervention of all patients
In the comparative analysis, the 1-, 5-, and 10-year freedom from reintervention rates in the Contegra group were 100%, 94.1%, and 47.1%, respectively. In the Biointegral group, the 1- and 5-year freedom from reintervention rates were 100% and 63.3%, respectively. The difference between groups were statistically significant (p = 0.024) (Fig. 4).Fig. 4. Actuarial freedom from reinterventions according to the conduit types
Discussion
Conduit choice may be the mainstay of a surgical procedure during correction of some congenital heart defects. As conduit failure is inevitable for all kinds of available conduits, all children deserve to have a conduit with the best outcomes. Pulmonary homograft conduit is considered the best for RVOT reconstruction with an approximate 10-year freedom from reoperation of 60–90%, but their scarcity prevents common usage [4, 6, 11]. Studies to develop an “ideal” conduit are still going on. Different materials, treatment methods, decellularization, and scaffold repopulation are being explored to achieve the ultimate goal [12]. To date, all conduit types are far from being optimal. In this study, we used two different types of xenograft conduits and our results are surprising. First of all, conduit failure is not a “benign” phenomenon. We had six late deaths; half of them died during reintervention and the other half died while waiting for reintervention. Five of the deaths were in the Biointegral group and both actuarial survival and freedom from reintervention rates were statistically different between the groups, favoring the Contegra conduit.
As mentioned before, no comparative study has been performed between Contegra and Biointegral conduits. To design a comparative study is not easy and may have some drawbacks. For example, neonates and infants with small conduits may need replacement earlier. The anatomic position of the conduit may affect longevity. Conduits after the Ross operation may perform better than conduits that are in an extra-anatomic position after the Rastelli operation. Patients who need unifocalization due to major aorto-pulmonary collaterals may have the worst conduit performance because of the high incidence of underdeveloped pulmonary vascular bed and higher pulmonary vascular resistance [11, 12]. To eliminate these biases, we excluded those patients from the study so that we could obtain well-balanced study groups. We think that our results may be noteworthy. We stopped using Biointegral pulmonary conduits and tried to find other alternatives. Handmade ePTFE valved Gore-Tex grafts may be promising with longer durability and lower risk of compression. In our study handmade trileaflet ePTFE valved conduits were sewn as described in Ando et al.’s [13] article. They used these conduits in 139 patients with complex congenital disease in their report. This technique is easy to apply and the grafts are not expensive and are mostly available. Also, as Contegra conduits don’t have larger sizes, in older children these conduits may be an alternative. Fujita et al. [14] reported that among 502 patients with ePTFE valved conduits, freedom from conduit explantation was 99.5% at 5 years and 89% at 10 years.
Shelhigh pulmonic valved conduit (Shelhigh Inc., Millburn, NJ) is another porcine conduit, harvested unbloc from porcine pulmonary artery. It is a natural conduit and does not contain any suture lines, like Biointegral conduit. According to a comparative study performed by Schoenhoff et al. [15], Contegra performed better than the Shelhigh conduit, although the difference was not statistically significant. Among 84 patients and 100 implantations (Contegra: 43 and Shelhigh: 57), the mean time to replacement was 18 ± 9 months for the Shelhigh pulmonic graft versus 42 ± 4 months for the Contegra conduit (p = 0.25).
Breymann et al. [16] presented the European Contegra Multicentre Study involving 165 Contegra implants and concluded that results at seven years were comparable to those of homografts. At 5 years of follow-up, freedom from any event was 13% for infants, 58% for 1–10-year-olds, and 82% for those above 10 years. Protopapas and Athanasiou reviewed the published literature and analyzed midterm outcomes from 17 reports covering a total of 767 patients. After a total follow-up of 573 patient-years, conduit stenosis was observed in 10.9% of the patients, more often in smaller sizes [17].
Brown et al. [10] analyzed their 216 patients who received Contegra (n = 153) and pulmonary homografts (n = 63). No significant differences were present between the groups with respect to mean age, body surface area, conduit indication or conduit diameter, although the mean follow-up duration was longer in patients who received homografts. Conduit dysfunction, conduit failure and the need for explantation were more in homografts, albeit at longer follow-up interval. The rate of conduit dysfunction was significantly higher in the pulmonary homograft cohort (73% and 47% at five and ten years, respectively) compared to the Contegra group (90% and 82% at five and ten years), respectively (p < 0.001). Similar to Brown’s series, Hickey et al. [18] compared the Contegra conduit with the homografts in 107 infants who survived truncus arteriosus repair, from 17 different institutions. They stated that the propensity-adjusted 3-year freedom from replacement for in-conduit stenosis was 96.4% for the Contegra and 69.8% for the homograft (p = 0.05). It seems that Contegra has a comparable performance with homografts, especially in small sizes. According to our experience, we think that the calcification rate of the Contegra conduits may be lower than that of other conduits, including homografts. Transcatheter reinterventions may be easier for the Contegra conduits when needed. Larger-sized stent grafts can be implanted during transcatheter interventions. However, Biointegral conduits are usually resistant to balloon dilatation due to heavy calcification. When we asked to our colleagues who are expert in transcatheter interventions, they confirmed our findings.
The downsides of the Contegra conduit are distal anastomotic stenosis and conduit dilatation especially during exposure to high pressure. In one of our latest articles [9], we detected severe dilatation in 4 (31%) out of 13 patients who underwent truncus arteriosus repair, after a median follow-up of 36 months. Additionally, three (23%) patients had stenosis at the distal anastomosis. In this study, no conduit dilatation or stenosis in at the distal anastomosis was encountered. Probably small pulmonary artery-conduit mismatch and pulmonary hypertension can be reasons for these complications. One of the largest series comparing porcine valved conduits to homografts belongs to Dearani et al. [19]. They stated that, the durability of the homografts was inferior to the porcine valved Dacron conduits in the late follow-up of 1095 patients. Their total freedom from reoperation rates were 55.5% and 31.9% at 10 and 20 years, respectively [19].
As patients with conduit failure may be asymptomatic, periodic clinical examinations with echocardiography are mandatory to detect dysfunction and high pressures in the right ventricle. As mentioned before, patients with conduits are at risk for sudden death or other major adverse events. Timely and proper reinterventions are very important to prevent worse outcomes [11, 12, 20].
In conclusion, the outcomes of the Contegra conduit were statistically significantly better than the Biointegral conduits, in terms of both survival and freedom from reintervention. Contegra is still the most valuable alternative to homografts. We believe that the choice of conduit in the first surgery is an important decision that directly affects survival and reintervention rates.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abolhoda A, Sumei Y, Oyarzun R, Allen KR, Cormick JRM, Shenggao H et al (1996) No-react detoxification process: a superior anticalcification method for bioprostheses. Ann Thorac Surg 62:1724–173010.1016/s 0003-4975(96)00948-48957377 · doi ↗ · pubmed ↗
- 2Hickey EJ, Mc Crindle BW, Blackstone EH, Yeh T, Pigula F, Clarke D, Tchervenkov CI, Hawkins J, CHSS Pulmonary Conduit Working Group (2008) Jugular venous valved conduit (Contegra) matches allograft performance in infant truncus arteriosus repair. Eur J Cardiothorac Surg 33:890–89810.1016/j.ejcts.2007.12.05218313324 · doi ↗ · pubmed ↗