Association between the ownership of home-based records and continuous, quality maternal and child health service utilisation: a multi-country analysis of Demographic Health Surveys from 18 low- and middle-income countries
Akiko Saito, Masahide Kondo

TL;DR
This study finds that owning health records is linked to better maternal and child health care, but no major differences were found between specific types of health records.
Contribution
The study provides new evidence on how health record ownership affects the quality and continuity of maternal and child health services in low- and middle-income countries.
Findings
Ownership of home-based records is associated with higher odds of completing quality maternal and child health care.
No significant differences were found between integrated Maternal and Child Health Handbooks and other health record types in facilitating care continuity.
MCHHBs may better support specific antenatal services like urine and blood tests compared to other health records.
Abstract
The continuity and quality of maternal and child health (MCH) services represent significant challenges in low- and middle-income countries (LMICs). Home-based records (HBRs), including the integrated Maternal and Child Health Handbook (MCHHB), may support consistent service usage and improved care quality. We aimed to evaluate the association between HBRs and continued quality MCH care, identifying differences in associations between MCHHBs and the continuum of care and those between other HBR types and the continuum of care. We conducted a pooled analysis of Demographic and Health Surveys (DHS) from 18 LMICs, including women and their youngest eligible children for the health card module. We defined the continuum of quality MCH care using receipt of quality antenatal care (ANC), skilled birth attendance, and quality postnatal care (qPNC), with ANC and PNC measured as composite…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
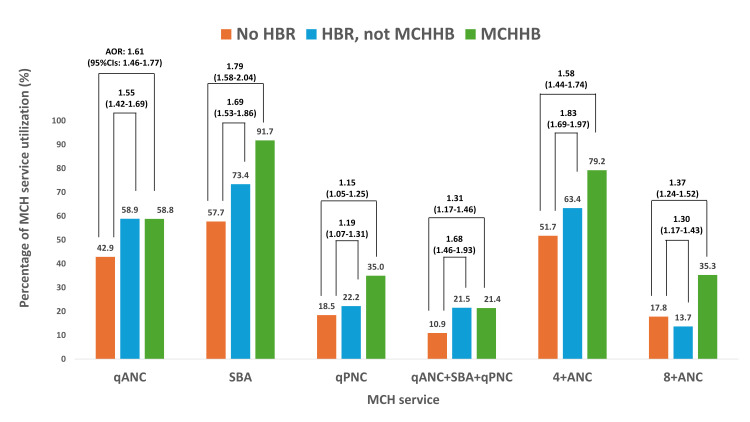 Figure 1
Figure 1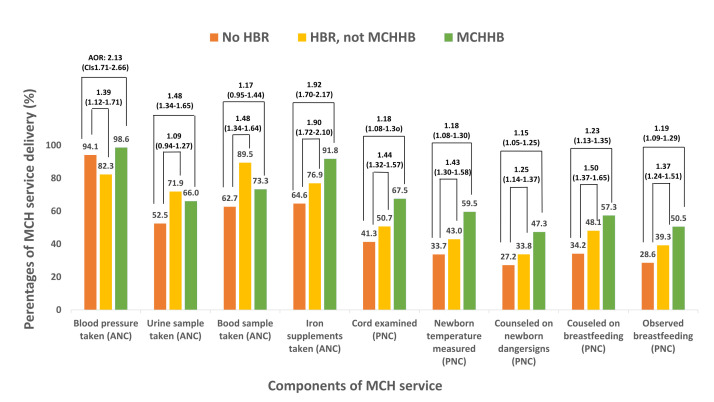 Figure 2
Figure 2| Description | |
|---|---|
|
| Coded as 1 if all five qANC components were received; otherwise coded as 0 |
|
| Coded as 1 if attended by any skilled health personnel ( |
|
| Coded as 1 if all five qPNC components were received within two days of delivery; otherwise coded as 0 |
|
| Defined as having qANC = 1 + SBA = 1 + qPNC = 1 |
|
| MCHHB/HBR present: 1 = card seen; MCHHB/HBR absent: 0 = no card or card not seen |
|
| Age in months at time of survey |
|
| Coded as: 1 = urban; 2 = rural |
|
| Coded as: 1 = no education; 2 = incomplete primary; 3 = completed primary; 4 = incomplete secondary; 5 = completed secondary; 6 = higher education |
|
| Coded as: 1 = poorest; 2 = poorer; 3 = middle; 4 = richer; 5 = richest |
| n (weighted %) | |
|---|---|
|
|
|
| Urban | 33 909 (37.7) |
| Rural | 55 993 (62.3) |
|
|
|
| Burkina Faso | 1995 (2.2) |
| Côte d'Ivoire | 2608 (2.9) |
| Kenya | 4257 (1.7) |
| Senegal | 1550 (4.7) |
| Indonesia | 14 444 (16.1) |
| Timor-Leste | 89 (0.1) |
| Ethiopia | 9684 (10.8) |
| Gambia | 215 (0.2) |
| Guinea | 1585 (1.8) |
| Liberia | 437 (0.5) |
| Mali | 2504 (2.8) |
| Mauritania | 433 (0.5) |
| Maldives | 22 (0.0) |
| Nigeria | 19 975 (22.2) |
| Pakistan | 18 538 (20.6) |
| Tanzania | 6332 (7.0) |
| South Africa | 3870 (4.3) |
| Zimbabwe | 1363 (1.5) |
|
|
|
| Male | 45 750 (50.9) |
| Female | 44 153 (49.1) |
|
|
|
| Poorest | 19 238 (21.4) |
| Poorer | 18 665 (20.8) |
| Middle | 18 212 (20.3) |
| Richer | 17 381 (19.3) |
| Richest | 16 407 (18.2) |
|
|
|
| No education | 31 543 (35.1) |
| Incomplete primary | 8934 (9.9) |
| Complete primary | 11 856 (13.2) |
| Incomplete secondary | 14 900 (16.6) |
| Complete secondary | 13 855 (15.4) |
| Higher | 8815 (9.8) |
| MCHHB | HBR, not MCHHB | No HBR | |
|---|---|---|---|
|
| 16 766 (18.6) | 37 958 (42.2) | 35 178 (39.1) |
|
| 1730 (86.7) |
| 265 (13.3) |
|
| 2049 (78.6) |
| 559 (21.4) |
|
| 3213 (75.5) |
| 1044 (24.5) |
|
| 1271 (82.0) |
| 279 (18.0) |
|
| 8457 (58.5) |
| 5988 (41.5) |
|
| 46 (51.9) |
| 43 (48.1) |
|
|
| 6838 (70.6) | 2846 (29.4) |
|
|
| 194 (90.1) | 21 (9.9) |
|
|
| 1041 (65.6) | 545 (34.4) |
|
|
| 280 (64.0) | 157 (36.0) |
|
|
| 1458 (58.2) | 1046 (41.8) |
|
|
| 197 (45.4) | 237 (54.6) |
|
|
| 18 (81.8) | 4 (18.2) |
|
|
| 8153 (40.8) | 11 822 (59.2) |
|
|
| 11 069 (59.7) | 7469 (40.3) |
|
|
| 4962 (78.4) | 1370 (21.6) |
|
|
| 2691 (69.5) | 1179 (30.5) |
|
| 1058 (77.6) | 305 (22.4) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Maternal and Child Health · Child Nutrition and Water Access · Food Security and Health in Diverse Populations
The continuum of maternal and child health (MCH) care is essential for the survival, health, and development of mothers and children, especially in low- and middle-income countries (LMICs), which face inadequate coverage of essential MCH services despite global efforts [1]. In 2022, the proportion of women receiving at least four antenatal care (ANC) visits with any provider was 55% in Eastern and Southern Africa and South Asia, highlighting the need to improve service utilisation [2,3].
However, the quality of care delivered during each contact is as critical as the number of visits [4,5]. Dandona and colleagues highlighted a notable discrepancy between the reported coverage of ANC and the quality-adjusted ANC visits that provide essential components [6]. Many women do not receive the recommended components of ANC, including routine assessments, interventions, and counselling [7–10]. Therefore, improving maternal and neonatal outcomes requires a high-quality continuum of care and consistent delivery of appropriate interventions across the antenatal, intrapartum, and postnatal periods.
One strategy to strengthen the continuity and quality of MCH care is the use of home-based records (HBRs) [11,12]. Introduced in the mid-1800s as a vaccination card [13], HBRs have evolved into comprehensive tools. The Maternal and Child Health Handbook (MCHHB) is an integrated HBR covering the continuum of care from pregnancy to a child’s fifth year. The MCHHB documents health service use and outcomes, provides educational information for families, and facilitates provider-client communication. It supports maternal education through provider-led counselling and self-directed learning on safe pregnancy, delivery, newborn care, and child development.
To date, over 50 countries and regions, primarily LMICs, have adopted the MCHHB [14], aligning with global health priorities such as the Sustainable Development Goals and World Health Organization (WHO) recommendations [14,15]. The integrated MCHHB was introduced in LMICs in the early 2000s through pilot programmes in Indonesia and Palestine, followed by gradual scale-up in Asia, Africa, and the Pacific during the 2010s. However, empirical evidence regarding the association between HBR ownership and the continuum of quality MCH care remains limited, and few studies have compared the effects of different types of HBRs [16]. Kitabayashi and colleagues reported that MCHHB users in Palestine had significantly higher odds of receiving quality ANC (qANC); however, their study was limited to ANC and a single-country setting [17]. Another study in rural Indonesia found that the MCHHB had positive effects on service uptake and home care practices (e.g. tetanus vaccination, four or more ANC visits, skilled birth attendance (SBA), Vitamin A supplementation, and exclusive breastfeeding), but did not assess the ANC or PNC quality components [18]. Therefore, we aim to examine the association between HBR ownership and the completion of a continuum of quality MCH care and compare outcomes between users of the MCHHB and of other HBR types, using pooled data from multiple LMICs collected in Demographic and Health Surveys (DHS) conducted from 2015 onward, when standardised quality-of-care indicators became available.
METHODS
Study design and data source
We employed a cross-sectional design using pooled data from the most DHS conducted in 18 countries: Burkina Faso (2021), Côte d'Ivoire (2021), Kenya (2022), Senegal (2019), Indonesia (2017), Timor-Leste (2015), Ethiopia (2019), Gambia (2019–2020), Guinea (2018), Liberia (2019–2020), Mali (2018), Mauritania (2019–2021), Maldives (2016–2017), Nigeria (2018), Pakistan (2017–2018), Tanzania (2022), South Africa (2016), and Zimbabwe (2015). We included all data from 2015 onward (Phase 7 and later), when the core questionnaires incorporated more standardised and comparable quality-of-care indicators for MCH across countries, and when standardised data sets containing MCH data were available [19,20].
The DHS is a nationally representative household survey collecting standardised data on MCH, including service coverage, utilisation, and care content. To examine the relationship between HBR ownership and the continuum of quality MCH care, we included countries regardless of whether they introduced the integrated MCHHB.
The DHS surveys follow a standardised sampling, questionnaire design, data collection, and coding methodology, enabling valid cross-country analyses. To ensure national representativeness, DHS employs stratified two-stage sampling: selecting enumeration areas based on each country’s sampling frame and then drawing a sample of households from each [21].
For this analysis, we used the Individual Recode file, which contains data collected from women aged 15–49 years.
Study population
Women and their youngest children (aged 0–35 months) who were eligible for the DHS ‘Has health card’ question were included, yielding 89 902 observations across countries: Burkina Faso (n/N = 1995/5637), Côte d'Ivoire (n/N = 2608/7630), Ethiopia (n/N = 9684/30 465), Gambia (n/N = 215/628), Guinea (n/N = 1585/4278), Indonesia (n/N = 14 444/5960), Kenya (n/N = 4257/14 752), Liberia (n/N = 437/1296), Mali (n/N = 2504/5075), Mauritania (n/N = 433/1296), Maldives (n/N = 22/114), Nigeria (n/N = 19 975/50 768), Pakistan (n/N = 18 538/47 186), Senegal (n/N = 1550/4275), Timor-Leste (n/N = 89/306), Tanzania (n/N = 6332/16 831), South Africa (n/N = 3870/17 272), and Zimbabwe (n/N = 1363/3992). Finally, we excluded 20 samples with missing essential MCH service data and included 36 samples with missing age data.
Variables
Dependent variables
The main outcome variable was the completion of the continuum of quality MCH maternal care, defined as combined receipt of qANC, SBA, and quality postnatal care (qPNC).
We defined qANC as receiving a blood pressure measurement, taking a urine sample, taking a blood sample, and receiving or purchasing iron tablets/syrup during pregnancy. Additionally, SBA was defined as delivery assisted by an obstetrician, doctor, general practitioner, midwife, nurse, certified birth attendant, or health officer. Finally, qPNC was defined as receiving umbilical cord examination, newborn temperature measurement, counselling on newborn danger signs, and counselling on and observation of breastfeeding within the first two days after delivery.
In addition, the analysis included individual outcomes for the number of ANC visits, qANC, SBA, and qPNC.
Independent variables
We used the DHS variable ‘Has health card’ as a proxy for HBR ownership. In countries where the MCHHB has been introduced [22], this card referred to the MCHHB. In other settings, it represented alternative HBR types (Table 1).
Statistical analysis
We merged the DHS data sets for pooled analysis. We conducted a logistic regression analysis to assess associations between HBR ownership and completion of the continuum of quality MCH care and estimated unadjusted and adjusted models. We also conducted subgroup analyses using separate logistic regression models for each MCH service component. Because these analyses were component-specific, we did not include interaction terms. The multivariable logistic regression controlled for known predictors of MCH service use: residence type, maternal education, and the household wealth index [23], and we included the county as a control variable. A multilevel model was unnecessary because ‘Has health card’ was only asked for the last-born child. For missing data, we conducted a complete-case analysis and used no imputation. We only included cases with complete data for qANC, qPNC, and qANC + SBA + qPNC. We reported the results as odds ratios (ORs) and adjusted ORs (aORs) with 95% confidence intervals (CIs).
We used IBM SPSS Statistics, version 29.0 (IBM Corp, Chicago, Illinois, USA) for all analyses. We used the complex samples package to consider the multistate sampling design, incorporating sample weights, primary sampling units, and strata [21]. We also applied country-level weights.
RESULTS
Participant characteristics
The analysis included 89 902 women and their youngest children. Among them, 37.7% of the women resided in urban areas, 21.4% were in the poorest quintile, and 35.1% had no formal education (Table 2).
HBR ownership by country
Among participants, 18.6% owned an MCHHB, 42.2% owned another HBR type, and 39.1% reported having no HBR. Ownership rates varied considerably in countries where the MCHHB is distributed nationally. Notably, the MCHHB ownership was relatively low in Indonesia (58.5%) and Timor-Leste (51.9%).
Among countries that have not yet implemented the MCHHB, the proportion of women owning any HBR type varied widely, from 90.1% in the Gambia to 40.8% in Nigeria (Table 3).
Service utilisation by HBR ownership
Among women who achieved qANC, 42.9% had no HBR, 58.9% owned an HBR other than an MCHHB, and 58.8% owned an MCHHB (Figure 1). Among those without HBR, 57.7% received SBA and 18.5% qPNC. On the other hand, among those with HBR other than MCHHB, 73.4% received SBA and 22.2% qPNC, and among those with MCHHB, 91.7% received SBA and 35.0% qPNC.
MCH service utilisation by types of HBRs and the association between HBR ownership and MCH service utilisation. AOR – adjusted odds ratio, CI – confidence interval, HBR – home-based record, MCH – maternal and child health, MCHHB – maternal and child health handbook, SBA – skilled birth attendance, qANC – quality antenatal care, qPNC – quality postnatal care, 4+ANC – at least four antenatal care visits, 8+ANC – at least eight antenatal care visits.
Furthermore, 51.7% of women without an HBR attended at least four ANC visits, compared with 64.3% of those with HBR and 79.2% of those with an MCHHB.
HBR ownership and MCH service utilisation
Women with MCHHB (OR = 1.90; 95% CI = 1.75–2.06) or another type of HBR (OR = 1.91; 95% CI = 1.76–2.06) were significantly more likely to achieve qANC compared with women without an HBR (Figure 1; Table S1 in the Online Supplementary Document). Likewise, women with MCHHB (OR = 8.14; 95% CI = 7.27–9.12) or another HBR (OR = 2.02; 95% CI = 1.85–2.20) were more likely to deliver with an SBA. Additionally, women with MCHHB (OR = 2.38; 95% CI = 2.18–2.59) or another HBR (OR = 1.26; 95% CI = 1.16–1.37) were more likely to receive qPNC.
Women who owned an MCHHB (OR = 2.22; 95% CI = 2.01–2.44) or another HBR (OR = 2.23; 95% CI = 2.00–2.49) were more likely to consistently utilise qANC, SBA, and qPNC. In terms of ANC visit frequency, MCHHB owners had significantly higher odds of attending at least four visits (OR = 3.56; 95% CI = 3.28–3.87) and more than eight visits (OR = 2.52; 95% CI = 2.31–2.75). Women with HBR were more likely to attend four visits (OR = 1.61; 95% CI = 1.50–1.74) but less likely to attend more than eight (OR = 0.73; 95% CI = 0.66–0.81).
The adjusted multivariable logistic regression showed similar trends. Women with an MCHHB (aOR = 1.61; 95% CI = 1.46–1.77) and another HBR (aOR = 1.55; 95% CI = 1.42–1.69) were significantly more likely to achieve qANC. Also, those with MCHHB (aOR = 1.79; 95% CI = 1.58–2.03) and another HBR (aOR = 1.69; 95% CI = 1.53–1.86) were more likely to utilise SBA. Additionally, women with an MCHHB (aOR = 1.15; 95% CI = 1.05–1.25) or other HBRs (aOR = 1.19; 95% CI = 1.07–1.31) had modestly increased odds of service use.
Association between MCHHB and other HBR types and MCH service utilisation
We conducted logistic regressions, including multivariable models, to assess differences in the associations between MCHHB and other HBR types and MCH service utilisation. We adjusted these models for type of residence, wealth index, women’s educational attainment, and country (Table S2 in the Online Supplementary Document).
Compared to those owning other HBR types, women who owned an MCHHB were significantly more likely to deliver with an SBA (OR = 4.03; 95% CI = 3.57–4.56), have higher qPNC (OR = 1.88; 95% CI = 1.73–2.05), attend at least four ANC visits (OR = 2.21; 95% CI = 2.02–2.41), and attend more than eight ANC visits (OR = 3.44; 95% CI = 3.08–3.85).
However, no significant differences were observed between the two groups in achieving qANC or continuous utilisation of qANC, SBA, and qPNC. Furthermore, after adjusting for residence type, wealth index, women’s educational attainment and country, the associations were no longer significant.
Association between HBR ownership and MCH service components
Compared to those without an HBR, women with MCHHB were more likely to receive blood pressure measurement (OR = 4.39; 95% CI = 3.60–5.35), urine testing (OR = 1.76; 95% CI = 1.62–1.91), blood testing (OR = 1.63; 95% CI = 1.50–1.78), and iron supplementation (OR = 6.11; 95% CI = 5.49–6.82) during ANCs. Women with other HBR types had lower odds of blood pressure measurement (OR = 0.29; 95% CI = 0.25–0.34) but higher odds of urine testing (OR = 2.32; 95% CI = 2.03–2.65), blood testing (OR = 5.05; 95% CI = 4.36–5.84), and iron supplementation (OR = 1.83; 95% CI = 1.67–2.00).
For PNC, women who owned MCHHB were more likely to receive cord examination (OR = 2.95; 95% CI = 2.70–3.23), newborn temperature measurement (OR = 2.89; 95% CI = 2.65–3.15), counselling on newborn danger signs (OR = 2.40; 95% CI = 2.21–2.61), counselling on breastfeeding (OR = 2.59; 95% CI = 2.38–2.81), and observed breastfeeding (OR = 2.55; 95% CI = 2.35–2.77). Women with other HBRs also had higher odds of these PNC services, although the estimates were generally smaller.
The adjusted analyses showed similar patterns. Compared to those without HBR, women with other HBRs were more likely to receive blood pressure measurement (aOR = 1.39; 95% CI = 1.12–1.71) and iron supplementation (aOR = 1.90; 95% CI = 1.72–2.10) (Figure 2; Table S3 in the Online Supplementary Document). However, the associations for urine testing (aOR = 1.09; 95% CI = 0.94–1.27) and blood testing (aOR = 1.17; 95% CI = 0.95–1.44) were not statistically significant.
Association between HBR ownership and each component of MCH service utilisation. ANC – antenatal care, AOR – adjusted odds ratio, CI – confidence interval, HBR – home-based record, MCH – maternal and child health, MCHHB – maternal and child health handbook, PNC – postnatal care.
For PNC, MCHHB ownership continued to be associated with cord examination (aOR = 1.18; 95% CI = 1.08–1.30), newborn temperature measurement (aOR = 1.18; 95% CI = 1.08–1.29), counselling on danger signs (aOR = 1.15; 95% CI = 1.05–1.25), counselling on breastfeeding (aOR = 1.23; 95% CI = 1.13–1.35), and observed breastfeeding (aOR = 1.19; 95% CI = 1.09–1.29). Ownership of other HBRs was also associated with higher adjusted odds of PNC services.
DISCUSSION
We examined associations between owning HBRs and the continuum of quality MCH care, examining differences between owning MCHHB and other HBR types. The findings suggest that mothers with any HBR type, including MCHHB, may receive improved continuous and quality care than those without any HBR. In addition, the MCHHB may facilitate ANC service provision more effectively than other HBRs. Although HBRs are widely adopted, to our knowledge, we are the first to evaluate their association with the continuum of quality MCH care using pooled, nationally representative multi-country DHS data, suggesting that the findings may be broadly relevant across diverse LMIC settings.
We found that women who owned any HBR type, including MCHHB, were more likely to attend at least four and more than eight ANC visits than women without an HBR, aligning with previous studies demonstrating a positive association between HBR ownership and attending at least four ANC visits [18,24], as well as WHO guidelines recognising HBRs as means for promoting continuity of care [16]. However, few studies have examined the association between HBR ownership and attendance of at least eight ANC visits, despite the WHO’s updated recommendation [11]. Our findings contribute to this under-researched area.
Although we found no significant differences between the MCHHB and other HBR types, owning any HBR type was associated with increased utilisation of MCH services, including SBA and PNC. Most studies have investigated associations between HBRs and individual care components, and our results align with those reporting positive associations between HBR ownership and maternal tests and education [17], maternal care [25], and the positive impact of MCHHB on delivery with SBA [18]. Some studies have described associations between HBRs and newborn care, such as immediate breastfeeding [24,26], but few examined HBRs and PNC. Therefore, our finding of a positive association between HBR ownership and postnatal care contributes to the literature.
Women more engaged with health services may be more likely to retain and present HBRs, complicating causal interpretation. Although our cross-sectional design limits causal inference, evidence from countries where the MCHHB was rolled out prior to data collection supports the assumed temporal ordering. Future studies employing longitudinal designs, instrumental-variable methods, or natural experiments are needed to clarify causal relationships.
Although we did not identify significant differences between owning MCHHB and other HBR types regarding continuous care utilisation and quality, we found that mothers who owned MCHHB were more likely to have urine and blood tests than those without HBR, suggesting the importance of owning an HBR that covers ANC. The MCHHB is distinguished by its comprehensive documentation, covering care from pregnancy to five years postpartum and providing detailed information on safe pregnancy, delivery, and child development. It may thus serve as a reminder for healthcare providers. Although many countries have adopted child vaccination cards, HBRs are not always available for ANC. Furthermore, while general HBR ownership may encourage initial visits to health facilities [27], continued engagement depends on women’s understanding of the value of the records and their prior care experiences [23,28].
The MCHHB provides structured guidance to healthcare providers regarding expected care at each ANC contact. Notably, health workers’ knowledge, attitudes, and incentives, along with the facility environment, can also influence care quality. Provider factors, including knowledge, significantly affect ANC quality in MCHHB settings [29]. In some cases, MCHHB is distributed without explanation, reducing its role to mere possession [30]. Qualitative studies exploring provider behaviour, perceptions, and constraints in real-world cases are needed to clarify these dynamics. Further studies, particularly those using qualitative methods, are needed to evaluate how MCHHB is used in practice and how provider-related factors shape its impact.
Following multivariable regression, most univariate associations, consistent with the descriptive statistics, changed direction. These findings suggest that maternal educational attainment and household wealth substantially influence care uptake and MCHHB possession. The MCHHB may require a certain level of literacy and understanding for effective use, although it often includes rich visual content to accommodate varying literacy levels. Therefore, mothers with higher education may derive greater benefit from MCHHBs, whereas vaccination cards may be more accessible to mothers with lower education levels.
Although we included countries where the MCHHB has been officially adopted and distributed nationally, multiple HBR formats coexist. In Côte d’Ivoire, an alternative MCHHB version for Muslim families is available, but it contains fewer informational pages. Additionally, simpler HBR forms are still used. Such variations result in reduced learning opportunities and knowledge gaps, potentially influencing MCH service utilisation.
Moreover, HBRs differ in form, from ANC or vaccination cards to comprehensive ‘mother’s booklets’, with overlapping content. These similarities may overestimate the impact of non-MCHHB HBRs on service use and quality, potentially contributing to the lack of significance in the differences across record types. Future research should consider a more detailed HBR classification to accurately assess their effects.
Finally, our findings suggest that MCHHBs may enhance service delivery by reminding healthcare providers of appropriate care. However, care quality may vary depending on provider-related factors, such as knowledge and motivation. Thus, provider training should be an integral component of MCHHB programmes, alongside qualitative assessments to understand challenges in adopting and delivering quality care. Moreover, the coexistence of multiple HBR formats may hinder effective use and increase provider workload. Countries with such diversity may consider adopting a comprehensive HBR that includes ANC components, as our results indicate improved uptake of urine and blood testing when implemented with a training package.
Limitations
This study has several limitations. First, provider characteristics may influence care quality, but we could not include provider-level factors because we lacked relevant variables. Second, we could not account for differences in HBR form and content, potentially leading to an overestimation of MCHHB and HBR ownership. Moreover, variations in content, format, and programmatic implementation across countries and survey years, as well as temporal changes, may limit the comparability of the ‘card seen’ measure. Such heterogeneity should be considered when interpreting pooled estimates. Third, we excluded some important components due to missing data in specific data sets, such as tetanus vaccination, which was excluded from the qANC indicator in all countries because it was unavailable in Indonesia and Timor-Leste. Additionally, recall bias may have influenced the data, and differences in interview timing may have affected card availability, as mothers reported events that occurred up to three years before data collection. We assessed this potential bias by restricting the analysis to mothers and children whose deliveries or births occurred within two months of data collection; the direction and magnitude of the results did not differ from the main analysis (data not shown). Furthermore, we focused on MCHHB/HBR possession for the most recent birth. When restricted to mothers who owned an MCHHB or other HBR for their firstborn child, the results were consistent with those of the main analysis (data not shown). Finally, because the DHS is cross-sectional, we could not establish causal relationships, and reverse causality remains a possibility.
CONCLUSIONS
We found that mothers who possessed any type of HBR were more likely to consistently utilise quality MCH services. Meanwhile, there were no significant differences between HBR type and the continuity of quality MCH care for MCHHBs, but MCHHB ownership was significantly associated with improved uptake of urine and blood tests.
Although MCHHB may enhance maternal understanding of ANC and assist providers in delivering appropriate care, our analysis was limited to HBR ownership and did not capture how the records were used. Furthermore, we did not consider provider-level factors or variations in content and format, highlighting the need for further research to examine the impact of HBR functionality and use across diverse settings.
Additional material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kerber K Jde Graft-Johnson JE Bhutta ZA Okong P Starrs A Lawn JE Continuum of care for maternal, newborn, and child health: from slogan to service delivery. Lancet. 2007;370:1358–69. 10.1016/S 0140-6736(07)61578-517933651 · doi ↗ · pubmed ↗
- 2United Nations Children’s Fund. Antenatal care. 2024. Available: https://data.unicef.org/topic/maternal-health/antenatal-care/. Accessed: 14 April 2025.
- 3United Nations Children’s Fund. Delivery care. 2024. Available: https://data.unicef.org/topic/maternal-health/delivery-care/. Accessed: 14 April 2025.
- 4World Health Organization. Reproductive, maternal, newborn and child health and human rights: a toolbox for examining laws, regulations and policies. Geneva, Switzerland: World Health Organization; 2014. Available: https://iris.who.int/bitstream/handle/10665/126383/9789241507424_eng.pdf;jsessionid=3BD 0837 A 51E 02B 6B 2A 62FF 32F 57D 57A 4?sequence=1. Accessed: 4 April 2025.
- 5World Health Organization. Maternal mortality. Geneva, Switzerland: World Health Organization; 2014. Available: https://iris.who.int/server/api/core/bitstreams/397dce 55-94cb-490c-bd 58-8ac 27d 8e 7aa 5/content. Accessed: 4 April 2025.
- 6Dandona R Kumar GA Majumder M Akbar M Prasad Dora SS Dandona L Poor coverage of quality-adjusted antenatal care services: a population-level assessment by visit and source of antenatal care services in Bihar state of India. Lancet Reg Health Southeast Asia. 2023;25:100332. 10.1016/j.lansea.2023.10033239021484 PMC 467073 · doi ↗ · pubmed ↗
- 7Benova L TunçalpÖMoran AC Campbell OMR Not just a number: examining coverage and content of antenatal care in low-income and middle-income countries. BMJ Glob Health. 2018;3:e 000779. 10.1136/bmjgh-2018-00077929662698 PMC 5898334 · doi ↗ · pubmed ↗
- 8Arroyave L Saad GE Victora CG Barros AJDA new content-qualified antenatal care coverage indicator: development and validation of a score using national health surveys in low- and middle-income countries. J Glob Health. 2021;11:04008. 10.7189/jogh.11.0400833692892 PMC 7916319 · doi ↗ · pubmed ↗