Brain Metastasis After Curative Resection of Non-small Cell Lung Cancer: A Systematic Review and Meta-Analysis
Ryuichi Ohta, Kasumi Nishikawa, Kaoru Tanaka, Hidetoshi Hayashi

TL;DR
This study reviews how often brain metastasis occurs after lung cancer surgery and finds that traditional clinical factors are better predictors than molecular ones.
Contribution
The study provides a meta-analysis of clinicopathological factors predicting brain metastasis after NSCLC surgery, highlighting the need for standardized surveillance.
Findings
The overall incidence of metachronous brain metastasis after NSCLC surgery is approximately 6.6%.
Traditional clinicopathological factors show more consistent associations with brain metastasis than molecular features like EGFR mutations.
Abstract
Metachronous brain metastasis is a clinically significant pattern of recurrence after curative-intent surgery for non-small cell lung cancer (NSCLC). The extent to which contemporary clinicopathological and molecular characteristics predict postoperative intracranial relapse, and whether routine postoperative neuroimaging might aid early detection, remains uncertain. We performed a systematic review and meta-analysis of studies reporting postoperative brain metastasis following curative resection for NSCLC. Fourteen retrospective cohort studies published between 2010 and 2025 were included, comprising 13,414 patients and 883 documented intracranial recurrence events. Data extraction focused on clinicopathological factors, molecular features, follow-up duration, and multivariable-adjusted hazard ratios (HRs). Only HRs derived from multivariable Cox regression models were pooled; studies…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
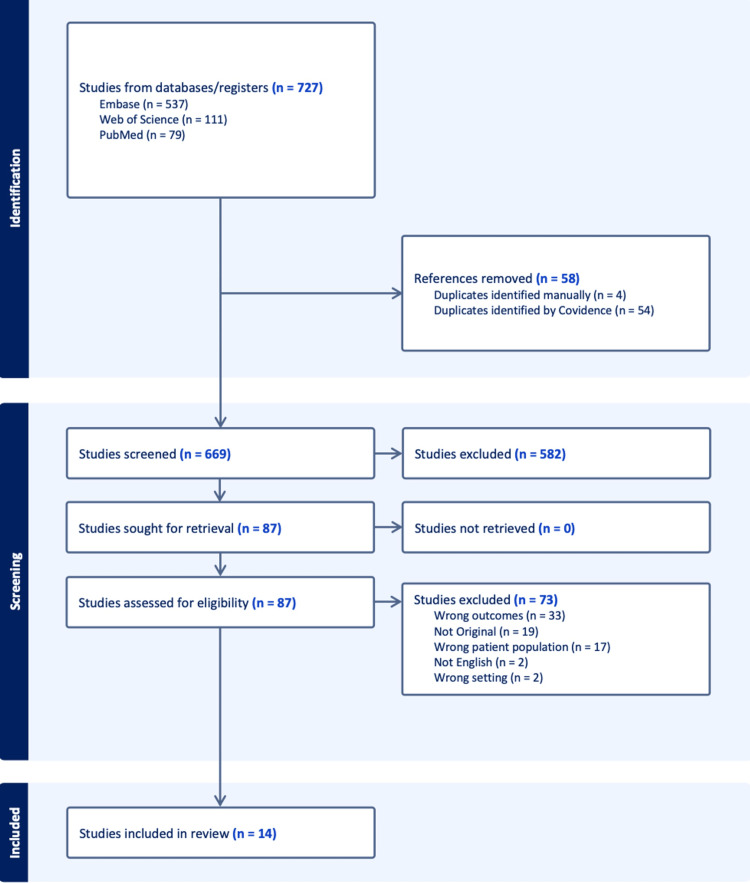 Figure 1
Figure 1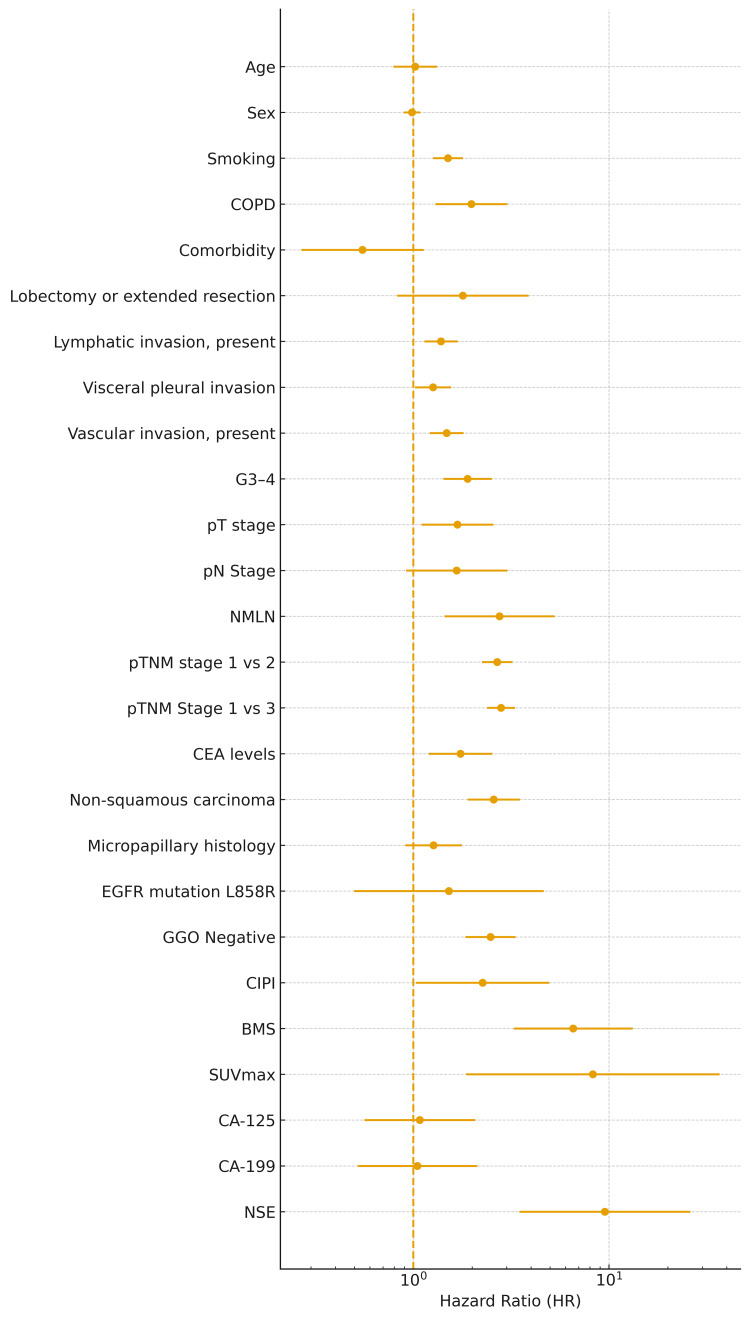 Figure 2
Figure 2| Author | Publication year | Country | Study design | Sample size | Brain metastasis event | Follow-up | Brain metastasis screening |
|
Hubbs et al. [ | 2010 | USA | Retrospective cohort | 975 | 60 | 33 months | No |
|
Kuo et al. [ | 2014 | Taiwan | Retrospective cohort | 181 | 61 | NR | No |
|
Won et al. [ | 2015 | South Korea | Retrospective cohort | 1218 | 87 | 43.6 months | No |
|
Zhang et al. [ | 2016 | China | Retrospective cohort | 637 | NR | 38 months | Yes |
|
Fu et al. [ | 2020 | China | Retrospective cohort | 272 | 35 | NR | No |
|
Li et al. [ | 2020 | China | Retrospective cohort | 332 | 135 | 70 months | Yes |
|
Zhang et al. [ | 2020 | China | Retrospective cohort | 357 | 60 | 40.4 months | No |
|
Liu et al. [ | 2021 | China | Retrospective cohort | 1962 | 30 | NR | No |
|
Deng et al. [ | 2021 | China | Retrospective cohort | 1512 | 118 | 53.2 months | Yes |
|
Mizuno et al. [ | 2021 | Japan | Retrospective cohort | 1099 | 72 | 60.5 months | No |
|
Li et al. [ | 2022 | China | Retrospective cohort | 181 | 64 | ≥60 months | Yes |
|
Liu et al. [ | 2022 | China | Retrospective cohort | 888 | 62 | 54.6 months | No |
|
Zhang et al. [ | 2025 | China | Retrospective cohort | 669 | 69 | NR | No |
|
Motono et al. [ | 2025 | Japan | Retrospective cohort | 1000 | 30 | 52.6 months | NR |
| Risk factor | Pooled HR | 95% CI lower | 95% CI upper | I² (%) |
|
Age [ | 1.02 | 0.79 | 1.32 | 18.62 |
|
Sex [ | 0.98 | 0.89 | 1.09 | 18.78 |
|
Smoking [ | 1.50 | 1.26 | 1.79 | 0 |
|
COPD [ | 1.98 | 1.29 | 3.03 | 0 |
|
Comorbidity [ | 0.55 | 0.27 | 1.13 | 0 |
|
Lobectomy or extended resection [ | 1.79 | 0.83 | 3.88 | 0 |
|
Lymphatic invasion, present [ | 1.38 | 1.14 | 1.69 | 0 |
|
Visceral pleural invasion [ | 1.26 | 1.02 | 1.56 | 9.11 |
|
Vascular invasion, present [ | 1.48 | 1.21 | 1.81 | 0 |
|
G3-4 [ | 1.89 | 1.42 | 2.52 | 8.78 |
|
pT stage [ | 1.68 | 1.10 | 2.57 | 0 |
|
pN Stage [ | 1.66 | 0.92 | 3.02 | 67.48 |
|
NMLN [ | 2.76 | 1.44 | 5.28 | 58.24 |
|
pTNM stage 1 vs. 2 [ | 2.68 | 2.24 | 3.21 | 0 |
|
pTNM Stage 1 vs. 3 [ | 2.80 | 2.38 | 3.30 | 2.02 |
|
CEA levels [ | 1.74 | 1.20 | 2.54 | 0 |
|
Non-squamous carcinoma [ | 2.58 | 1.89 | 3.50 | 0 |
|
Micropapillary histology [ | 1.27 | 0.92 | 1.77 | 51.15 |
|
EGFR mutation L858R [ | 1.52 | 0.50 | 4.64 | 86.12 |
|
GGO Negative [ | 2.48 | 1.85 | 3.33 | 0 |
|
CIPI [ | 2.26 | 1.03 | 4.95 | 0 |
|
BMS [ | 6.56 | 3.26 | 13.21 | 0 |
|
SUVmax [ | 8.27 | 1.86 | 36.77 | 0 |
|
CA-125 [ | 1.08 | 0.56 | 2.08 | 0 |
|
CA-199 [ | 1.05 | 0.52 | 2.12 | 0 |
|
NSE [ | 9.52 | 3.48 | 26.04 | 0 |
| Author | Year | Selection | Comparability | Outcome | Total NOS score |
|
Hubbs et al. [ | 2010 | 3 | 1 | 2 | 6 |
|
Kuo et al. [ | 2014 | 3 | 1 | 2 | 6 |
|
Won et al. [ | 2015 | 3 | 1 | 2 | 6 |
|
Zhang et al. [ | 2016 | 3 | 1 | 2 | 6 |
|
Fu et al. [ | 2020 | 3 | 1 | 2 | 6 |
|
Li et al. [ | 2020 | 4 | 2 | 2 | 8 |
|
Zhang et al. [ | 2020 | 3 | 1 | 2 | 6 |
|
Liu et al. [ | 2021 | 4 | 2 | 2 | 8 |
|
Deng et al. [ | 2021 | 4 | 2 | 2 | 8 |
|
Mizuno et al. [ | 2021 | 4 | 2 | 2 | 8 |
|
Li et al. [ | 2022 | 4 | 2 | 2 | 8 |
|
Liu et al. [ | 2022 | 4 | 2 | 2 | 8 |
|
Zhang et al. [ | 2025 | 4 | 2 | 2 | 8 |
|
Motono et al. [ | 2025 | 4 | 2 | 2 | 8 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBrain Metastases and Treatment · Lung Cancer Research Studies · Lung Cancer Treatments and Mutations
Introduction and background
Non-small cell lung cancer (NSCLC) accounts for approximately 80-85% of all lung malignancies and remains the leading cause of cancer-related mortality worldwide despite advances in diagnostic and therapeutic strategies [1]. Surgical resection is the standard curative modality for patients with early-stage NSCLC, and improved radiological techniques - including low-dose computed tomography (LDCT) - have contributed to increasing detection rates of early-stage disease and prolonged survival [2,3]. Recent evidence from screening trials, including the SUMMIT study, has further emphasized the mortality benefit of early diagnosis through LDCT, underscoring the growing importance of postoperative management in surgically treated populations [3].
Although curative surgery offers favorable long-term survival in early-stage NSCLC, postoperative recurrence remains a clinically significant issue [4]. Among distant recurrence sites, the brain represents one of the most frequent and clinically devastating locations, often leading to neurological symptoms, impaired functional status, and poor quality of life [4]. Existing international and national guidelines, including the National Comprehensive Cancer Network (NCCN, version 2024-2025) and the American Society of Clinical Oncology (ASCO, most recent surveillance guidance), recommend routine postoperative surveillance with chest computed tomography, whereas scheduled brain imaging is not recommended for asymptomatic patients [4]. This recommendation is primarily based on the historically low detection yield of routine brain imaging in unselected postoperative populations, concerns regarding cost-effectiveness, and the lack of clear evidence demonstrating a survival benefit from routine neuroimaging in the absence of neurological symptoms. Consequently, postoperative brain metastases are frequently identified only after the onset of neurological manifestations, which may delay diagnosis and limit timely intervention in routine clinical practice.
In addition, the true incidence of postoperative metachronous brain metastasis remains uncertain due to variations in study design, surveillance strategies, and definitions of recurrence across published studies [5]. Moreover, advances in systemic therapy, including epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors and immune checkpoint inhibitors, may influence recurrence patterns, including a potential impact on brain tropism [6,7]. While several studies have suggested associations between clinicopathological characteristics and brain recurrence, the available evidence remains heterogeneous and fragmented [8,9].
Importantly, a comprehensive synthesis focusing specifically on brain metastasis as the first site of recurrence after curative surgery is lacking. In contrast to prior reviews that pooled heterogeneous recurrence outcomes or unadjusted estimates, the present review was methodologically restricted to studies reporting multivariable-adjusted effect estimates, enabling a more rigorous evaluation of independent risk factors for postoperative intracranial relapse [10]. Consequently, risk stratification strategies capable of identifying high-risk individuals who may benefit from intensified surveillance remain insufficiently defined.
Furthermore, despite increasing availability of local and systemic treatment modalities - including stereotactic radiosurgery (SRS), whole-brain radiotherapy (WBRT), neurosurgical resection, and targeted systemic therapies - the optimal management of postoperative brain recurrence has not been clearly established, and high-quality evidence integrating treatment patterns and prognostic determinants remains limited [6,11].
Therefore, we conducted a systematic review and meta-analysis to determine the incidence of metachronous brain metastasis after curative resection for NSCLC, identify clinicopathological risk factors associated with postoperative brain recurrence, and summarize available evidence on treatment strategies and subsequent survival outcomes. Our findings aim to support future development of risk-adapted postoperative surveillance strategies, refine clinical decision-making, and establish an evidence-based foundation for further prospective investigation.
Review
Study design
This study was conducted as a systematic review and meta-analysis following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines [12]. The protocol was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO) (registry number: CRD420251248812). We included original research reporting postoperative brain metastasis among patients with curatively resected NSCLC.
Data sources and search strategy
A comprehensive literature search was conducted using PubMed, Embase, and Web of Science from January 2010 to October 2025. The search strategy incorporated Medical Subject Headings (MeSH) and free-text terms related to NSCLC, surgical resection, recurrence, and brain metastasis. The following search string was applied: (“lung cancer” OR “non small cell lung cancer” OR NSCLC) AND (“resection” OR “surgical resection” OR “complete resection” OR postoperative OR lobectomy) AND (“recurrence” OR relapse OR “pattern of recurrence” OR “metastatic pattern”) AND (“brain metastasis” OR “CNS metastasis” OR “intracranial metastasis” OR “brain recurrence”).
The full electronic search strategies for each database, including PubMed, Embase, and Web of Science, are provided in Appendices. Only English-language studies were included. Reference lists of eligible studies were manually screened to identify additional citations. However, we acknowledge that exclusion of non-English-language publications may introduce language bias and potentially limit the generalizability of the findings. Reference lists of eligible studies were manually screened to identify additional citations. Unpublished studies, conference abstracts, editorials, and non-peer-reviewed reports were excluded.
Eligibility criteria
Studies were evaluated against predefined inclusion and exclusion criteria focused on population, intervention, outcomes, and design characteristics.
Inclusion Criteria
We included studies enrolling adult patients (≥18 years) with histologically confirmed NSCLC who underwent curative-intent surgical resection (R0). Eligible reports were required to describe postoperative brain metastasis, either as the initial site of recurrence or as part of cumulative follow-up, and to examine associations between clinicopathological features and brain recurrence, or to provide information regarding incidence, management strategies, or survival outcomes. We considered observational designs including prospective and retrospective cohort studies, case-control analyses, registry-based studies, and post-hoc analyses of clinical trials.
Exclusion Criteria
Studies were excluded if they predominantly involved small-cell lung cancer or mixed histologies for which NSCLC-specific data were not extractable, or if surgery was non-curative (R1 or R2 resection). Additional exclusion criteria comprised studies focusing exclusively on synchronous brain metastasis or on non-brain recurrence, as well as animal studies, laboratory investigations, pediatric series, case reports with fewer than 10 patients, narrative reviews, editorials, and conference abstracts. When multiple publications derived from the same cohort were identified, the most complete or most recent analysis was selected.
Study selection
Study selection was performed in two stages. First, two independent reviewers screened titles and abstracts to assess potential eligibility. Subsequently, full texts of selected articles were examined in detail. Any discrepancies regarding study inclusion were resolved through consensus, and involvement of a third reviewer was arranged when necessary. The overall selection process followed the PRISMA recommendations.
Data extraction
Data extraction was carried out independently by two reviewers using a standardized data collection form. Extracted variables included study characteristics, patient demographics, pathological findings, perioperative treatments, incidence and timing of postoperative brain metastasis, and adjusted effect estimates-preferably hazard ratios (HRs) or odds ratios-from multivariable analyses. Only variables for which multivariable-adjusted estimates were reported were included in the pooled analyses of risk factors, to minimize confounding and ensure comparability across studies. Information on treatment modalities following recurrence and on survival outcomes was also collected, along with the duration of follow-up. When reported, molecular and radiological information, such as EGFR mutation, SUVmax, or specific imaging characteristics, was additionally extracted.
Data synthesis
When appropriate data were available, pooled effect estimates were synthesized using random-effects models. HRs or odds ratios (ORs) adjusted in multivariable analyses were prioritized. Statistical heterogeneity was assessed using the I² statistic and Cochran’s Q test. For proportion data of postoperative brain metastasis incidence, a Freeman-Tukey double arcsine variance-stabilizing transformation was applied prior to pooling. Incidence estimates were pooled as cumulative proportions and therefore did not explicitly account for between-study differences in follow-up duration, which varied across cohorts. Publication bias was assessed using funnel plots and Egger’s regression test when ≥10 studies were available. All meta-analyses were conducted using EZR (Easy R) (Yoshiharu Kanda, Jichi Medical University, Saitama, Japan), an updated graphical user interface for R (R Core Team, R Foundation for Statistical Computing, Vienna, Austria), which incorporates the meta (Guido Schwarzer, University of Freiburg, Freiburg, Germany) and metafor packages (Wolfgang Viechtbauer, Maastricht University, Maastricht, Netherlands).
Quality assessment
The methodological quality of included studies was assessed independently by two reviewers using the Newcastle-Ottawa Scale (NOS) for cohort studies, which evaluates selection, comparability, and outcome assessment (maximum score: nine points) [13]. Studies were considered to be of higher quality when they included well-defined surgical cohorts, adequate postoperative follow-up, radiologically confirmed brain metastasis, and multivariable adjustment for key clinicopathological factors. Discrepancies were resolved by consensus. Study quality was not used as an exclusion criterion but was considered when interpreting heterogeneity.
Results
Study Selection
A total of 727 records were initially identified through database searching, including 537 from Embase, 111 from Web of Science, and 79 from PubMed. After removal of 58 duplicates (54 identified automatically by Covidence and four through manual inspection), 669 records were screened based on titles and abstracts. Of these, 582 were excluded for not meeting eligibility criteria.
Eighty-seven full-text articles were assessed for eligibility. After a detailed review, 73 studies were excluded for the following reasons: unrelated outcomes (n = 33), non-original article types such as reviews or editorials (n = 19), ineligible patient population (n = 17), non-English language (n = 2), or inappropriate study setting (n = 2). Ultimately, 14 studies met the eligibility criteria and were included in the qualitative and quantitative synthesis. The study selection process is illustrated in the PRISMA flow diagram (Figure 1).
Selection flow
Characteristics of the Included Articles
A total of 14 retrospective cohort studies published between 2010 and 2025 were included, comprising 13,414 surgically resected NSCLC patients. Geographically, studies were predominantly conducted in Asia, including China (n = 9), Japan (n = 2), South Korea (n = 1), and Taiwan (n = 1), with only one study from the United States. All studies included patients undergoing curative-intent pulmonary resection, most commonly lobectomy with systematic lymph node dissection.
Study sample sizes ranged from 181 to 1,962, and postoperative metachronous brain metastasis events ranged from 30 to 135 per study, yielding a combined total of 883 intracranial recurrences, corresponding to an overall frequency of approximately 6.6% (883/13,414) during postoperative follow-up. Across included studies, brain metastasis was variably defined as either the first site of recurrence or as occurring at any time during follow-up; however, all analyses were restricted to metachronous (postoperative) intracranial events, and studies exclusively reporting synchronous brain metastasis were excluded. Given the limited number of studies consistently reporting first-site recurrence only, these definitions were pooled, and this heterogeneity is acknowledged as a potential source of between-study variability. Median follow-up duration ranged from 33 to 70 months in studies reporting this information.
Across the included articles, adenocarcinoma accounted for 45-100% of cases, and several studies exclusively evaluated adenocarcinoma cohorts. Only a minority of cohorts included substantial proportions of non-adenocarcinoma histology (approximately 20-55%). Several Asian studies reported high proportions of never-smoking patients (approximately 30-75%), consistent with the epidemiology of lung adenocarcinoma in East Asia.
Postoperative screening practices showed notable variation. Only four out of 14 studies (28.6%) incorporated routine scheduled brain MRI as part of follow-up, whereas the remaining studies relied exclusively on symptom-driven neuroimaging. This differential surveillance intensity represents a major source of detection bias. Cohorts without routine brain imaging are likely to under-detect subclinical intracranial metastases, which may lead to underestimation of postoperative brain metastasis incidence and attenuated or inconsistent associations in risk factor analyses. Consequently, variability in surveillance strategies likely contributed to heterogeneity in reported incidence estimates and may partially explain between-study differences in observed postoperative intracranial recurrence rates.
Molecular profiling was available in a subset of studies. Among publications reporting mutation status, EGFR positivity ranged from 55% to 85%, reflecting the high prevalence of driver alterations in Asian adenocarcinoma populations. Other biomarker information, such as SUVmax, was available only in limited cohorts (Table 1).
Results of Meta-Analysis
A total of 14 studies investigating postoperative metachronous brain metastasis among patients with resected NSCLC were included in the meta-analysis. The pooled results demonstrated that several clinicopathological features were significantly associated with an increased risk of postoperative brain metastasis, whereas conventional demographic characteristics showed no consistent association. Forest plots for each risk factor are presented in Figure 2.
Forest plot illustrating pooled hazard ratios for risk factors associated with postoperative brain metastasis in NSCLCForest plot showing pooled hazard ratios (HRs) with corresponding 95% confidence intervals (CIs) for each investigated risk factor in postoperative non-small cell lung cancer (NSCLC). Estimates were calculated using a random-effects model. A logarithmic scale was applied to the x-axis. The vertical dashed line represents HR = 1.0. Variables are ordered according to the predefined dataset order and displayed in reverse order from bottom to top for presentation purposes.Abbreviations: BMS, brain metastasis score; CA-125, cancer antigen-125; CA-199, carbohydrate antigen-19-9; CEA, carcinoembryonic antigen; CIPI, clinical and imaging prognostic index; COPD, chronic obstructive pulmonary disease; EGFR, epidermal growth factor receptor; G3-4, pathological grade 3-4; GGO, ground-glass opacity; NMLN, number of metastatic lymph nodes; NSE, neuron-specific enolase; pN, pathological N stage; pT, pathological T stage; pTNM, pathological TNM stage; SUVmax, maximum standardized uptake value; TNM, tumor-node-metastasis
Pooled HRs for risk factors of postoperative brain metastasis in NSCLC are summarized in Table 2.
Demographic and Baseline Clinical Characteristics
Age (analyzed as a continuous variable or binomial) was not significantly associated with metachronous brain metastasis (pooled HR = 1.02, 95% CI 0.79-1.32, I² = 18.6%). Similarly, male sex showed no significant association (HR = 0.98, 95% CI 0.89-1.09, I² = 18.8%). Smoking status (current/former vs never) was significantly associated with an increased risk of brain metastasis (HR = 1.50, 95% CI 1.26-1.79, I² = 0.0%). In contrast, chronic obstructive pulmonary disease (COPD) was evaluated in only one study, which reported a higher risk (HR = 1.98, 95% CI 1.29-3.03). Comorbidity burden (comorbidity score) was also reported by a single study and suggested a non-significant tendency towards reduced risk (HR = 0.55, 95% CI 0.27-1.13), although precision was limited.
Tumor Histology and Pathological Differentiation
Non-squamous carcinoma histology was strongly associated with a higher incidence of brain metastasis (HR = 2.58, 95% CI 1.89-3.50, I² = 0.0%). Within this group, micropapillary histology showed a tendency towards increased risk but did not reach statistical significance (HR = 1.27, 95% CI 0.91-1.77, I² = 51.1%). Poorly differentiated tumors (G3-4) were significantly associated with brain metastasis (HR = 1.89, 95% CI 1.42-2.52, I² = 8.8%), indicating that histological grade is an important determinant.
Invasion-Related Pathological Features
Lymphatic invasion was one of the most consistent pathological predictors. The presence of lymphatic invasion significantly increased the risk of brain metastasis (HR = 1.39, 95% CI 1.14-1.69, I² = 0.0%). Visceral pleural invasion was also significantly associated with brain metastasis (HR = 1.26, 95% CI 1.02-1.56, I² = 9.1%). Similarly, vascular invasion conferred a significantly elevated risk (HR = 1.48, 95% CI 1.21-1.81, I² = 0.0%). These findings indicate that invasion beyond the primary tumor, particularly into lymphatic and vascular structures and the visceral pleura, is consistently linked to postoperative brain relapse.
Tumor Size, T Category, and Lymph Node Involvement
Pathological T category was significantly associated with metachronous brain metastasis (HR = 1.68, 95% CI 1.10-2.57, I² = 0.0%), suggesting that more locally advanced primary tumors are at higher risk. Pathological N stage showed a trend toward increased risk, but the pooled estimate was not statistically significant and exhibited substantial heterogeneity (HR = 1.66, 95% CI 0.92-3.02, I² = 67.5%). This heterogeneity may reflect differences across studies in nodal staging systems, extent of lymph node dissection, pathological assessment, and use of adjuvant therapies, all of which could influence both nodal classification and subsequent risk of intracranial recurrence. In contrast, a more quantitative assessment of nodal burden demonstrated a clearer association: the number of metastatic lymph nodes (NMLN) was significantly associated with brain metastasis (HR = 2.76, 95% CI 1.44-5.28, I² = 58.2%). Lymph node-related composite indices such as CIPI and BMS were each evaluated in single studies and showed elevated risks (CIPI: HR = 2.26, 95% CI 1.03-4.95; BMS: HR = 6.56, 95% CI 3.26-13.21).
Pathological TNM Stage
A higher pathological TNM stage was consistently associated with a substantially increased risk of brain metastasis. Compared with stage I, pathological stage II had a pooled HR of 2.68 (95% CI 2.24-3.21, I² = 0.0%), and stage III had a pooled HR of 2.80 (95% CI 2.38-3.30, I² = 2.0%). These findings highlight that overall pathological stage, integrating T and N status, is a robust stratifier of brain metastasis risk after surgery.
Surgical Procedure
The extent of resection was evaluated in terms of lobectomy or extended resection. Patients undergoing lobectomy or extended resection showed a non-significant trend towards higher risk (HR = 1.79, 95% CI 0.83-3.88, I² = 0.0%). Segmentectomy and wedge resection were reported less consistently and could not be pooled.
Molecular Marker: EGFR Mutation
EGFR mutation (L858R) was evaluable in two studies. Other EGFR mutation subtypes, including exon 19 deletion, were not pooled because they were either inconsistently reported or lacked multivariable-adjusted effect estimates across studies. The pooled analysis for L858R yielded an HR of 1.52 (95% CI 0.50-4.64, I² = 86.1%). Although the point estimate suggested a higher risk of metachronous brain metastasis among patients with EGFR-mutated tumors, the wide confidence interval and substantial heterogeneity preclude definitive conclusions. These results nonetheless indicate that EGFR mutation may contribute to brain tropism, warranting further investigation in larger, standardized cohorts.
Serum Biomarkers and Metabolic Parameters
Among serum biomarkers, elevated CEA levels were significantly associated with increased risk of brain metastasis (HR = 1.74, 95% CI 1.20-2.54, I² = 0.0%). Other tumor markers were each reported in single studies: CA-125 (HR = 1.08, 95% CI 0.56-2.08), CA19-9 (HR = 1.05, 95% CI 0.52-2.12), and NSE (HR = 9.52, 95% CI 3.48-26.04). While NSE showed markedly elevated HR, the evidence is currently limited to a single study. Maximum standardized uptake value (SUVmax) on PET was also examined in a single study. It showed a considerable increase in risk (HR = 8.27, 95% CI 1.86-36.77), suggesting that high metabolic activity might be linked with subsequent brain metastasis.
Imaging-Related and Composite Risk Indices
Ground-glass opacity (GGO) status was reported in one study, where the absence of GGO (GGO negative) was associated with a higher risk of brain metastasis (HR = 2.48, 95% CI 1.85-3.33). Two composite indices, the clinical prognostic index (CIPI) and brain metastasis score (BMS), also showed significant associations in single studies (CIPI HR = 2.26, 95% CI 1.03-4.95; BMS HR = 6.56, 95% CI 3.26-13.21), indicating the potential utility of multivariable risk stratification tools, although external validation remains limited.
Quality Assessment
Quality assessment was conducted using the NOS for observational cohort studies, focusing on three domains: selection, comparability, and outcome assessment. All 14 studies adopted a retrospective cohort design and met the criteria for adequate cohort selection, including histologically confirmed NSCLC and curative-intent resection. Most studies reported well-defined eligibility criteria and postoperative follow-up periods sufficient for detecting metachronous brain metastasis (median follow-up 33-70 months).
Comparability between exposure groups was generally acceptable, as the majority of studies adjusted for key prognostic variables such as pathological stage, tumor differentiation, lymphovascular invasion, and smoking status in multivariable analyses. However, the extent of covariate adjustment varied among studies, and only a subset incorporated molecular markers or postoperative therapy in their multivariable models.
Outcome assessment was based primarily on radiologic confirmation of postoperative brain metastasis across studies, although brain imaging strategies differed substantially. Several studies relied on symptom-triggered neuroimaging, whereas others incorporated routine postoperative brain MRI, potentially introducing detection bias. The definition of postoperative brain failure (initial versus cumulative site of recurrence) also varied, contributing to heterogeneity among reported outcomes (Table 3).
Discussion
Summary of the Study
In this systematic review and meta-analysis involving 14 retrospective cohort studies and more than 13,000 patients undergoing curative-intent resection for NSCLC, we examined the incidence and determinants of postoperative metachronous brain metastasis. Across included studies, adenocarcinoma was the dominant histological subtype, and the majority of patients were treated in Asian surgical cohorts with long-term follow-up. Although the reported incidence of postoperative brain metastasis varied owing to differences in imaging strategies and study design, our findings confirm that metachronous brain recurrence remains a clinically relevant pattern of disease progression, particularly among patients with adverse clinicopathological features. Furthermore, several molecular characteristics-including EGFR mutation-have been investigated as potential predictors of intracranial failure; however, the available evidence remains inconsistent and highly heterogeneous, and pooled estimates did not demonstrate a robust or reproducible association. In contrast, clinicopathological factors showed more consistent and stable associations across multivariable analyses, suggesting that molecular predictors alone are currently insufficient for reliable postoperative risk stratification of brain recurrence.
Given that a proportion of postoperative brain metastases are detected only after neurological presentation, our findings highlight the potential clinical relevance of risk-adapted postoperative neuroimaging. However, this concept should be regarded as hypothesis-generating, as none of the included studies directly evaluated surveillance strategies or compared scheduled versus symptom-driven brain imaging. In particular, whether scheduled brain imaging may benefit selected high-risk individuals remains an important unanswered question and represents a key motivation for further prospective investigation.
Comparison With Other Studies
Prior systematic reviews have described recurrence patterns following resection for early-stage NSCLC, yet few have focused specifically on metachronous brain metastasis as the primary outcome [28-30]. Several studies have reported higher rates of brain recurrence in adenocarcinoma and EGFR-mutant populations, reflecting the changing epidemiology of NSCLC in East Asian cohorts [31,32]. Our findings are partially consistent with these observations; however, the magnitude and consistency of association between EGFR mutation and postoperative brain metastasis were less pronounced in our pooled analysis compared with earlier reports. These discrepancies may be attributable to differences in study populations, evolving molecular testing strategies, and competing pathological determinants that were simultaneously evaluated in multivariable models.
Conversely, several clinicopathological and host-related factors that have received comparatively less attention in prior recurrence analyses demonstrated more robust and consistent associations in our synthesis. Specifically, lymph node involvement, visceral pleural invasion, tumor differentiation, smoking status, and the presence of chronic pulmonary comorbidity, such as COPD, emerged as independent predictors of metachronous intracranial failure across multiple adjusted models [33-35]. These observations suggest that classical pathological and clinical factors continue to play a central role in determining brain recurrence risk even in the molecular era, and that reliance solely on genomic markers may underestimate the contribution of fundamental disease biology and host susceptibility.
Notably, the absence of routine postoperative brain imaging in earlier cohorts likely led to an underestimation of intracranial relapse, underscoring the need for risk-adapted surveillance strategies [36]. Future studies should therefore integrate standardized imaging protocols, contemporary biomolecular testing, and comprehensive adjustment for clinicopathological determinants to clarify the relative prognostic weight of genomic versus traditional risk factors in surgically treated NSCLC.
Strengths of the Study
This review synthesizes contemporary evidence across 15 years of surgical oncology practice, integrating clinical, pathological, radiologic, and molecular determinants of postoperative brain failure. The inclusion of more than 13,000 resected NSCLC cases enables risk estimation in real-world surgical cohorts across different regions and healthcare systems. Rigorous study selection, predefined eligibility criteria, and structured quality assessment provide a reliable methodological foundation for interpreting pooled estimates.
Importantly, by focusing exclusively on metachronous brain metastasis following curative-intent surgery, our analysis addresses a clinically relevant gap that has been insufficiently characterized in previous recurrence studies. Although EGFR mutation has long been recognized as a potential driver of brain tropism in NSCLC, our findings suggest that the association may be less consistent than generally assumed in the surgical setting, particularly when compared with fundamental pathological and clinical features [37]. Lymph node involvement, visceral pleural invasion, histologic differentiation, smoking history, and comorbid conditions such as COPD demonstrated more consistent associations with postoperative brain recurrence across multivariable analyses. These results highlight that traditional tumor biology and host-related clinical factors remain key determinants of intracranial relapse risk beyond molecular profile alone, underscoring the need for future models that integrate both classical clinicopathological parameters and contemporary genomic information. Such integrated risk stratification has important clinical implications for multidisciplinary postoperative planning, including coordination among thoracic surgeons, medical oncologists, radiation oncologists, and radiologists when considering follow-up strategies and early intervention for high-risk patients.
Limitations
Several limitations inherent to the available literature should be recognized. First, all included studies were retrospective observational cohorts, which may introduce selection bias and residual confounding despite multivariable adjustment in most analyses. Second, considerable heterogeneity existed in postoperative brain imaging strategies. While a minority of studies incorporated scheduled brain MRI surveillance, the majority relied on symptom-driven neuroimaging, which may have led to delayed detection of subclinical intracranial recurrence and an underestimation of the true metachronous incidence. The variability in imaging modality, surveillance interval, and clinical threshold for neuroimaging likely contributed to detection bias and heterogeneity across studies. In addition, differences in follow-up duration and timing of recurrence assessment may have introduced time-to-event bias, and competing risks, particularly postoperative mortality, were not uniformly accounted for across studies. These factors may have influenced both incidence estimates and HR calculations in postoperative cohorts.
Third, although effect estimates were derived primarily from multivariable analyses, the selection of covariates included in these models differed substantially among studies. Some models adjusted for classical pathological parameters such as nodal stage, tumor differentiation, and lymphovascular invasion. In contrast, others incorporated molecular markers or adjuvant treatment variables, resulting in inconsistent adjusted HRs. As a result, pooled estimates reflect partially harmonized effect sizes rather than fully standardized prognostic comparisons and should therefore be interpreted with caution.
Fourth, molecular and genomic profiling was inconsistently reported, and even among studies with available genetic data, the inclusion of biomarkers (such as EGFR, PD-L1, or other driver alterations) in multivariable models varied markedly. Likewise, reporting of adjuvant chemotherapy and radiotherapy was heterogeneous, precluding comprehensive evaluation of treatment-related modifiers of brain recurrence.
Finally, most included cohorts originated from East Asian populations, in which the prevalence of adenocarcinoma and EGFR-mutant disease is significantly higher than in Western populations. These epidemiologic and biological differences may limit the generalizability of our findings and highlight the need for future prospective studies including diverse populations and standardized neuro-oncological follow-up protocols. In particular, external validation in Western and multi-ethnic cohorts will be essential to confirm the applicability of these risk factors across different healthcare systems and genomic backgrounds [38].
Conclusions
Metachronous brain metastasis represents a clinically relevant pattern of recurrence after curative-intent resection for NSCLC. Robust clinicopathological factors-such as nodal involvement, visceral pleural invasion, tumor differentiation, and adenocarcinoma histology-were most consistently associated with postoperative intracranial relapse in multivariable analyses. In contrast, molecular characteristics, including EGFR mutation, showed heterogeneous and inconclusive associations, limiting their current utility as standalone predictors. These findings support the development of personalized postoperative surveillance strategies primarily grounded in clinicopathological risk stratification. In this context, whether selected high-risk patients may benefit from scheduled, rather than purely symptom-driven, postoperative brain imaging remains an important hypothesis-generating clinical question. Prospective, multi-center studies incorporating uniform imaging protocols and comprehensive molecular evaluation will be required to refine risk stratification and to determine whether intensified neurological follow-up can improve early detection and outcomes in resected NSCLC.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Recent advances in non-small cell lung cancer targeted therapy; an update review Cancer Cell Int Araghi M Mannani R Heidarnejad Maleki A 1622320233756819310.1186/s 12935-023-02990-y PMC 10416536 · doi ↗ · pubmed ↗
- 2Cancer progress and priorities: lung cancer Cancer Epidemiol Biomarkers Prev Schabath MB Cote ML 156315792820193157555310.1158/1055-9965.EPI-19-0221 PMC 6777859 · doi ↗ · pubmed ↗
- 3Low-dose CT for lung cancer screening in a high-risk population (SUMMIT): a prospective, longitudinal cohort study Lancet Oncol Bhamani A Creamer A Verghese P 6096192620254015451410.1016/S 1470-2045(25)00082-8 · doi ↗ · pubmed ↗
- 4Follow up and surveillance post lung cancer surgery: a narrative review Video-Assist Thorac Surg Philip B Jain A Ramesh P 282023
- 5Survival and quality of life after first-time diagnosis of brain metastases: a multicenter, prospective, observational study Lancet Reg Health Eur Yri OE Astrup GL Karlsson AT 1011814920253980715310.1016/j.lanepe.2024.101181 PMC 11728971 · doi ↗ · pubmed ↗
- 6Comprehensive analysis of lung cancer metastasis: sites, rates, survival, and risk factors—a systematic review and meta-analysis Clin Respir J Wang S Tang W Jin F Luo H Yang H Wang Y 019202510.1111/crj.70107 PMC 1225419140650339 · doi ↗ · pubmed ↗
- 7Advances in molecular pathology and therapy of non-small cell lung cancer Signal Transduct Target Ther Huang Q Li Y Huang Y 1861020254051716610.1038/s 41392-025-02243-6PMC 12167388 · doi ↗ · pubmed ↗
- 8Clinicopathological factors related to recurrence patterns of resected non-small cell lung cancer J Clin Med Shimizu R Kinoshita T Sasaki N 39202010.3390/jcm 9082473 PMC 746564932752198 · doi ↗ · pubmed ↗