Therapeutic Algorithm for Extramammary Paget Disease: Experience in a Dermatology Referral Center in Western Mexico
Michelle Alcocer Salas, Diana L Vazquez-Cantu, Mercedes Hernández Torres, Víctor Manuel Tarango-Martinez

TL;DR
This paper presents a diagnostic and treatment algorithm for extramammary Paget disease based on 10 patient cases from a Mexican dermatology center.
Contribution
A novel diagnostic and therapeutic algorithm for EMPD based on institutional experience and clinical outcomes.
Findings
All 10 cases confirmed primary EMPD with no associated internal malignancies.
Surgical excision with wide margins was the treatment of choice in all patients.
A CK7-positive/CK20-negative immunohistochemical profile confirmed primary EMPD in 60% of cases.
Abstract
Introduction Extramammary Paget disease (EMPD) is a rare intraepithelial adenocarcinoma that predominantly affects areas rich in apocrine glands. Its chronic and nonspecific clinical presentation frequently leads to misdiagnosis and delayed treatment. Objective The primary objective is to describe the clinical, epidemiological, histopathological, and therapeutic characteristics of patients with EMPD treated at a dermatology referral center. The secondary outcome is to propose a diagnostic and therapeutic algorithm based on institutional experience. Methods A single-center, retrospective, observational case series was conducted at the Instituto Dermatológico de Jalisco. All patients with histopathologically confirmed EMPD diagnosed between 2011 and 2025 were included. Demographic, clinical, histopathological, immunohistochemical, and therapeutic data were analyzed.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
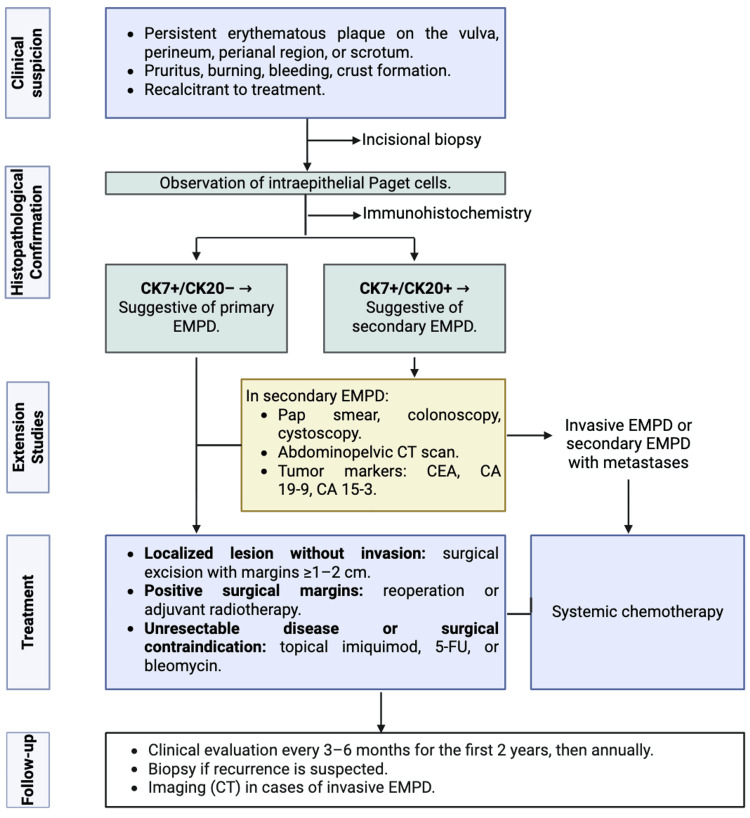 Figure 1
Figure 1| Case | Age (years) | Sex | Topography | Morphology | Evolution (months) | Clinical symptoms | Initial diagnostic suspicion | Histopathology | Associated neoplasia | Immunohistochemistry | Treatment |
| 1 | 86 | F | Vulva | Erythematous ulcerated plaque | 48 | Pruritus | SCC vs. erosive lichen planus vs. vulvitis | Intraepidermal Paget cells | No | CK7+, CK20- | Surgical |
| 2 | 63 | F | Suprapubic | Erythematous plaque with scaling and blue pigment | 18 | None | Basal cell carcinoma | Intraepidermal Paget cells | No | Not performed | Surgical |
| 3 | 66 | F | Vulva and perineum | Erythematous plaque with excoriations | 12 | Pruritus | EMPD | Intraepidermal Paget cells | No | Not performed | Surgical |
| 4 | 73 | F | Vulva | Whitish plaques | 6 | None | EMPD | Intraepidermal Paget cells | History of vulvar carcinoma | Not performed | Surgical |
| 5 | 60 | F | Vulva | Ulcerated and bleeding neoformations | 12 | Pain | Lichen sclerosus | Intraepidermal Paget cells | No | CK7+, CK20- | Surgical |
| 6 | 81 | F | Vulva | Macerated plaques | 60 | None | Lichen sclerosus | Intraepidermal Paget cells | No | CK7+, CK20- | Surgical |
| 7 | 57 | F | Perineum | Ulcerated erythematous neoformation | 12 | None | Melanoma vs. basal cell carcinoma | Intraepidermal Paget cells | No | CK7+, MELAN-A- | Surgical |
| 8 | 66 | F | Vulva and perineum | Hyperkeratotic plaque with hypo-/hyperpigmentation | 4 | None | EMPD vs. Bowen disease | Intraepidermal Paget cells | No | CK7+, CK20- | Surgical |
| 9 | 72 | F | Vulva | Erythematous plaque with vesicles and ulceration | 24 | None | Pemphigus vulgaris vs. erosive lichen planus vs. EMPD | Intraepidermal Paget cells | No | CK7+, CK20- | Surgical |
| 10 | 73 | M | Scrotum | Erythematous and scaly plaque | 1 | None | Psoriasis vs. contact dermatitis | Intraepidermal Paget cells | No | Not performed | Surgical |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer and Skin Lesions · Hedgehog Signaling Pathway Studies · Genetic and rare skin diseases.
Introduction
Extramammary Paget disease (EMPD) is a rare intraepithelial adenocarcinoma that predominantly arises in areas rich in apocrine glands, including the vulva, perianal region, scrotum, and less commonly the axillae and umbilicus. It is an uncommon malignancy, with an estimated incidence of approximately 0.12 cases per 100 million individuals annually, underscoring its extreme rarity and the limited availability of large prospective studies [1].
Clinically, EMPD typically presents as chronic, persistent, well-demarcated erythematous plaques, frequently accompanied by scaling, ulceration, crusting, bleeding, or pigmentary changes. Symptoms such as pruritus, burning sensation, and pain are common, although up to 10% of patients may remain asymptomatic [2]. Due to its nonspecific presentation, EMPD is frequently misdiagnosed as more common inflammatory dermatoses, including eczema, psoriasis, candidiasis, or erosive lichen planus, leading to substantial diagnostic delay and prolonged morbidity [2].
Histopathological examination remains the cornerstone of diagnosis, demonstrating characteristic large pale Paget cells within the epidermis. Immunohistochemistry (IHC) plays an important adjunctive role, particularly in distinguishing primary cutaneous EMPD from secondary disease associated with underlying internal malignancies. A cytokeratin 7 (CK7)-positive and cytokeratin 20 (CK20)-negative profile supports a primary cutaneous origin, whereas CK20 positivity may suggest secondary involvement from gastrointestinal or urothelial primaries [3,4].
Management of EMPD remains challenging due to its high recurrence rates and potential association with internal malignancies. Surgical excision with wide margins remains the standard of care, although radiotherapy, topical therapies, and systemic treatments have been reported in selected cases, particularly when surgery is not feasible or margins are positive [5].
Given the rarity of EMPD, most available evidence derives from small institutional case series. Studies conducted in dermatology referral centers are particularly valuable, as they provide real-world insight into diagnostic challenges, treatment patterns, and outcomes in specialized clinical settings. The present study aims to describe the clinical, histopathological, and therapeutic characteristics of patients with EMPD treated at a tertiary dermatology referral center in western Mexico. Additionally, we propose a pragmatic diagnostic and therapeutic algorithm based on institutional experience to assist clinicians in the evaluation and management of this uncommon malignancy.
Materials and methods
Study design and setting
This was a single-center, retrospective, observational case series conducted at the Instituto Dermatológico de Jalisco, a tertiary dermatology referral center in western Mexico.
Study population
All patients diagnosed with EMPD between January 2011 and May 2025 were identified through the institutional histopathology database and clinical records.
Inclusion Criteria
All cases with histopathological confirmation of EMPD were included in the study.
Exclusion Criteria
No exclusion criteria were applied.
Data collection
Clinical and pathological information was obtained from electronic and physical medical records. Variables collected were grouped as follows: demographic variables: age and sex; clinical variables: lesion location, morphology, symptoms, duration of disease, and initial clinical diagnosis; pathological variables: histopathological findings; IHC variables: CK7 and CK20 expression; evaluation of associated malignancy: staging investigations; and therapeutic variables: treatment modality and surgical margins.
Histopathology and IHC
All diagnoses were confirmed by histopathological examination, identifying characteristic intraepidermal Paget cells. IHC studies were performed selectively in cases with clinical or histopathological suspicion of secondary EMPD and were not applied routinely to all patients. The primary markers used were CK7 and CK20 to differentiate primary from secondary disease. Additional markers (e.g., GCDFP-15 and HER2) were not required due to consistent immunophenotypic profiles.
Staging and evaluation of associated malignancy
Staging investigations were requested only when clinically indicated and included gynecologic examination and Papanicolaou smear, colonoscopy, cystoscopy, abdominopelvic computed tomography (CT), and tumor markers (carcinoembryonic antigen (CEA), carbohydrate antigen (CA) 19-9, and CA 15-3). These assessments were performed to rule out underlying or associated malignancies in cases with suspected secondary EMPD.
Treatment
Treatment decisions were individualized based on lesion size and anatomical location, histopathological findings, surgical margin status, patient comorbidities and functional status, and institutional surgical protocol. All patients underwent wide-margin surgical excision, with margins ranging from 1 to 2 cm, in accordance with institutional practice and published recommendations.
Ethical considerations
This study was conducted in accordance with the Declaration of Helsinki and its later amendments. Due to its retrospective nature, formal approval from the institutional ethics committee was waived. All patient data were anonymized to ensure confidentiality.
Statistical analysis
Descriptive statistics were used. Categorical variables are presented as frequencies and percentages, and continuous variables as medians with ranges.
Results
A total of 10 patients with EMPD were included in the study (N = 10). There was a marked female predominance, with nine women (90%) and one man (10%), yielding a female-to-male ratio of 9:1. The median age at diagnosis was 69 years (range: 57-86 years).
Clinical characteristics
Lesions were most frequently localized to the vulva in seven patients (70%), followed by the perianal region in two patients (20%) and the scrotum in one patient (10%). All patients presented with chronic, well-demarcated erythematous plaques. Additional clinical features included ulceration, maceration, scaling, vesiculation, bleeding, and pigmentary changes. Pruritus and burning sensations were the most commonly reported symptoms, although four patients (40%) were asymptomatic at presentation.
The duration of symptoms prior to diagnosis ranged from two to 60 months. The median diagnostic delay was 20 months, reflecting a substantial delay in clinical recognition in several cases.
Initial clinical suspicion
Initial clinical diagnoses before histopathological confirmation included inflammatory dermatoses in six patients (60%), such as contact dermatitis, psoriasis, erosive lichen planus, and lichen sclerosus. In the remaining four patients (40%), neoplastic conditions were suspected, including squamous cell carcinoma, basal cell carcinoma, melanoma, and EMPD. One patient (10%) had a documented previous history of vulvar carcinoma.
Histopathology and IHC
Histopathological examination confirmed EMPD in all cases (100%), demonstrating characteristic intraepidermal Paget cells. IHC analysis was performed in six patients (60%) based on clinical or histopathological suspicion of possible secondary disease. All tested cases demonstrated a CK7-positive/CK20-negative immunophenotype, supporting a primary cutaneous origin. Therefore, all cases in this cohort were classified as primary EMPD. Additional markers, including GCDFP-15 and HER2, were not required, as the CK7/CK20 profile was sufficient for diagnostic classification.
Evaluation for associated malignancy
Staging investigations were carried out in the same six patients who underwent IHC evaluation. These included gynecologic examination with Papanicolaou smear, colonoscopy, cystoscopy, abdominopelvic CT, and tumor marker analysis. No underlying or associated internal malignancies were identified in any patient.
Treatment
All patients (100%) underwent wide-margin surgical excision as primary treatment, with surgical margins ranging from 1 to 2 cm. Patients with positive margins were referred for re-excision or considered for adjuvant radiotherapy according to institutional protocol.
Summary of cases
The detailed clinical, histopathological, and therapeutic characteristics of all patients are summarized in Table 1. The heterogeneity in clinical presentation and frequent initial misdiagnosis highlight the diagnostic challenges associated with EMPD and emphasize the importance of early biopsy in persistent genital or perianal lesions.
Discussion
EMPD remains a rare cutaneous malignancy associated with significant diagnostic and therapeutic challenges. In this single-center case series from a dermatology referral center, we describe the clinical and pathological characteristics of 10 patients and propose an experience-based diagnostic and therapeutic algorithm. Our cohort demonstrated a marked female predominance (90%) and a median age at diagnosis of 69 years, findings consistent with previously published series reporting a higher prevalence among elderly women [6,7].
The vulva was the most commonly affected site (70%), followed by the perianal region (20%) and scrotum (10%). This anatomical distribution closely mirrors reports in the literature, where vulvar involvement accounts for approximately 65%-70% of cases [6,8], supporting the external validity of our findings despite the inherent limitations associated with small sample sizes in rare diseases.
From a clinical perspective, EMPD continues to pose diagnostic difficulty due to its nonspecific presentation. In our series, 60% of patients were initially misdiagnosed with inflammatory dermatoses, including lichen sclerosus, erosive lichen planus, and contact dermatitis. This misdiagnosis rate aligns with previously reported figures ranging from 40% to 70% [7,9]. The median diagnostic delay of 20 months reflects prolonged symptom duration prior to biopsy. Although this delay is shorter than the up to 43 months described in other studies [9,10], it remains clinically significant and highlights the need for heightened clinical suspicion and early biopsy of persistent anogenital plaques.
Histopathological examination confirmed the diagnosis in all cases. IHC was selectively employed in patients with suspicion of secondary disease. All tested cases demonstrated a CK7-positive and CK20-negative immunophenotype, confirming a primary cutaneous origin. Consequently, all cases in this cohort were classified as primary EMPD. This finding is clinically relevant, as secondary EMPD is associated with underlying internal malignancies and requires a distinct diagnostic approach [10,11].
Staging investigations performed in selected patients revealed no associated internal malignancies. This is an important observation, as it supports evidence suggesting lower rates of associated neoplasia in vulvar-predominant cohorts compared with perianal or male genital involvement [6,8,12]. The absence of secondary malignancies in our cohort reinforces the importance of individualized staging based on clinical and histopathological features rather than routine extensive screening in all patients.
Surgical excision with wide margins remains the standard of care and was performed in all patients in this series. However, recurrence rates remain high even after apparently complete excision, as consistently reported in the literature [10-12]. For this reason, adjuvant therapies, including radiotherapy and topical treatments, may be considered in selected cases, particularly in patients with positive margins or contraindications to surgery.
The principal contribution of this study is the translation of institutional experience into a pragmatic diagnostic and therapeutic algorithm (Figure 1). By integrating early clinical suspicion, prompt histopathological confirmation, selective use of IHC, and individualized staging, this framework provides a structured approach to management in referral centers. Importantly, this algorithm should be interpreted as hypothesis-generating and experience-based rather than prescriptive or evidence of therapeutic superiority.
Diagnostic and Therapeutic Algorithm for Extramammary Paget Disease (EMPD)CT: computed tomography; CEA: carcinoembryonic antigen; CA: carbohydrate antigen; 5-FU: 5-fluorouracil
This study has several limitations. The small sample size, retrospective design, and single-center setting limit generalizability. Additionally, long-term outcomes such as recurrence rates, disease-free survival, and standardized follow-up were not evaluated. Furthermore, the proposed algorithm has not been formally validated or compared with existing management strategies, which should be considered when interpreting these findings.
Despite these limitations, this series provides valuable real-world data from a specialized referral center and contributes to the growing body of literature on this rare malignancy. Future multicenter prospective studies with standardized outcome measures are needed to validate diagnostic pathways, optimize treatment strategies, and refine follow-up protocols.
Conclusions
EMPD is an uncommon malignancy with a chronic and nonspecific clinical presentation that frequently leads to diagnostic delay and initial mismanagement. Early clinical suspicion and prompt biopsy of persistent genital or perianal lesions are essential to achieve a timely and accurate diagnosis. In this single-center case series, all patients were classified as having primary EMPD, and no associated internal malignancies were identified, underscoring the importance of selective rather than routine extensive staging based on clinical and histopathological features. Surgical excision with wide margins remains the standard of care and was successfully implemented in all cases.
The diagnostic and therapeutic algorithm proposed in this study provides a structured, experience-based framework to guide clinical decision-making in referral centers. However, this approach should be interpreted as hypothesis-generating rather than prescriptive. Future multicenter prospective studies with standardized outcome measures are needed to validate this strategy and to optimize diagnostic pathways, treatment selection, and follow-up protocols for patients with EMPD.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Extramammary Paget's disease: updates in the workup and management Asian J Urol Nabavizadeh R Vashi KB Nabavizadeh B Narayan VM Master VA 451459920223638159610.1016/j.ajur.2022.08.001PMC 9643171 · doi ↗ · pubmed ↗
- 2Extramammary Paget disease Dermatol Online J St Claire K Hoover A Ashack K Khachemoune A 25201931046904 · pubmed ↗
- 3Mammary and extramammary Paget's disease An Bras Dermatol Lopes Filho LL Lopes IM Lopes LR Enokihara MM Michalany AO Matsunaga N 2252319020152583099310.1590/abd 1806-4841.20153189 PMC 4371672 · doi ↗ · pubmed ↗
- 4Extramammary Paget's disease: summary of current knowledge Dermatol Clin Lam C Funaro D 8078262820102088392210.1016/j.det.2010.08.002 · doi ↗ · pubmed ↗
- 5Current management and treatment of extramammary Paget's disease Curr Treat Options Oncol Hashimoto H Ito T 8188302320223537710110.1007/s 11864-021-00923-3 · doi ↗ · pubmed ↗
- 6Extramammary Paget disease Bahsas Zaky O Puckett Y Treasure Island (FL)Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 493224/29630276 · pubmed ↗
- 7Tumor thickness as a prognostic factor in extramammary Paget's disease J Dermatol Ito T Kaku Y Nagae K 2692754220152555743410.1111/1346-8138.12764 · doi ↗ · pubmed ↗
- 8Extramammary Paget disease: a therapeutic challenge, for a rare entity Curr Oncol Rep Pérez JC Salgado AC Pérez-Mies B Rullán JA Ajuria-Illarramendi O Alia EM Serrano Domingo JJ 108110942520233742158310.1007/s 11912-023-01434-0PMC 10556167 · doi ↗ · pubmed ↗