Impact of the SARS-CoV-2 pandemic on healthy aging and functionality in older Mexican adults: insights from the MHAS cohort
Carmen Arroyo-Quiroz, Silvestre Alavez

TL;DR
This study explores how the SARS-CoV-2 pandemic affected the health and functionality of older adults in Mexico, finding that hospitalization from COVID-19 was linked to worse aging outcomes, while vaccination helped prevent functional decline.
Contribution
The study provides novel insights into the multidimensional impact of the pandemic on healthy aging in Latin America, particularly focusing on Mexico.
Findings
Hospitalization due to COVID-19 was significantly associated with lower Healthy Aging Scores.
Vaccination was linked to a reduced likelihood of functional impairment.
Infection and vaccination were not significantly associated with changes in the Healthy Aging Score.
Abstract
Older adults were among the most affected by the COVID-19 pandemic, facing greater vulnerability to infection, hospitalization, and post-infection sequelae. However, evidence on its multidimensional impact on healthy aging remains limited, particularly in Latin America. This study examined the association of COVID-19 infection, hospitalization, and vaccination with healthy aging and functional impairment among older Mexican adults. We analyzed longitudinal data from the Mexican Health and Aging Study (MHAS), comparing pre-pandemic (2018) and post-pandemic (2021) waves. Two outcomes were assessed: the Healthy Aging Score (HAS), a composite indicator of physical, mental, and social functioning (mean = 50, SD = 10), and functional impairment, defined as any limitation in basic or multiple instrumental activities of daily living. Random-effects regression models estimated associations with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
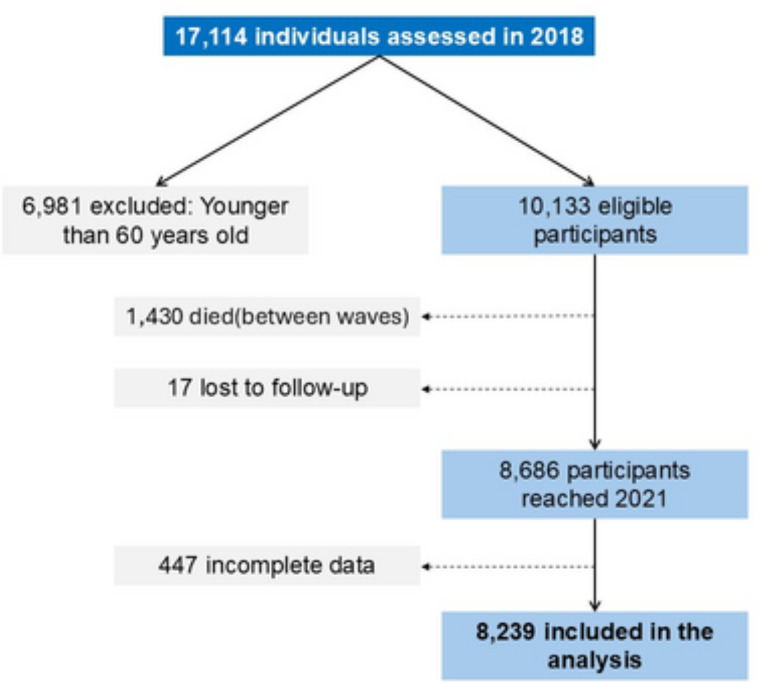 Figure 1
Figure 1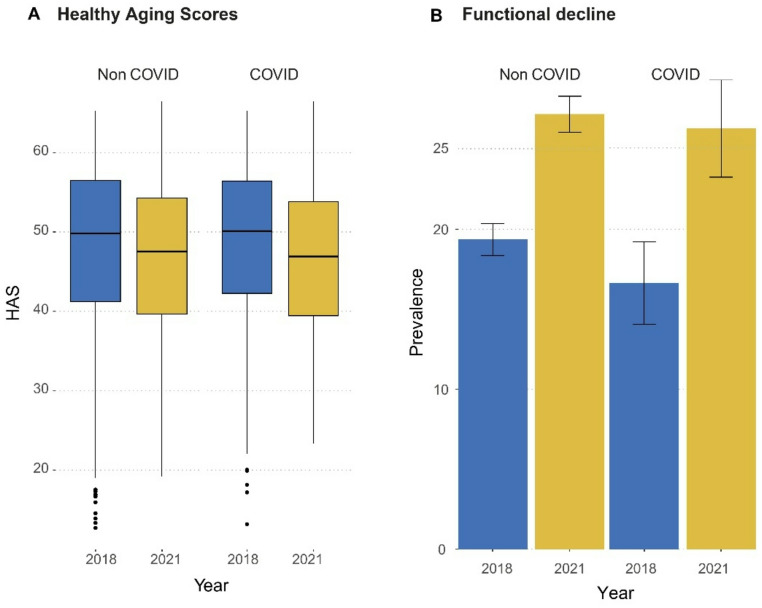 Figure 2
Figure 2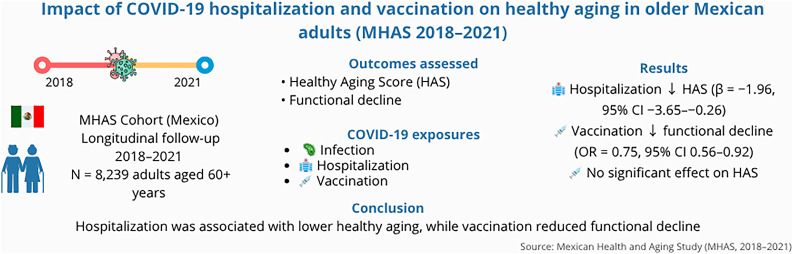 Figure 3
Figure 3- —Universidad Autonoma Metropolitana
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 and Mental Health · Aging and Gerontology Research · Health disparities and outcomes
Introduction
The COVID-19 pandemic has represented one of the most profound public health challenges of recent decades, with disproportionate consequences for older adults due to age-related physiological vulnerability and comorbid conditions [1, 2]. Beyond the elevated rates of infection, hospitalization, and mortality, accumulating evidence highlights the long-term functional and clinical consequences of SARS-CoV-2 infection in this population [3–5]. Older adults have also shown the highest prevalence of long COVID or persistent post-infection symptoms [6, 7]. These findings suggest that COVID-19 may compromise key domains associated with aging well, such as physical capacity, independence, and overall functioning.
Functional decline and frailty progression have emerged as major post-COVID sequelae among older survivors. In France, nearly half of older patients reported persistent symptoms three months after infection, and one-third were newly classified as frail despite being robust at baseline [8]. Similarly, an Italian cohort reported that over 40% of previously independent older adults either died or lost functional autonomy within six months following hospitalization [9]. A large U.S. study found that nearly one-third of older adults developed at least one new health condition after COVID-19, 11% more than uninfected peers [6]. Consistent with this evidence, hospitalization has been widely used as a proxy for severe COVID-19 among older adults and has been associated with subsequent functional decline, particularly in those aged 70 years and older [10]. These findings point to a broader clinical picture of post-COVID aging characterized by increased frailty, multimorbidity, and functional loss.
In Mexico, the population is aging rapidly, with adults aged 60 years and older now accounting for over 12% of the total population, a proportion that is projected to double within the next three decades [11]. This demographic process is taking place in a context of marked socioeconomic inequality, high levels of informal employment, and a fragmented health system, which influence access to healthcare, social protection, and support services for older adults [12, 13]. These structural conditions are essential to consider when examining health trajectories among older Mexicans.
During the COVID-19 pandemic, these vulnerabilities likely intensified risk in this population. Older adults in Mexico experienced disproportionately high rates of severe disease, hospitalization, and mortality, while simultaneously facing disruptions in routine care, rehabilitation, and community or family support [7, 12, 14]. National vaccination campaigns prioritized older adults and achieved broad coverage, although with regional and socioeconomic heterogeneity [15, 16]. By late 2021, approximately 85–90% of adults aged ≥ 60 years in Mexico had received at least one COVID-19 vaccine dose, and national analyses reported substantial reductions in hospitalizations and deaths following vaccine rollout [16, 17]. Vaccination has been consistently associated with reductions in severe COVID-19 outcomes [18, 19]. However, there is limited evidence on how these pandemic-related experiences relate to broader trajectories of healthy aging in older adults, particularly in Mexico.
Despite emerging evidence on the clinical sequelae of COVID-19, few studies have examined its broader impact on healthy aging using composite indicators that integrate physical, functional, and psychosocial domains, particularly in low- and middle-income countries. According to the World Health Organization, healthy aging refers to “the process of developing and maintaining the functional ability that enables well-being in older age” [20]. Recent international evidence suggests that fewer than one in four older adults achieve healthy aging when assessed comprehensively, highlighting the relevance of monitoring this outcome [21]. Given that COVID-19 and related disruptions may compromise these domains, it is essential to evaluate how pandemic experiences relate to broader aging trajectories. Therefore, this study aimed to analyze the impact of the COVID-19 pandemic on healthy aging and functional status among Mexican older adults and to explore the role of COVID-19 vaccination and hospitalization as relevant health-related variables of interest.
Materials and methods
Data sources
Data were drawn from the Mexican Health and Aging Study (MHAS), a nationally representative cohort of adults aged 50 years and older in Mexico [22]. The methodology has been described elsewhere [22, 23]. Data and documentation are publicly available at [www.MHASweb.org].
For this analysis, we included participants interviewed in both the 2018 and 2021 waves. Of 17,114 respondents in 2018, we excluded those younger than 60 years (n = 6,981). Among 10,133 eligible participants, 1,430 died and 17 were lost to follow-up, leaving 8,686 survivors in 2021. After excluding incomplete cases, the final analytic sample comprised 8,239 individuals (Fig. 1).
Fig. 1. Participant flow diagram showing sample inclusion and follow-up between the 2018 and 2021 waves of the Mexican Health and Aging Study (MHAS)
Study outcomes
Two outcomes were examined: the Healthy Aging Score (HAS) and physical functional impairment assessed through ADL and IADL limitations. The Healthy Aging Score (HAS) was constructed following the methodology by Sánchez-Niubó et al. [24], based on 41 items. The score includes indicators of physical capacity, psychological well-being, sensory function, and social participation. All items were dichotomized to indicate the presence or absence of difficulties, and a two-parameter logistic item response theory (IRT) model was applied. Expected-a-posteriori estimates were transformed into T-scores (mean = 50, SD = 10), representing overall healthy aging, with higher values indicating better healthy aging. In the present study, 39 of the 41 ATHLOS items were operationally available in MHAS and were used to construct the HAS; only two items had no equivalent measure and were therefore not included. Although some individual performance items related to daily functioning are included as indicators of physical capacity, the HAS does not operationalize clinical disability. Functional impairment based on ADL/IADL limitations was analyzed separately as an independent outcome, and chronic diseases were not included in the HAS. A complete list of included items, correspondence with MHAS variables, coding rules, and IRT details is provided in Supplementary Material 1.
Functional status was assessed using basic and instrumental activities of daily living (ADL and IADL). Normal physical function was defined as no limitation in ADL and at most one limitation in IADL, as validated for the Mexican population [25]. ADLs included bathing, dressing, eating, getting into or out of bed, using the toilet, and walking inside the home. IADLs included preparing a hot meal, shopping, taking medications, and managing money. Individuals who did not meet the criteria for normal physical function were classified as having physical functional impairment.
Although a number of individual performance items related to daily functioning are included within the HAS as indicators of physical capacity, the HAS captures a broader multidimensional construct of healthy aging and does not operationalize disability. Therefore, functional impairment was examined separately using an ADL/IADL-based definition, which has been validated and extensively used in studies with Mexican older adults. This distinction is consistent with international conceptual models distinguishing functional capacity from functional disability and ensures comparability with previous literature.
Main exposure
Self-reported history of COVID-19 infection was assessed in 2021 by the question: “Since March 2020,* has a doctor or medical personnel told you that you had or currently have COVID-19?”* Participants additionally reported any COVID-19–related hospitalization and vaccination status (≥ 1 dose). Hospitalization was considered a proxy for severe COVID-19, and vaccination a relevant COVID-related health exposure; both variables are conceptually and epidemiologically justified in the Introduction.
Covariates
Covariates included sex, age (five-year groups), education, physical activity (≥ 3 times/week), BMI, employment status, and chronic conditions (hypertension, diabetes, heart disease, stroke, obesity, and depression). BMI was initially categorized as < 20 kg/m² (underweight), 20–24.9 kg/m² (normal weight), 25–29.9 kg/m² (overweight), and ≥ 30 kg/m² (obesity), and these categories are presented in Table 1 for descriptive purposes. However, in multivariable models the overweight category was not significantly associated with the outcomes and did not improve model fit; therefore, overweight was combined with the reference group and only obesity (≥ 30 kg/m²) was retained as a separate category in Table 2. All covariates were measured in 2018 and 2021.
Table 1. Baseline characteristics of 8,239 Mexican older adults (MHAS 2021) by self-reported COVID-19 infection statusTotalCOVIDNon-COVIDp-value**N* = 8239n = 943N = 7296Age (years), mean (SD)72.5 (7.6)71.1 (6.9)72.7 (8.8)< 0.01´Sex, n(%) Male4434 (44)390 (41.2)4044 (44.3)0.1 Female5659 (55.9)551 (58.4)5108 (55.6)Weight status, n(%) Underweight172(2)7(0.8)165(2.1)< 0.01 Normal weight2915(33.3)196(23.1)2719(34.4) Overweight3555(40.6)377(44.4)3178(40.2) Obesity1950(22.3)250(29.4)1700(21.5)Hypertension, n(%)5190 (51.3)497 (52.7)4693 (51.1)0.38Diabetes, n(%)2807 (27.7)264 (28)2543 (27.7)0.86Cardiac problems, n(%)901 (8.9)95 (10.1)806 (8.8)0.15Depressive symptoms, n(%)2816 (31)260 (29.4)2556 (31.2)0.25Physical activity, n(%)º2649 (29.1)277 (31.2)2372 (28.8)0.13Employment, n(%)2791 (27.5)295 (31.3)2496 (27.2)0.01Years of education, mean(SD)5.3 (4.6)5.9 (4.8)5.2 (4.6)< 0.01´ Outcomes HAS, mean (SD)48.6 (10)49 (9.6)48.6 (10.1)0.41Functionality problems, n(%)1570 (19.1)157 (16.6)1413 (19.4)0.05HAS: Healthy Aging Score, *P-value for the comparison COVID-19 survivors and non–COVID-19 survivors, Chi-squared test unless otherwise indicated, ’ Kruskal-Wallis test, ºPhysically active: those who reported to exercise/hard physical work 3 or more times per week
Table 2. Estimated associations of COVID-19 status with healthy aging score (HAS) and functional decline.Regression estimates for the associations between COVID-19 infection,* hospitalization*,* and vaccination with two outcomes: HAS (continuous) and functional decline (binary).VariableHASFunctional impairmentCoef.95% CIp*-valueOR95% CIp-value Sex (ref: male) Female-2.09(-2.45, -1.73)< 0.0011.24(1.08, 1.44)< 0.001 Year (ref: 2018) Year 2021-0.34(-0.51, -0.17)< 0.0011.22(1.12, 1.34)< 0.001 Age group (ref: 60–69 years) 70–79-0.11(-0.6,0.37)0.650.88(0.68, 1.15)0.38 80+-1.44(-2.34, -0.54)< 0.0011.27(0.88, 1.63)0.31 Health variables (ref: no condition) Hypertension-1.58(-1.88, -1.28)< 0.0011.34(1.16, 1.52)< 0.001Diabetes-2.03(-2.37, -1.69)< 0.0011.83(1.52, 2.11)< 0.001Cardiac condition-2.71(-3.18, -2.24)< 0.0011.96(1.41, 2.28)< 0.001Stroke-3.13(-4.03, -2.22)< 0.0012.64(1.93, 3.58)< 0.001Obesity-1.09(-1.48, -0.71)< 0.0011.63(1.35, 1.95)< 0.001Depression-5.17(-5.47, -4.86)< 0.0013.89(3.14, 4.72)< 0.001Physical activity ≥ 3 times/week1.46(1.18, 1.74)< 0.0010.61(0.46, 0.75)< 0.001 Socioeconomic variables Employment (ref: not employed)1.52(1.20, 1.84)< 0.0010.65(0.48, 0.79)< 0.001Income quartile (ref: Q1 – lowest quartile) Q2-0.82(-1.21, -0.44)< 0.0011.22(1.01, 1.49)0.04 Q3-1.07(-1.52, -0.62)< 0.0011.27(1.03, 1.61)0.05 Q4-0.5(-1.06, 0.07)0.081.06(0.77, 1.41)0.71 COVID VARIABLES (ref: absence of) COVID-0.25(-0.78, 0.28)0.350.86(0.63, 1.02)0.27Hospitalization-1.96(-3.65, -0.26)0.021.77(0.88, 2.53)0.13Vaccine0.49(-0.03, 1.01)0.070.75(0.56, 0.92)0.02HAS = Healthy Aging Score; Q = income quartile; OR = odds ratio. Models adjusted for all covariates listed. The intercept was estimated but is not reported for brevity. Reference categories are indicated in parentheses in the table headersBMI was initially modeled using four categories. Overweight was not associated with outcomes and was combined with the reference group to improve model parsimony. Only obesity (≥ 30 kg/m²) is shown
Depression was defined using a modified nine-item CES-D scale, with ≥ 5 positive responses indicating depression [26]. All covariates were modeled as time-varying and were updated using information from both 2018 and 2021, consistent with the longitudinal design of the study.
Statistical analysis
We summarized baseline sociodemographic and lifestyle characteristics as mean ± standard deviation (SD) or median and interquartile range (IQR) for continuous variables, and as percentages for categorical variables. Differences between groups were assessed using chi-square tests for categorical variables and t-tests for continuous variables; the Kruskal–Wallis test was applied when normality assumptions were not met.
Associations between self-reported COVID-19 infection, hospitalization, and vaccination (≥ 1 dose) with healthy aging outcomes were evaluated using random-effects models. For the Healthy Aging Score (HAS), we fitted a random-effects generalized least squares (GLS) model with Mundlak correction, including the individual means of time-varying covariates (mean age, mean income quartile, and mean education level) to separate within- and between-individual variability. For functional impairment, we applied a random-effects logistic regression model with the same specification. Both models adjusted for sex, age group, education, BMI category, physical activity, and chronic conditions (depression, hypertension, diabetes, cardiac disease, obesity, and stroke). Robust standard errors clustered at the individual level were used to account for within-person correlation across observations.
Sensitivity analyses were conducted to evaluate model robustness. First, we re-estimated models excluding major chronic diseases (depression, hypertension, and diabetes). Second, we restricted the sample to participants younger than 80 years. Third, outliers in HAS, functional outcomes, and BMI were excluded. Fourth, we incorporated interaction terms between vaccination and sex or age. Finally, fixed-effects models were fitted for comparison with random-effects estimates.
All analyses were conducted using Stata version 18.5 (StataCorp, College Station, TX).
Ethics approval and consent to participate
This study is a secondary analysis of de-identified data from the Mexican Health and Aging Study (MHAS). The MHAS protocol received ethical approval from the Institutional Review Board of the University of Texas Medical Branch in the United States and the Ethics Committee of the National Institute of Public Health in Mexico. All participants provided informed consent prior to data collection in each wave.
Results
Table 1 presents the main characteristics of the study sample, which comprised 8,239 participants, 55.9% of whom were women. At baseline, the mean age was 72.5 years (SD = 7.6). Among participants, 62.9% were classified as overweight or obese, 27.7% had diabetes, 51.3% had hypertension, and 8.9% reported cardiac disease. Regarding socioeconomic variables, 27.5% were employed, and the mean years of education were 5.3 (SD = 4.6).
Most variables showed significant differences between participants with and without a history of COVID-19 infection. Compared with non-COVID-19 participants, those who reported previous infection were younger, had higher BMI, and more frequently reported employment and higher education. In 2018, the COVID-19 group also had fewer functional impairments (16.6% vs. 19.4%, p = 0.05) and slightly higher HAS, although this difference was not statistically significant (49.0 vs. 48.6, p = 0.41).
HAS T-scores were computed for all participants with two available measurements (Fig. 2A). The mean HAS was 48.6 (SD = 10.0) in 2018 and 47.0 (SD = 10.0) in 2021, representing an average decrease of − 1.62 points (SD = 8.7), equivalent to a − 1.4% change over the study period.
When comparing groups, individuals with prior COVID-19 infection showed higher HAS at baseline (48.9 vs. 48.6, p < 0.001) but not at follow-up (46.6 vs. 47.0, p = 0.17). The mean percentage change was slightly greater among the COVID-19 group (− 4.8%) than in the non-COVID group (− 3.1%), although the difference was not statistically significant (p = 0.19).
Regarding functional impairment (Fig. 2B), its prevalence increased from 19.1% in 2018 to 27.1% in 2021 (p < 0.001). Among non-COVID participants, impairment rose from 19.4% to 27.2% (≈ 40% increase), while in the COVID-19 group it increased from 16.7% to 26.3% (≈ 58% increase). Both within-group changes were statistically significant (p < 0.001).
Fig. 2. Healthy Aging Score (HAS) and prevalence of functional decline among older Mexican adults in 2018 and 2021. Panel A displays mean HAS scores by COVID-19 infection status across both waves. Panel B shows the proportion of participants with functional decline, highlighting increased prevalence in both groups by 2021. Error bars represent standard deviations
The results of multivariate models for HAS and functional impairment, adjusted for sex, age, chronic conditions, physical activity, employment, and obesity, are presented in Table 2.
For HAS, protective effects were observed for regular exercise (β = 1.46, 95% CI: 1.18–1.74) and employment (β = 1.52, 95% CI: 1.20–1.84). Negative associations were found for female sex (β = −2.09, 95% CI: −2.45, − 1.73), older age groups, hypertension (β = −1.58, 95% CI: −1.88, − 1.28), diabetes (β = −2.03, 95% CI: −2.37, − 1.69), cardiac disease (β = −2.71, 95% CI: −3.18, − 2.24), obesity (β = −1.09, 95% CI: −1.48, − 0.71), and depression (β = −5.17, 95% CI: −5.47, − 4.86).
COVID-19 infection and vaccination were not significantly associated with HAS, whereas hospitalization due to COVID-19 was negatively associated (β = −1.96, 95% CI: −3.65, − 0.26). Between-individual effects were significant for mean age (β = −2.82, 95% CI: −3.33, − 2.31) and mean income quartile (β = 1.09, 95% CI: 0.83, 1.36), suggesting that higher long-term income is associated with better healthy aging outcomes.
For functional impairment, the direction and significance of most covariates were consistent with those observed for HAS, although some differences in magnitude were noted. Depression showed the strongest association (OR = 3.88, 95% CI: 3.14–4.72, p < 0.001), followed by stroke (OR = 2.64, 95% CI: 1.93–3.58, p < 0.001) and diabetes (OR = 1.83, 95% CI: 1.52–2.11, p < 0.001). Female sex, older age, and chronic conditions (hypertension, cardiac disease, obesity, stroke) were significantly associated with increased odds of functional impairment. Conversely, regular exercise (OR = 0.60, 95% CI: 0.46–0.75, p < 0.001) and employment (OR = 0.52, 95% CI: 0.39–0.65, p < 0.001) were protective. Neither self-reported COVID-19 infection nor hospitalization was significantly associated with functional impairment, whereas vaccination showed a protective effect (OR = 0.75, 95% CI: 0.53–0.95, p = 0.02).
Sensitivity Analyses
Sensitivity analyses confirmed the robustness of the results (Supplementary Material 1–2). Excluding depression, hypertension, diabetes, or participants aged ≥ 80 years resulted in only minor changes in effect sizes without altering direction or significance. Fixed-effects models, particularly for functional impairment, retained fewer cases and slightly affected some estimates. Removing extreme values of HAS, functional outcomes, and BMI confirmed that results were not driven by outliers. Interaction terms for vaccination with sex and age were non-significant. Despite the omission of variables with no within-group variation (e.g., sex, age group, income quartile), associations with chronic conditions, physical activity, and employment status remained consistent. Overall, findings across datasets supported the stability of the original models.
Discussion
In this nationally representative study of older Mexican adults, we examined the association of COVID-19 infection, hospitalization, and vaccination with healthy aging and functional status. We found that COVID-19–related hospitalization, as an indicator of COVID-19 severity, was significantly associated with lower Healthy Aging Scores (HAS), while vaccination was protective against functional impairment. These findings suggest that severe COVID-19 may accelerate declines in multidimensional health, whereas vaccination contributes to preserving autonomy and functionality in later life. These patterns are particularly relevant in Mexico, where vaccination coverage among adults aged ≥ 60 years reached over 80% during 2021, yet regional and socioeconomic heterogeneity persists, implying that not all older adults benefited equally from immunization efforts [15, 17].
The Healthy Aging Score (HAS) captures a broad construct of health, integrating physical, cognitive, and psychosocial domains. A lower HAS indicates reduced physiological reserve and resilience—factors closely linked to frailty, disability, and mortality risk. The observed negative association between COVID-19 hospitalization and HAS therefore signals potential long-term vulnerability in older adults recovering from severe infection. These results align with clinical observations of post-COVID functional loss and with the conceptual overlap between post-acute sequelae and frailty syndromes [27]. In line with recent evidence showing that older adults hospitalized with COVID-19 experience greater functional loss and poorer prognosis than younger patients, but can still benefit substantially from inpatient rehabilitation [10], our findings suggest that preserving functional reserve after severe infection is a key component of healthy aging trajectories.
The Healthy Aging Score (HAS) is consistent with the WHO definition of healthy aging as the maintenance of functional ability determined by intrinsic capacity and environmental factors [28]. Evidence from ATHLOS and related studies shows that multidimensional indicators of this type are comparable across populations and predict mortality and functional outcomes [24, 29]. Similar approaches applied in the Mexican Health and Aging Study have also identified heterogeneous healthy aging trajectories, reinforcing the relevance of multidimensional indicators in this context [30]. Thus, the HAS is suitable for interpreting the potential long-term impact of COVID-19 on aging trajectories.
Our findings complement previous research documenting persistent symptoms and reduced functional capacity among older survivors of COVID-19 [8, 9, 31]. Studies in Europe and North America have reported that up to 40–50% of older adults hospitalized for COVID-19 experience new or worsened limitations in daily functioning, mobility, or cognitive performance within months of discharge [9, 32]. The mechanisms underlying these changes are multifactorial and may include prolonged inflammation, endothelial dysfunction, deconditioning, and exacerbation of pre-existing comorbidities [33, 34]. Such biological and behavioral pathways can compromise the capacity to recover homeostasis after stressors, accelerating transitions from robustness to vulnerability—one of the key determinants of healthy aging trajectories.
Although COVID-19–related exposures were the primary focus of this study, several covariates consistently emerged as robust predictors of healthy aging and functional outcomes. Female sex, depression, diabetes, and cardiovascular conditions (including cardiac disease and stroke) were all significantly associated with lower HAS scores and increased functional impairment. These findings align with `gender-health paradox´ whereby women, despite their greater longevity, frequently experience higher disability burden in later life, even after controlling for age and other risk factors [35–37]; that depression substantially contributes to functional decline and reduced resilience [38, 39]; and that cardiometabolic diseases accelerate biological aging, frailty, and disability trajectories [40–42]. Recent analyses using MHAS and other Mexican data have also documented widening inequalities in basic and instrumental activities of daily living by wealth and gender, with women and poorer older adults experiencing higher and increasing levels of functional limitations over time [43]. By acknowledging these underlying factors, we can contextualize our results within the long-standing health disparities that continue to shape the lives of older adults across Mexico.
The protective association of vaccination with functional outcomes underscores the broader benefits of immunization beyond infection prevention. COVID-19 vaccines have been shown to reduce disease severity, hospitalization, and mortality in older adults [44], and accumulating evidence suggests that vaccinated individuals who become infected exhibit milder and shorter post-COVID sequelae [45, 46]. From a geriatric perspective, maintaining vaccination coverage is an essential component of preserving function and delaying frailty progression. In the Mexican context—where vaccination coverage in older adults exceeded 80% by mid-2021 [17]—these results reinforce the role of sustained immunization and booster campaigns as tools to protect multidimensional health in aging populations. In Mexico, although vaccination coverage among older adults was high, it was not evenly distributed. Evidence shows that vaccination uptake was lower among older adults with fewer economic resources, lower education, and more limited access to health services, particularly in rural and disadvantaged contexts [15, 44, 45]. In Mexico City, for example, around 7–8% of older adults did not receive a first vaccine dose despite universal eligibility, mainly due to misinformation, vaccine hesitancy, socioeconomic barriers, and household food insecurity [15]. These inequities are relevant to interpreting our findings: they suggest that the protective association between vaccination and functional outcomes likely reflects not only biomedical protection but also underlying social advantage [47]. Older adults with better socioeconomic conditions may have been more likely to access vaccination and, simultaneously, to maintain health care continuity, rehabilitation, nutrition, and social support during the pandemic [15, 47]. Therefore, the benefits of vaccination may have compounded existing social gradients in aging, reinforcing the need for equity-oriented vaccination policies and targeted support for vulnerable older adults.
Interestingly, self-reported COVID-19 infection was not associated with either HAS or functional impairment. This lack of association likely reflects measurement limitations. Only 10% of participants reported infection, far below the estimated 25% national seroprevalence [17, 48]. Many infections among older adults may have been asymptomatic or unrecognized, as a substantial proportion of SARS-CoV-2 infections occur without symptoms or go undetected in surveillance systems [48, 49]. Moreover, self-reported variables introduce recall bias and differential misclassification, particularly in cognitively impaired individuals. In contrast, hospitalization data are less subject to reporting errors and represent severe cases, explaining the stronger associations observed for this exposure.
The overlap between post-COVID symptoms and aging-related conditions complicates causal attribution. Chronic fatigue, reduced endurance, dyspnea, and cognitive difficulties are common to both long COVID and geriatric syndromes. Recent studies have emphasized that acute SARS-CoV-2 infection can precipitate decompensation in multiple systems, including cardiovascular, metabolic, and neurological pathways [50, 51]. The convergence of these processes may amplify frailty and accelerate the decline of functional reserve, leading to lower HAS scores over time.
Our results also highlight the importance of contextual factors in Latin America. Older adults in Mexico often face high burden of multimorbidity, poverty, and limited access to health care services [12]. Moreover, external shocks such as the COVID-19 pandemic have exacerbated vulnerabilities in nutritional and functional status among older adults [52]. In addition, the Mexican health system is highly fragmented, and access to services remains unequal across socioeconomic and geographic groups [13]. These structural barriers likely influence not only the probability of receiving vaccination and timely COVID-related care, but also access to rehabilitation and follow-up services that are essential to preserving functionality after severe illness. The pandemic further disrupted chronic-disease management and social support, conditions that are strongly linked to functional loss. The HAS, by capturing biopsychosocial dimensions, provides a valuable lens to monitor how such structural inequities translate into differential aging trajectories. Integrating functional and psychosocial indicators into national surveillance could strengthen early identification of individuals at risk of accelerated aging.
More broadly, evidence from MHAS and Mexican national health surveys shows that access to health care, hospitalization, and preventive service use among older adults are strongly patterned by health insurance coverage, socioeconomic status, and urban–rural residence, highlighting ongoing structural inequities within [43, 53, 54]. These factors likely shaped not only COVID-19 exposure and vaccine accessibility but also the capacity for rehabilitation and functional recovery. Consequently, employing the Healthy Aging Scale (HAS) enables an assessment of how structural and social determinants manifest as unequal aging trajectories, extending the analysis beyond purely clinical outcomes.
Some limitations should be considered. First, all measures, including COVID-19 exposure, were self-reported and subject to recall bias. The timing between infection and assessment could not be determined, and effects may have attenuated among early cases. Second, unmeasured confounding (e.g., nutrition, medication use, sleep quality) could influence results. Third, the number of confirmed COVID-19 cases was smaller than national estimates, reducing statistical power for subgroup analyses. Despite these limitations, our study has notable strengths: the use of a nationally representative cohort, pre-pandemic baseline data, and a validated multidimensional indicator of healthy aging. These features enable a more robust evaluation of pandemic-related changes in functionality and resilience among older adults.
Clinically, our findings suggest that post-hospitalization follow-up and functional assessment should be routine for older adults recovering from COVID-19. Rehabilitation programs addressing mobility, endurance, and psychosocial well-being may mitigate the long-term effects of severe infection. Public-health strategies should also emphasize booster vaccination and targeted outreach to socioeconomically disadvantaged older adults, who may experience greater barriers to care and recovery. From a research perspective, future studies should incorporate objective measures of physical performance (e.g., grip strength, gait speed), biomarkers of inflammation, and longer follow-up to clarify the biological mechanisms linking COVID-19 severity to healthy aging outcomes. More broadly, our findings reinforce the relevance of healthy aging as a policy framework, highlighting the need to protect functional capacity, resilience, and autonomy among older adults in the post-pandemic context.
Conclusions
COVID-19 hospitalization was associated with lower Healthy Aging Scores, indicating multidimensional health deterioration among older adults, while vaccination was protective against functional impairment. These findings reinforce the clinical importance of preventing severe infections and maintaining vaccination coverage to sustain functionality, independence, and healthy aging. As health systems adapt to the post-pandemic era, continuous monitoring of functional and psychosocial domains in older adults will be critical to mitigate the long-term impact of COVID-19 on aging trajectories.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary Material 2
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Okoye C, Calsolaro V, Calabrese AM, Zotti S, Fedecostante M, Volpato S et al (2022) Determinants of Cause-Specific mortality and loss of independence in older patients following hospitalization for COVID-19: the Gero Covid outcomes study. J Clin Med 11(19). 10.3390/jcm 1119557810.3390/jcm 11195578 PMC 957111436233447 · doi ↗ · pubmed ↗
- 2MHAS M Ha AS (2012) Data Files and Documentation (public use): Mexican Health and Aging Study, Database. https://www.MHA Sweb.org. Retrieved from on 11 Mar 2019
- 3Correa L, Gomes CDS, Camara S, Barbosa JFS, Azevedo IG, Vafaei A et al (2023) Gender-Specific associations between Late-Life disability and socioeconomic status: findings from the international mobility and aging study (IMIAS). Int J Environ Res Public Health 20(4). 10.3390/ijerph 2004278910.3390/ijerph 20042789 PMC 995609536833484 · doi ↗ · pubmed ↗
- 4Jung J, Kim S, Kim B, Kim M, Yang J, Chung D et al (2022) Accelerated cognitive function decline in Community-Dwelling older adults during COVID-19 pandemic: the Korean frailty and aging cohort study (KFACS). Int J Environ Res Public Health 19(17). 10.3390/ijerph 19171066610.3390/ijerph 191710666 PMC 951842736078381 · doi ↗ · pubmed ↗