Teleultrasound in obstetrics: A systematic review and meta-analysis
Jack Le Vance, Matthew Vaughan, Tanvi Bhatia, Leo Gurney, Victoria Hodgetts Morton, R. Katie Morris, Alexandra Tosun, Alexandra Tosun, Alexandra Tosun, Alexandra Tosun

TL;DR
This study reviews the use of teleultrasound in pregnancy care, finding it feasible, accurate, and acceptable, especially for high-risk patients and in rural areas.
Contribution
The paper provides the first comprehensive systematic review and meta-analysis on the feasibility, accuracy, and cost-effectiveness of teleultrasound in obstetrics.
Findings
Teleultrasound is non-inferior to conventional ultrasound for identifying fetal structures in most cases.
Patient-operated and novice-led teleultrasound show promise for improving access in low-resource settings.
Diagnostic accuracy is high, with an AUC of 0.93, though specialized anatomy visualization remains challenging.
Abstract
Ultrasound is a common diagnostic modality in obstetrics to evaluate the fetal condition, frequently used in pregnant women classifying as high-risk. Modifications to guidelines, implementation of national initiatives, combined with an aging obstetric population has led to an increased number of high-risk patients. This places a substantial strain on outpatient obstetric services to accommodate the increased demand for serial antenatal ultrasound scans. Recent advancements in digital technology have enabled the swift innovation of teleultrasound development. The recent pandemic has also substantially influenced technological development, as obstetric services considered alternative solutions to healthcare provision standards. This review aims to assess whether teleultrasound is feasible, acceptable, diagnostically accurate, and cost-effective for antenatal care. We searched MEDLINE,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
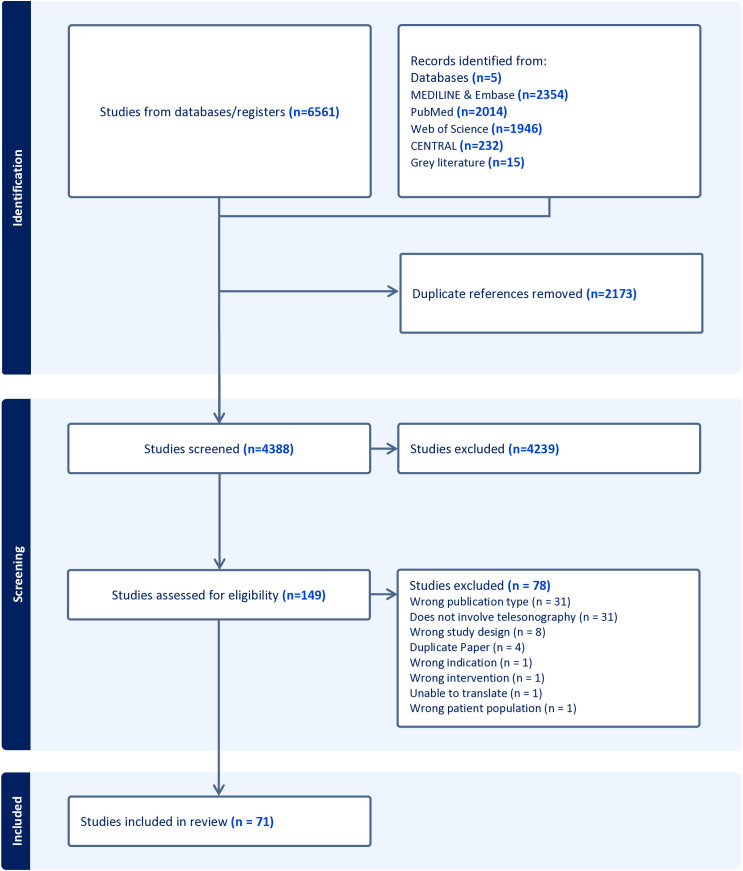 Fig 1
Fig 1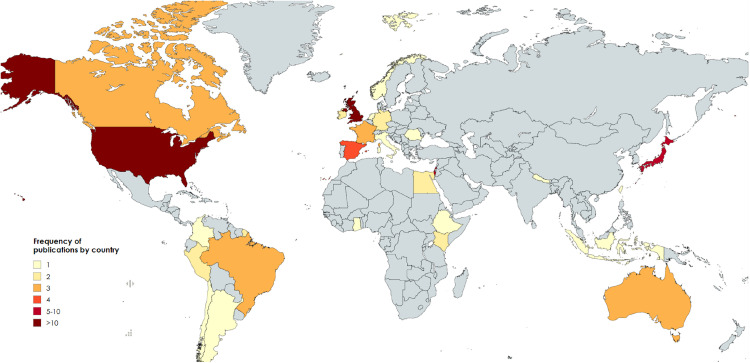 Fig 2
Fig 2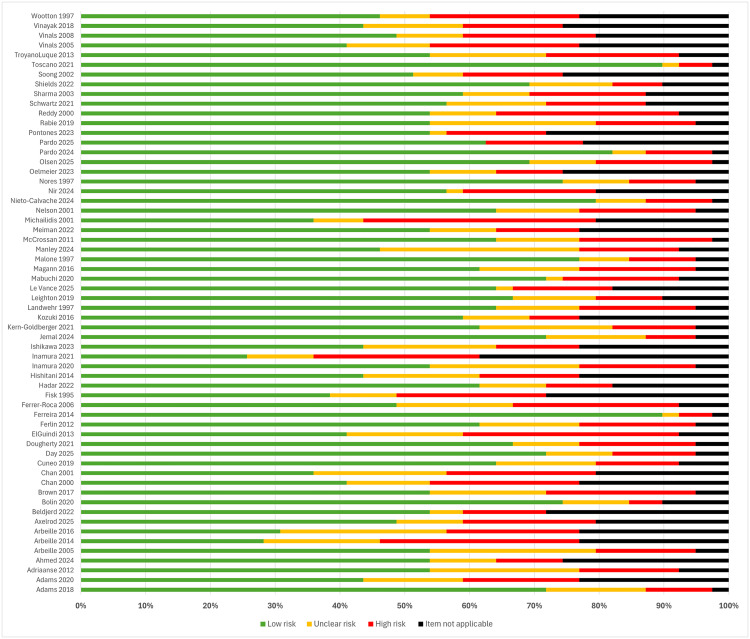 Fig 3
Fig 3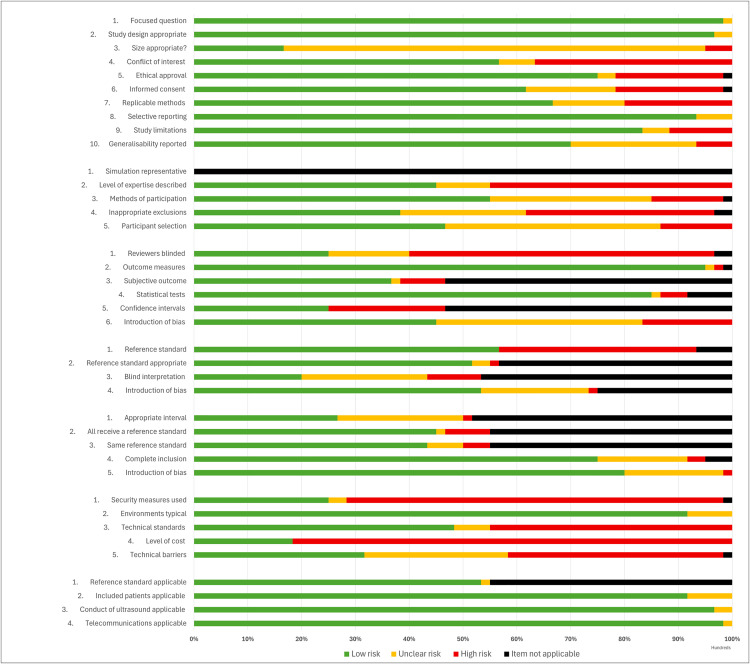 Fig 4
Fig 4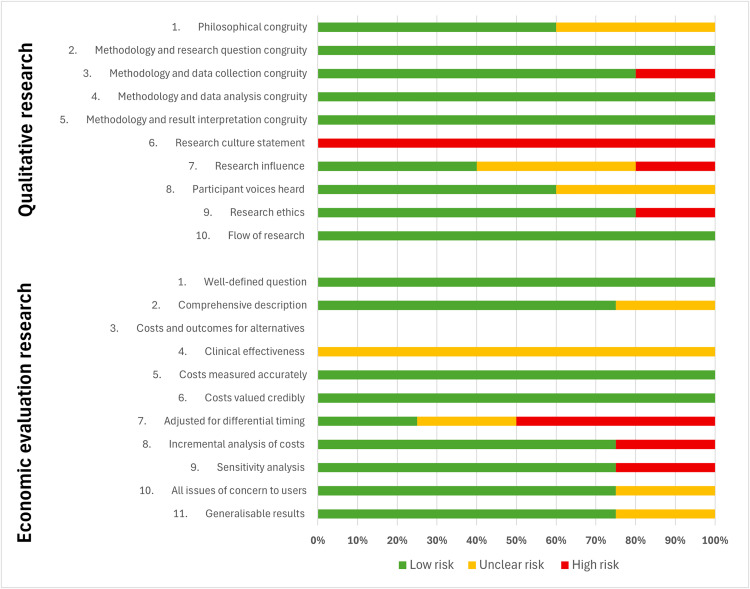 Fig 5
Fig 5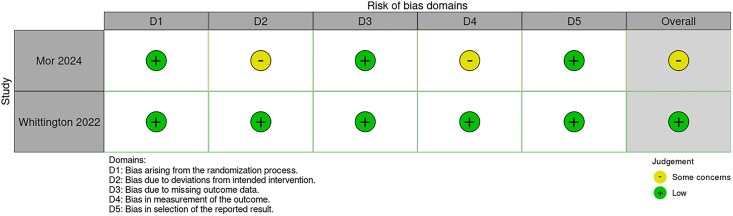 Fig 6
Fig 6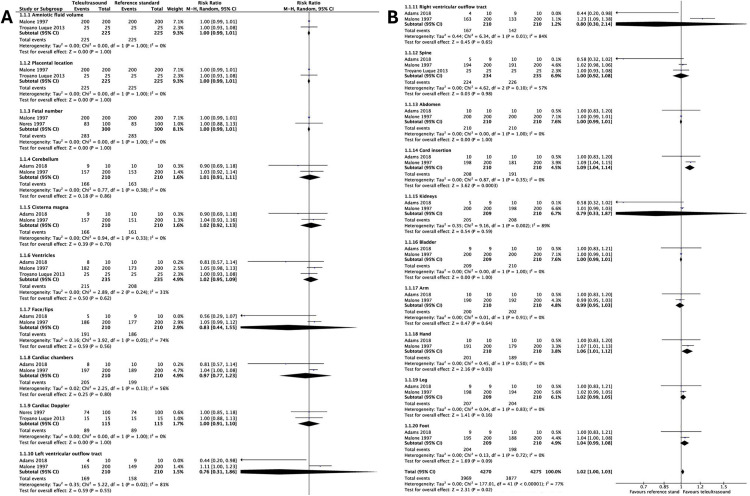 Fig 7
Fig 7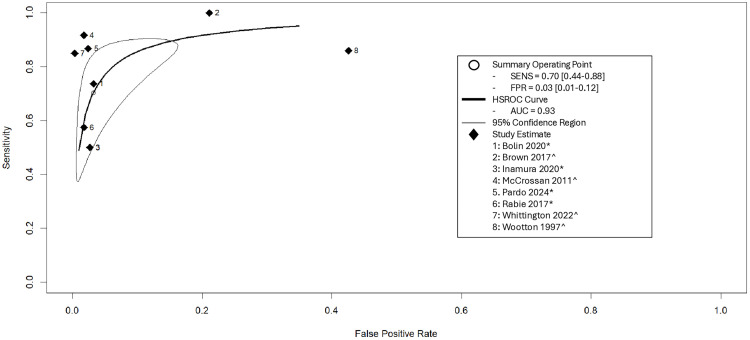 Fig 8
Fig 8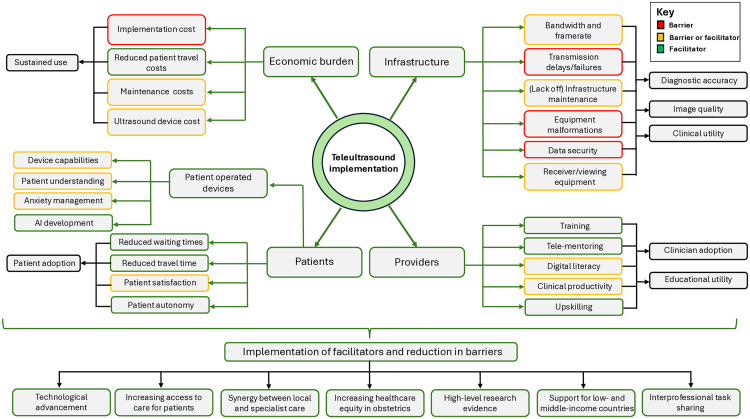 Fig 9
Fig 9Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUltrasound in Clinical Applications · Ultrasound Imaging and Elastography · Phonocardiography and Auscultation Techniques
Introduction
Ultrasound is a commonly used diagnostic modality in obstetrics to evaluate the fetal condition, which is frequently used in pregnant women who are classified as high-risk. Following recent guideline changes combined with an aging obstetric population, a greater proportion of women are now classified as high-risk, placing a strain on current obstetric services to accommodate the increased demand for ultrasound examination [1]. Advancements in digital medical technology combined with the increased access to smartphones, virtual video communication, and wireless internet have enabled the swift innovation of teleultrasound development [2,3]. The recent pandemic has also had a substantial influence on technological development, as obstetric services now need to consider alternative solutions to current healthcare provision standards.
Teleultrasound/tele-sonography and remote portable ultrasound devices combine the usage of ultrasound with telecommunication to enable remote examination either in synchronous or asynchronous format. Synchronous communication involves real-time feedback commonly conducted between a non-expert sonographer and an imaging expert [4]. Ultrasound examination with delayed transmission for expert review demonstrates asynchronous communication [5]. Obstetric teleultrasound represents potential advantages with improved patient autonomy, education, reduced hospital attendance, and economic burden [3,6,7]. Importantly, teleultrasound presents opportunities to improve overall access to ultrasound services and aims to address current health outcome disparities, particularly seen within low- and middle-income countries [6,8].
Teleultrasound usage in other healthcare settings, such as emergency medicine has been clearly demonstrated [4]. Despite the rapid developments of digital teleultrasound innovations in obstetrics, the collation of available evidence is minimal and requires thorough exploration. This review aims to assess whether teleultrasound is feasible, acceptable, diagnostically accurate, and cost-effective for the assessment of obstetric patients.
Methodology
Study registration
This systematic review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines (S1 Table) [9,10]. A protocol for this review was registered with PROSPERO (CRD42024615570).
Inclusion and exclusion criteria
Complete inclusion and exclusion criteria can be seen within Table 1. Principally, all primary research studies regarding antenatal teleultrasound usage within obstetrics were included. Included studies assessed teleultrasound services, remote patient- or clinician-operated ultrasound devices. However, studies using remote ultrasound devices were only included if the study detailed an additional telemedicine review for the completed ultrasound images/recordings. Synchronous and/or asynchronous telemedicine transmission occurring between hospitals, between pre-hospital sectors and the hospital, or between the home and hospital were included. Clinical outcomes related to feasibility, diagnostic accuracy, clinical and educational utility, qualitative and economic outcomes were eligible for inclusion. Conference abstracts, communication papers, editorials, systematic reviews, narrative reviews, and single case reports. were excluded. Studies referring to overall telemedicine models, however, not specifying teleultrasound usage were excluded.
Table 1: Inclusion and exclusion criteria.
Search strategy, study selection, and data extraction
MEDLINE, Embase, Cochrane Database of Clinical Trials (CENTRAL), Web of Science, and PubMed databases were searched from inception to 31st December 2025. Search terms and functions were appropriately adapted for each database with medical subject headings and text words were used. The research strategy for MEDLINE and Embase can be seen in S2 Table. Reference lists of primary studies and reviews were additionally screened to identify gray literature citations eligible for inclusion. No language restrictions were applied. Covidence software (Veritas Health Innovation M, Australia) was used to manage title, abstract, and full manuscript screening. This process was repeated for the subsequent data extraction. All titles, abstracts, and full texts were reviewed independently by two out of three available researchers (JLV, MV, TB). Any conflicts were discussed with a fourth independent author (LG). For eligible studies, data was extracted into a pre-designed electronic spreadsheet. Data extracted from each study included the author, year of publication, study location, patient demographics, sample size, indication of teleultrasound usage, gestational age of usage, type of technology used, teleultrasound technical details, teleultrasound method (synchronous or asynchronous), teleultrasound performer, teleultrasound examiner, and additional study-specific outcomes. Data extraction was performed by two out of three available independent researchers (JLV, MV, TB). Any discrepancies were resolved by consensus.
Risk of bias and trustworthiness
For observational studies, the methodological quality of these studies was assessed using an adapted form of the QUADAS-2 checklist from Whiting and colleagues and Marsh-Feiley and colleagues [4,11] (S3 Table). Seven domains, adapted for obstetric studies, were assessed to determine bias: 1) Generic quality standards; 2) Participant selection bias; 3) Index test; 4) Reference standard; 5) Flow and timing; 6) Telemedicine/technology-specific items; 7) Overall applicability. Risk of bias for qualitative and economic evaluation studies was performed using the critical appraisal checklists from the Joanna Briggs Institute (JBI) [12,13]. The Cochrane risk of bias tool (RoB2) was used to assess bias in randomized interventional studies [14]. Risk of bias were independently assessed by two out of three available reviewers (JH, MV, TB). Any discrepancies with bias assessment were arbitrated with a fourth independent author (LG).
Certainty of evidence
The grading of recommendations assessment, development, and evaluation (GRADE) approach was used to assess the certainty of the body of evidence for each applicable outcome evaluated in the findings and presented in tabulated format [15,16].
Data analysis
Single variable proportional data such as the identification rates of fetal/placental structures was calculated using R version 4.5.1 [17]. Random effects models were used to meta-analyze estimates of the overall proportional data and 95% confidence intervals (CIs), due to the high likelihood of statistical heterogeneity. The inverse variance method with logit transformation of the rate was used. Summary proportions and CI were configured with forest plots, including quantitative assessment for heterogeneity using I^2^ [18].
To evaluate the diagnostic accuracy of teleultrasound compared with the reference standard, a hierarchical summary receiver operating characteristic (HSROC) model was employed. This approach allows for the simultaneous estimation of study-level sensitivity and specificity while accounting for between-study heterogeneity and when a range of thresholds are used [19]. All analyses were conducted in using R version 4.5.1 using the mada packages [17,20]. Study-level 2 × 2 contingency data (true positives, false positives, false negatives, and true negatives) were extracted and entered into R to compute individual study estimates of sensitivity and specificity with corresponding 95% CIs. The Reitsma bivariate random-effects model, a function from the mada package was used to fit a bivariate random-effects model to the diagnostic accuracy data to derive pooled estimates of sensitivity and specificity, along with the summary receiver operating characteristic (SROC) curve and the area under the curve (AUC) [21].
Review Manager 5.4 (RevMan) was pragmatically used to meta-analyze pairwise data, such as identification rates of fetal/placental structures in teleultrasound versus the denoted reference standard [22]. Inclusion of two of more studies with identical clinical outcomes were eligible for meta-analysis. Dichotomous outcome data were assessed with 2 × 2 tables constructed to calculate risk ratios (RRs) and 95% CI. Mantel–Haenszel method random-effects models were utilized for meta-analysis. Summary RR were presented using forest plots, allowing visual inspection and quantitative assessment for heterogeneity using I^2^. Zero-cell adjustments to 0.5 were used as required. Meta-analysis of clinical and technological outcome data was not possible due to inconsistent outcome reporting and wide methodological variance in included studies. Therefore, a descriptive synthesis of data alongside available meta-analyzable data is therefore provided. Standardized metrics provided by included studies, such as p values, have also been integrated into the results and summary tables below. Due to the small number of included studies for each meta-analyzed outcome, subgroup analysis, and publication bias was not examined.
Results
The database and gray literature searches identified 6,561 abstracts. A total of 2,173 duplicate abstracts were removed, leaving 4,388 abstracts for screening. A total of 149 full texts were reviewed, from which 71 papers (60 clinical observational studies, five qualitative studies, four economic evaluation studies, and two randomized controlled trials) recruiting across 27 countries were eligible for inclusion (Fig 1) [23–93]. The most common reason for exclusion during full text screening was due the wrong publication type, whereby the acquired full text frequently referred to a published conference abstract without a full manuscript available. Excluded studies following full-text screening are presented in S4 Table.
PRISMA flow diagram.CENTRAL, Cochrane Database of Clinical Trials.
Study characteristics
All articles were published between 1995 and 2025, with the majority occurring between 2020 and 2025. Recruitment from low/middle income countries represented 14% of the total included studies [40,41,50,52,79,81,84–86,90]. One study recruited in each of: Argentina, Chile, Colombia, Ethiopia, Ghana, Indonesia, Italy, the Netherlands, Nepal, Norway, Romania, and Taiwan. Two studies recruited in each of: Egypt, French Guiana, Germany, Ireland, Kenya, and Peru. Three studies recruited in each of: Australia, Brazil, Canada, and France. Four studies recruited in Spain, six in Japan and Israel, 13 in the United Kingdom (UK), and 22 in the United States of America (USA). Four studies recruited participants in more than one country, ranging from two to 12 [26,83,86,90]. A graphical representation of study recruitment can be seen in Fig 2.
World map graphical representation of included studies recruitment origin.Produced with permission from https://www.mapchart.net/world.html.
Risk of bias
Risk of bias assessments for all included articles are presented in S5 Table. Summary results for each of the 60 observational studies, including pooled results stratified by the individual risk of bias domain using the modified QUADAS-2 checklist are presented in Figs 3 and 4. The overall quality of the articles was generally poor, with high risk of bias. This was primarily attributed to the suboptimal quality of methodological reporting regarding participant inclusion/exclusion criteria and detailed technical descriptors/standards of the teleultrasound modality used. Many studies lacked a reference group or comparison, leading to insufficient detail to enable study replication. Most commonly, observational studies failed to provide information regarding security measures and cost implications. When provided, details were frequently limited to brief statements such as encrypted/personal communication networks [33,41,45,47–49,55,84], de-identified image transfer [29,62,90], and secure teleultrasound technology [44,54]. Observational studies presenting cost outcomes ranged from detailed economic evaluations [29,54] to crude cost estimations [35,36,85], but most commonly demonstrated only short, brief statements regarding teleultrasound costings [40,45,60,75,77,86].
Summary risk of bias results for clinical observational studies using the QUADAS-2 checklist.
Risk of bias results for clinical observational studies using the QUADAS-2 checklist, stratified by each domain.
Economic evaluation and qualitative studies were generally of lower bias risk across all categories assessed within the JBI frameworks. The two randomized interventional studies generally demonstrated low bias risk across all domains of the Cochrane RoB2 tool; however, aspects of bias concerns were raised within one study over deviations from the intended intervention and the outcomes measured (Figs 5 and 6) [65].
Risk of bias results for qualitative and economic evaluating studies using the JBI frameworks, stratified by each domain.
Risk of bias results for randomized controlled trials using the Cochrane RoB2 tool, stratified by each domain.
Study design and methodology
Included studies were highly heterogenous in design, methodology and the outcomes measured. Study sample sizes ranged from 2 to 106,674 participants; however, 67% of studies included 100 participants or fewer. Ten% of studies incorporated tele-transmission of transvaginal ultrasound scans, whilst the remaining solely used transabdominal ultrasound scans [68,75,78,79,83,90]. Isolating results specifically for tele-transvaginal scans was not possible. Gestational age at which teleultrasound occurred was widely dispersed in the studies. Four studies assessed in the first trimester [40,68,78,79], eight in the second trimester [25,37,41,60,61,86,88,90], six in the third trimester [27,48,67,85,87,89], three in the first and second trimesters [31,65,66], 19 in the second and third trimesters [7,23,32,33,36,49,50,55,62,63,70,71,73,74,76,80,84,91], 12 in all trimesters [24,29,30,42,44,51,53,58,82,83,92,93], and 19 did not disclose [7,26,28,34,35,38,39,43,45,52,54,59,64,69,72,75,77,81]. Sixty studies assessed hospital to hospital teleultrasound transmission, four evaluated pre-hospital/community to hospital transmission [24,50,52,81], and seven studies assessed home to hospital transmission [44,65,85,87,89,92,93].
Observational studies were broadly categorized by the authors (JLV and LG) into two main subtypes. Firstly, feasibility studies considered the capabilities and specifications of different teleultrasound technologies to transmit and receive information that was deemed clinically useful [24,26–28,34,35,39–41,43,45,48,49,51,54,57,63,66–70,72–75,77,80,81,86,87,89,92]. Secondly, diagnostic accuracy studies evaluated the diagnostic capabilities of teleultrasound [23,25,29,32,33,36,37,42,44,47,51,53,55,56,59,60,62,71,78,79,83–85,88,90,91,93].
All studies either incorporated asynchronous [23,25,26,29,30,33,37–39,42,44,47,48,51,52,55,61–63,66,70,75,78–81,83–85,88–90,92] or synchronous teleultrasound transmission [27,28,31,32,34–36,41,43,49,50,53,54,59,60,64,65,67,74,76,77,82,86,87,91]. Several studies incorporated both transmission techniques [24,40,45,46,56–58,68,69,71–73,93]. The vast majority of studies transmitted data via internet, satellite, telephone or ISDN channels, however, three additional earlier studies incorporated physical courier transfer alongside internet transmission [58,66,68]. Internet transmission bandwidths ranged between 64 kilobits per second (Kb/s) to 9.6 gigabits per second (Gb/s) [36,42], however, many studies failed to provide such details. Included studies encompassed various clinical applications including antenatal screening [34,35,38–41,45,46,57,58,63,68,69,74–76,79], antenatal diagnosis [25,29,30,32,33,42,47,48,51,55,56,60–62,64,80,82–84,86,88,90], access to specialist expertise in rural and deprived areas [23,24,26–28,31,36,43,49,53,54,59,66,72,77,85,91], and handheld/point-of-case ultrasound [37,44,50,52,65,67,70,75,81,87,89,92,93]. Several studies acknowledged more than one of these clinical applications. Documented distance between the operator and receiver for teleultrasound transmission, aside from in-hospital transfer ranged vastly from 4 to 8,276 miles [41,73]. Despite the crucial role of compression algorithms in facilitating the packaging and reduction of data volume from an original file format to enable successful teleultrasound, only eight studies detailed such information [40,41,43,57,59,63,84,88]. Detailed description of each study methodology can be found in S6 Table.
Study findings
Feasibility.
Thirty-three studies primarily evaluated feasibility outcomes. The duration of an ultrasound scan ranged from 3.8 min for a basic first-trimester scan to 38.1 min using a tele-operated robotic ultrasound device performing a second-trimester anatomy scan [24,68]. Frequently, if commented on, scans persisted longer than 10 min [28,35,40,57]. Transmission delays and failures were scarcely reported. In synchronous systems, transmission delays were commonly less than 3 s, with little impact on performance [24,28,40]. However, Adams and colleagues demonstrated ultrasound video transmission delays of up to 10 s in 14% of scans, whereby this impacted on performance were noted [24]. Amongst asynchronous systems, transmission delays ranged from 4 to 19 min; usually dependent on the number of image acquisitions acquired [26,27,81,84]. Transmission failure rates ranged from 0%–20%, however, minimal studies commented on this [27,67,68,74,77,86]. Primarily, this was attributed to insufficiencies in technological infrastructure support, equipment malformations, and software corruption.
Image quality was assessed using a variety of measures including binary assessment [26,57,63], Likert scales [41,66,68,74,84], and subjective metrics [24,28,40,43,45,86,89]. When studies compared against the reference standard, image quality of tele-transmitted scans was particularly good, frequently reporting more than 75% of tele-scans having similar quality or rather reporting high image quality agreement through subjective assessment [41,45,57,68,74]. Overall image quality was higher in 2-dimensional versus three-dimensional teleultrasound, primarily due to the loss of resolution on extracted planes from acquired volume data [66].
First- and third-trimester tele-scans frequently demonstrated high visualization scoring for basic anatomical identification, reporting rates ranging between 68%–100% and 81%–100%, respectively [24,26,27,40,44,53,59,67,68,78–80,89,93]. Studies examining second-trimester fetuses adequately identified structures ranging from 18% to 100% [23,24,47,53,57,59,60,63,70,80,88,93]. However, typically second-trimester scans examined a greater number of more specialized anatomical features. Included studies frequently classed an anatomical structure as correctly identified when the acquired images would be comparative to what is normally conducted in routine ultrasound practice. Table 2 represents a condensed tabulated summary of all visualization rates using teleultrasound. These have been stratified by anatomical structure and grouped by body system. A series of proportional meta-analyses demonstrating the identification rates for fetal/placental structures using teleultrasound, provided by included studies can be seen in S1 Fig. Generally, neurological, facial, and cardiac anatomy were frequently visualized at lower rates during routine anatomical teleultrasound surveys versus other structures. Such that the cavum septum pellucidum, nuchal thickness, fetal profile and genitalia were seen in only 33%, 43%, 64% and 80% of teleultrasound scans, respectively (S1 Fig). Fetal breathing was also infrequently identified in one study using patient-operated remote ultrasound at a rate of 24% [44]. Field of view, focal zone range, and gray scale changes following tele-transmission of scans were attributing factors to loss of image quality [40]. Equipment alterations, such as larger video monitors did enable enhanced clinician-reported image quality [43].
Table 2: Rates of identification reported within included studies for each respective anatomical structure.
Meta-analysis of identification rates between teleultrasound and the reference standard were available in four studies for a subset of fetal and placental structures (Fig 7). Only two or three studies were eligible for each meta-analyzed outcome. Teleultrasound was non-inferior in 18 out of the 20 anatomical structures assessed when compared to the reference standard, with an overall pooled effect of RR 1.02 (95% CI [1.00,1.03]). Identification rates of the abdominal cord insertion and the fetal hand were significantly greater in the teleultrasound group RR 1.09 (95% CI [1.04,1.14]) and RR 1.06 (95% CI [1.01,1.12]), respectively. The reference standard in the included studies was not consistent, ranging from conventional in-hospital ultrasound to videotape review. This likely attributed to variations in the point estimates seen and thus should be considered when interpreting these findings.
Meta-analysis of identification rates for fetal and placental structures using teleultrasound vs. the reference standard.(A) Structures 1–10. (B) Structures 11–20, including the overall pooled effect. CI, confidence interval. M-H, Mantel–Haenszel.
The relationship between various bandwidth requirements and image quality was further explored within studies. Very low bandwidths (<284 Kb/s) demonstrated significantly worse (p < 0.01) image quality versus higher bandwidths; however, the most cost-effective rates were 384 Kb/s and 1 megabit per second (Mb/s) [35,74]. Decreasing the frame rate may reduce overall data burden, enabling transmission over lower bandwidths, whilst aiming to not decrease overall image quality and risk transmission failure [57,77]. Bandwidths above 2Mb/s alongside a higher framerate demonstrated ultrasound images which were comparative to original scans, with minimal loss of image quality [40,43,45,50]. However, certain studies still demonstrated constraints with image quality and delayed video lag using advanced telesonography techniques with bandwidths up to 5 Mb/s, such as robotic ultrasound [24,28]. Less recent publications (>20 years old) frequently used bandwidths of 384 Kb/s or less [34,57,68,74,77], whilst more recent studies, with the advent of newer teleultrasound technology all used bandwidths ≥1 Mb/s [24,26,28,40,41,45,50]. Lower bandwidth requirements were more frequently seen in studies with a primary clinical focus on antenatal screening, whilst higher bandwidth requirements were more commonly seen in studies further aiming to improve access to specialist expertise in remote and deprived areas. It was feasible to transmit ultrasound data across a wide range of distances, both asynchronously and synchronously, with many studies transmitting data over 500 kilometers (km) [24,28,34,35,38,41,66,77]. Evidence suggests that healthcare professionals with novice obstetric ultrasound skills are capable of performing basic scans with the aid of long-distance remote tele-supervision [26,28,50,81]. A summary of studies primarily evaluating feasibility outcomes can be seen in Table 3.
Table 3: Summary of studies primarily evaluating feasibility outcomes.
Diagnostic accuracy.
Twenty-seven studies primarily evaluated outcomes in relation to the diagnostic accuracy of teleultrasound. For almost all such studies, accuracy was established by the comparative proportion of correctly classified cases using teleultrasound versus the reference standard. Most studies used either conventional in-hospital ultrasound [23,27,37,42,47,51,53,60,78,79,82–84,88,91,93], intraoperative diagnosis [90] or postnatal diagnosis as the chosen reference standard [25,33,36,55,56,82]. Some studies graded each teleultrasound scan employing a binary classification (normal/abnormal or satisfactory/unsatisfactory) [29,44,52]. However, trinary and quinary classifications were implemented in certain studies, to further refine the diagnostic accuracy of teleultrasound when comparing to the reference standard [25,42,53,79]. A single study, by Rabie and colleagues explicitly defined accuracy as the proportion of correctly identified cases by the sum of the true positives and true negatives [71].
Diagnostic accuracy ranged between 68.7% and 98.6% [82,83], with studies frequently citing above 95% [32,47,55,56,60,82]. One randomized controlled trial of 300 patients, whereby a sonographer performed the scan with synchronous interpretation by a group of five specialists, demonstrated that teleultrasound was non-inferior to conventional ultrasound for assessing congenital anomalies. Diagnostic accuracy was above 97% for both groups, however, details regarding the type of anomalies detected and their respective individualized diagnostic accuracy were not reported [82].
A HSROC model was applied to evaluate the diagnostic accuracy of teleultrasound across available included studies (Fig 8). The pooled diagnostic accuracy across studies demonstrated excellent overall performance, with an AUC of 0.93, indicating strong discriminative ability. The pooled sensitivity was 0.70 (95% CI [0.544,0.88]), and the pooled false positive rate was 0.03 (95% CI [0.01,0.12]). Statistical heterogeneity was moderate, with an I² value of 42.5%. This level of heterogeneity is likely indicated by some variability in study populations and choice of reference standard. Additionally, a proportional meta-analysis of all available accuracy results within included studies can be seen in S2 Fig. Overall, the pooled diagnostic accuracy of obstetric teleultrasound was 93% (95% CI [87%,99%]). A tabulated version including sensitivity, specificity, positive and negative predictive values can be seen in S7 Table.
Hierarchical summary receiver operating characteristic (HSROC) curve for the diagnostic accuracy of teleultrasound with the confidence region around summary operating point.() represents the reference standard was conventional in-hospital ultrasound. (^) represented the reference standard was postnatal diagnosis. AUC, area under the curve; FPR, false positive rate; HSROC, hierarchical summary receiver operating characteristic SENS, sensitivity.*
Among users reviewing obstetric tele-transmitted images/videos, inter-agreement was frequently moderate to excellent, albeit there was wide range; Cohen’s kappa (k) = 0.11–1.00 [37], k = 0.75 [42], k = 0.70–0.98 [44], k = 0.17–0.65 [53], k = 0.59 [56], k = 0.89 [60], k = 0.91 [78], k = 0.40–1.00 [79], k = 0.55–0.78 [84], k = 0.94–1.00 [85], k = 0.63 [90]. Low agreement levels were primarily in relation to discriminate positions of placental locations and identification of more subtle anatomical features such as the fetal kidneys, which frequently rely on optimal image quality for clear identification [37,53]. Intraclass correlations between teleultrasound and conventional ultrasound were noted by three studies, demonstrating poor to excellent agreement 0.711–0.995 [26], 0.28–0.95 [84] and 0.990–0.993 [91]. A summary of studies primarily evaluating diagnostic accuracy outcomes can be seen in Table 4.
Table 4: Summary of studies primarily evaluating diagnostic accuracy outcomes.
Clinical utility.
Maternal-fetal clinical outcomes were not significantly different (p > 0.05) between the teleultrasound group versus the control groups; however, rates of prenatal diagnosis significantly increased following implementation of teleultrasound, ranging from 26% to 159% (p < 0.05) [29,54,62,93]. Regarding system-based findings, teleultrasound shortened the overall clinic visit time, reduced the time taken for patients to be informed of clinical findings, and was associated high ratings of acceptability among service users [54,72,87]. Teleultrasound was noted to decrease patient waiting times for scans and reduced overall patient backlogs, fostering a streamlined obstetric clinic [59]. Chan and colleagues revealed that the implementation of teleultrasound resulted in a modification to the existing clinical diagnosis in 46% of teleultrasound cases, which altered the continued management plan in a third of cases (half of which were minor variations) [34].
Patient-operated telesonography.
Eight studies assessed the usage of patient-operated obstetric teleultrasound [44,65,67,70,87,89,92,93]. Patient-operated ultrasound was a feasible solution for performing a basic assessment of fetal well-being, with high user acceptability. Hadar and colleagues and Le Vance and colleagues demonstrated high acquisitions of the fetal heartbeat (95.3% and 92%), fetal movements (88.3% and 83%), and assessment of normal liquor volume (92.2% and 100%) in 1,360 and 24 self-scans, respectively [44,89]. Pontones and colleagues reported lower identification rates using asynchronous transmission in 46 women, at only 52.2% for the fetal heart rate and amniotic fluid volume, whilst only 14% for fetal profile [70]. Contrastingly, Nir and colleagues incorporated real-time support for 10 patient self-scan sessions, demonstrating appropriate biophysical assessment in 90% of cases, combined with high acceptability ratings [67]. Further comparison between patient independently scanning versus those synchronously guided by clinician demonstrated improved accuracy across several parameters, including the fetal heart rate, measurement of the liquor volume using the latter technique [93]. The use of patient-operated devices has also demonstrated effectiveness for anxiety management for women with recurrent pregnancy loss, as demonstrated in a recently published randomized controlled trial of 50 women [65]. Patient-operated teleultrasound technology is a novel intervention and currently only provides limited assessments of fetal well-being. Further evaluation of home use is necessitated, particularly in patients from ethnic minorities and low education levels, which were underrepresented in current studies [44,65,89]. A summary of studies using patient-operated teleultrasound devices can be seen in Table 5.
Table 5: Summary of studies using patient-operated teleultrasound devices.
Three- and four-dimensional ultrasound.
Three-dimensional obstetric ultrasound via asynchronous tele-transmission was investigated by five studies [26,42,55,63,66]. Primarily, image quality was poor in comparison to two-dimesensional ultrasound, with far longer image pre-processing (up to 4 hours) and transmission times due to large data volumes [42,55,66]. Nevertheless, Mabuchi and colleagues reported a high prenatal diagnostic accuracy (95%) for cases of congenital heart disease in second and third trimester fetuses, whilst Ferrer-Roca and colleagues demonstrated a moderate interclass correlation (Kappa = 0.70) between three-dimensional and conventional image acquisitions within all trimesters [42,55]. This scan modality may play a role in off-line assessment for remote locations whereby access to a tertiary unit is distant [63].
Four-dimensional image acquisition demonstrated a promising ability to adequately recognize fetal cardiac structures within all gestational ages via asynchronous transmission [25,79,80]. Vinals and colleagues exhibited a moderate interobserver concordance (Kappa > 0.6) within 14 out of 18 intracardiac structures assessed within the first trimester [79]. However, the study sample size was small (35 fetuses), and postnatal diagnosis verification was limited. An earlier study by the same team, conducted on later gestation fetuses, achieved a complete cardiac examination within 86%–95% of cases (single observer with two independent operators) [80]. Contrastingly, a later study by Adriaanse and colleagues whereby three observers analyzed 10 second-trimester cases demonstrated a perfect agreement for pathology identification in only 20% of cases [25].
The specialist nature of these modalities represents their main weaknesses to widespread implementation and currently may be best suited as an adjunct rather than a replacement to two-dimensional ultrasound. A summary of studies can be seen in Table 6.
Table 6: Summary of studies using three- and four-dimensional teleultrasound.
Robotic ultrasound.
The implementation of robotic obstetric teleultrasound remains theoretically plausible; however, the beneficial applications remain doubtful [23,24,26–28,91]. Studies demonstrated that transmission could be conducted across far distances (up to 7,000 km), primarily synchronously, with reasonable visualization of general anatomical structures [24, 27, 28]. Intraclass correlation between robotic teleultrasound and conventional ultrasound was high (>0.90) for the four main biometric measurements taken, reported by two studies. [23,91]. However, key anatomical features, such as the cavum septum pellucidum were only visualized in a third of cases using robotic ultrasound versus 100% of conventional two-dimensional ultrasound cases, as noted by Adams and colleagues [23]. Transmission delays were a common barrier for achieving adequate scans, resulting in lag on the expert’s side, thus leading to poor visualization of anatomical structures [24, 28]. This attributed to an extended time for scan completion compared to conventional scanning [26,91]. Furthermore, operators of the robotic device itself were often inexperienced, leading to frequent repositioning of the scan probe and difficulties for the expert to achieve all the images required [27]. However, patient satisfaction was high, noting a reduction in long-distance travel as a main benefit of this technology [91]. A summary of studies using robotic teleultrasound can be seen in Table 7.
Table 7: Summary of studies using robotic teleultrasound.
Low- and middle-income countries.
In 10 studies, teleultrasound services were conducted in low- and middle-income countries across all gestations [6,40,41,50,52,79,81,84,90]. Low-cost tele-transmission services were feasible to develop with minimal overall loss to image quality [40,41]. Four studies examined point-of-care ultrasound (POCUS), utilized by healthcare professionals who were inexperienced with ultrasound, combined with tele-supervision by trained clinicians [50,52,81,84]. Studies frequently incorporated an in-depth multi-week training curriculum, enabling operators to develop a strong understanding of obstetric ultrasonography [50,52,81,84,85]. Operators were able to acquire a range of fetal anatomical assessments with high concordance when the same images were viewed by independent obstetricians [50,84,85]. Continued tele-mentoring facilitated updated learning and continued clinical improvement and the adoption of interprofessional task sharing with capacity building enabled an improvement in ultrasound accessibility in pre-hospital sectors [52,81]. A consistent approach to continued verification of ultrasound scans and evaluation of outcomes by experienced staff facilitated a safe approach in areas with minimal technological infrastructure. The low cost of the devices was highlighted as a critical enabler for providing ultrasound services to economically strained countries [50,52]. Teleultrasound in low- and middle-income countries provides an avenue to improve access to maternity care in areas known to have disproportionately high adverse perinatal outcomes compared to higher-income countries. A summary of studies using teleultrasound in low- and middle-income countries can be seen in Table 8.
Table 8: Summary of studies recruiting in low-and middle-income countries.
Patient and provider experiences.
Five of the 61 aforementioned studies primarily evaluated patient and provider experiences with teleultrasound services [31,46,52,61,76]. Obstetric teleultrasound was associated with improved patient satisfaction, with many preferring subsequent teleultrasound scans, irrespective of the outcome of the antenatal scan findings [61]. Patients also cited high satisfaction for reduced travel to consultations [61,76,87,89]. Many studies examined patient satisfaction using a 5-point Likert scale, frequently reporting scores between 4 and 5 out of 5 [23,24,34,36,50,54,61,70,74,76,77,82,89].
Stakeholders cited benefits of teleultrasound in relation to timely identification of high-risk pregnancies and improved access to antenatal services, which enabled a balance in healthcare equity across obstetric communities [31,46,52]. Service users cited preference over synchronous versus asynchronous teleultrasound transmission [46]. Whilst initial challenges were noted by sonographers in relation to anxiety and pressure from real-time observation by senior clinicians, the iterative nature of the studies meant that barriers were addressed swiftly and reconfigured into beneficial factors [31]. Upskilling, increased access to timely specialist feedback and improved management of complex pregnancies were cited as the main benefits for service users [31,45]. Additional studies cited an increase in clinician confidence with teleultrasound using a Likert scale [25,34,46,50,60,84]. Clinician satisfaction was also rated highly among several studies [23,31,46,50,51,60,81]. A summary of qualitative studies can be seen in Table 9.
Table 9: Summary of included qualitative studies.
Economic burden.
Four studies primarily evaluated economic outcomes, with additional studies examined cost outcomes alongside clinical outcomes [29,30,35,36,38,45,50,58,64,85,86]. Initial startup cost for adequate technological infrastructure was high, ranging from 101,750 [29,30,45,58,85]. The economic burden was noted to be higher for earlier published studies (101,750 in 1998) [[58](#pmed.1004922.ref058)], with more recent studies demonstrating a reduction in implementation costs of 10,355–$22,450 [29,85]. However, the number of scans performed in the earliest study was 600 per month across 3 centers [58], whilst more recently published studies included 804 in a single year [85], and 322 over 48 months [29]. Consequently, the frequency of scans performed is an important consideration when interpreting the economic burden. The cost of an individual teleultrasound encounter was frequently less than standard care; noted to be up to nine times less by Cuneo and colleagues [29,30,36,86]. Studies reported substantial overall monthly non-fixed cost savings using teleultrasound, enabling recovery of fixed implementation costs within 12–14 months [35,58]. Dowie and colleagues demonstrated that the cost of a telemedicine encounter was greater than face-to-face consultation (£206 versus £74), however, within 14 days overall costs were neutral due to a reduction in travel costs [38]. The clinical application of the included studies, such as antenatal screening or antenatal diagnosis, did not seem to substantially influence the economic burden of teleultrasound implantation. Teleultrasound may be a viable option for antenatal care, however, high initial costs need to be mediated by offering the service to a wide cohort of women and for an extended duration. A summary of economic studies can be seen in Table 10.
Table 10: Summary of included economic evaluation studies.
A summary of the overall study findings, GRADE assessments, and future recommendations are in Table 11.
Table 11: Summary of existing evidence.
Discussion
This systematic review and meta-analysis was designed to comprehensively assess the role of teleultrasound for obstetric care by evaluating feasibility, diagnostic accuracy, acceptability, utility, and economic burden. Despite included studies demonstrating a high risk of bias, primarily due to methodological heterogeneity, obstetric teleultrasound was feasible in a wide range of settings. This included both synchronous and asynchronous transmission. However, at times the image quality was insufficient to clearly assess finer anatomical structures in more complex fetal anatomical tele-scans. This was in conjunction with bandwidth requirement, which was a crucial factor to enable adequate image quality and reduced transmission delay. Higher bandwidth requirements were more commonly seen in newer published studies, and feasibility studies including a clinical focus on improving access to specialist expertise in remote and deprived areas. However, overall meta-analysis between obstetric teleultrasound and the reference standards was non-inferior for identifying fetal and placental structures. The diagnostic accuracy of teleultrasound was highly discriminative (AUC 0.93). The false positive rate was 0.03 demonstrates teleultrasound is an excellent tool for low-risk cases. The sensitivity was moderate (0.4 (95% CI [0.44,0.84]), with wide CIs, suggesting teleultrasound may miss potential high-risk diagnoses if used as a sole screening tool. Initial results suggest novice ultrasound users can competently perform obstetric scans using low-cost devices with concurrent tele-supervision. Patient-operated teleultrasound devices were emerging in the literature, with initial assessments of basic fetal well-being performed in the home setting. Examination of ultrasound variants (robotic, three-dimensional, and four-dimensional teleultrasound) did not highlight a superiority to two-dimensional ultrasound. The specialist nature of these tele-scan types represents the main limitation for widespread implementation.
Overall acceptability ratings for obstetric teleultrasound were high for both patients and providers, citing common benefits in relation to satisfaction, reduced travel, economic savings, increased access to obstetric care and balance in healthcare equity. Whilst start-up costs for teleultrasound are high, overall costs were less in more recently published studies and could normally be accrued back over the subsequent months due to overall capital savings from the teleultrasound service versus routine care.
There was an underrepresentation of high-quality randomized controlled trials, suggesting a need for further research. Furthermore, current literature is limited in the reporting of clear methodological and technological capabilities of the teleultrasound systems, proving difficulty for researchers to replicate studies. Despite this, obstetric teleultrasound for antenatal care has flourished over recent years, demonstrating a growing body of evidence to support the digital migration of pregnancy care. Additionally, the evolving use of obstetric teleultrasound in community and home settings further supports one of the three main pillars of the recently published 10-year plan provided by the national health service in the UK [94]. Consequently, to support national objectives and future implementation, it is imperative for studies, particularly randomized controlled trials to consider a more standardized approach to study design, particularly regarding type of antenatal ultrasound, gestational age at time of ultrasound, the reference standard and clinical outcomes assessed. This will develop a greater cohesive and applicable body of evidence for obstetric teleultrasound which would enhance quantitative analysis and potentially aid in wider implementation.
Findings in this review align closely with previously published narrative literature on the use of teleultrasound for obstetric care [3,95,96]. The most recent review by Kariman and colleagues explores the use of obstetric ultrasound within 31 studies, highlighting similar findings to our review in relation to feasibility and acceptability of teleultrasound, however, included a more focused approach on point-of-care devices without incorporated teleultrasound [3]. Similarly to our review, a lack of high-level evidence was available, further highlighting a clear research requirement for future research, particularly assessing its impact on clinical maternal-fetal outcomes. Whilst the evaluation of teleultrasound on clinical outcomes such as adverse perinatal outcomes would be clinically useful, this may be troublesome given its rare occurrence, requiring a very large sample size to suitably assess. Therefore, usage of a composite perinatal outcome score, may be more preferable in future prospective studies; a factor that has been previously incorporated in recent high-level randomized controlled trials exploring alternative telemedicine obstetric interventions [97]. Vitally, alongside investigating feasibility and diagnostic accuracy, researchers should assess the impact of teleultrasound on other key service-led outcomes such as emergency hospital attendance and hospital admission, enabling a thorough understanding of the safety of such interventions. A health economics analysis is also encouraged to formally assess the economic burden of teleultrasound interventions.
In conjunction, teleultrasound usage has the potential to raise several ethical and regulatory issues which are imperative to consider when globally assessing obstetric teleultrasound functionality future high-evidenced studies, and the potential for wider rollout. Firstly, a detailed informed consent process is imperative, ensuring patients attain clarity on who will be interpreting the ultrasound scan if it is digitally transmitted. This is particularly important in asynchronous systems whereby the interpreting clinician may not be physically present and subsequent immediate explanation of the scan results is somewhat limited. This may lead to reduced patient satisfaction if this is not clearly explained during the consent process. Secondly, the reporting of essential technology security standards such as data encryption, data storage/retention, and liability in cross-jurisdictional teleultrasound usage is vital. Transmission of data should be watertight to minimize any breach of sensitive information. Data stored on cloud or shard databases must comply with data protection regulations such as the Health Insurance Portability and Accountability Act (HIPAA) in the USA and General Data Protection Regulation (GDPR) in Europe. Whilst cross-jurisdictional teleultrasound transmission may be necessary for certain study/clinical settings, different privacy laws may apply, complicating compliance and liability, particularly in uncommon situations where a fetal abnormality is missed. Thirdly, cost and reimbursement is an essential issue to consider when using teleultrasound on a wider scale. Insurance and national health systems may not yet have clear frameworks for teleultrasound reimbursement. This can limit equitable access to teleultrasound services and should be address prior to wider implementation. Maintaining professional standards and training in teleultrasound is also key to maximizing diagnostic and technical capabilities. The competency of remote operators requires continued training, whilst professional bodies (e.g., RCOG) should develop standards for teleultrasound practice, such as minimum technical requirements and quality assurance measures, This is a key facet for wider scale teleultrasound implementation. Finally, continued auditing of teleultrasound services is required, particularly in relation to clinical outcomes, patient satisfaction, and data portion. This is essential to maintaining ethical integrity.
Key themes in prior reviews suggest the need to produce a low-cost affordable teleultrasound system which enables clinicians to reduce the geographical and ethnic disparities that can be seen in obstetric care [3,89,90,95,96]. This is particularly important in low- and middle-income countries where the disparities in poorer obstetric outcomes are clear. There is some evidence to suggest that teleultrasound may benefit low- and middle-income countries, however, prior generalized reviews substantially underrepresent obstetric studies, suggesting further research in this area was required [8]. Our updated review provides insight into the recent work currently undertaken, particularly incorporating long-distance synchronous tele-transmission in pre-hospital settings using tele-supervision. In the absence of capacity to implement advanced healthcare infrastructure in such areas, the addition of basic telesonography services may prove beneficial and improve patient access to maternity care [4]. However, simple infrastructure requirements such as continuous electricity and costs for tele-system maintenance need to be considered and are perceived barriers to remote geographical implementation [98]. Importantly, almost half of the world’s population reside in remote areas, which can be susceptible to substandard telecommunication coverage [99]. Recent data suggests that even the least developed countries are capable of internet bandwidth connections of between 256 Kb/s and 2 Mb/s, suggesting teleultrasound implementation on the most basic level is plausible [100]. Needless to say, obstetric ultrasound training and subsequent regulation of antenatal teleultrasound services should be rigorous to reduce risk of harm secondary to improper use in this context. Therefore, measures to ensure consistent quality control should be integrated into future study design within low- and middle-income countries [4,101].
Interestingly, the integration of artificial intelligence (AI) into obstetric ultrasound has been explored. Blind abdominal sweeps using a low-cost device has recently been assessed in Zambia for first-trimester scanning, whereby accuracy was deemed similar to scans performed by trained sonographers [102]. This alludes to an alternative avenue for providing obstetric care in more deprived countries. However, clinicians incorporating AI must acknowledge certain technology-specific regulatory factors prior to wider implementation. This includes, but is not limited to, responsibility in the presence of an error, the requirement for continued technology validation, ensuring consistency of data production in the presence of diverse populations and ownership of the data that is produced.
This review contained a balance of synchronous and asynchronous transmission services. Asynchronous obstetric teleultrasound transmission may be more suitable on a global scale, as images can be transmitted over lower bandwidths and less reliable telecommunication channels, as concerns regarding transmission delays/lag become less important [4]. Asynchronous transmission may be suitable for scans requiring expert input, which can be infrequently attained within a timely fashion [103]. However, in the context of obstetrics, an emergency intervention may be warranted at times following antenatal ultrasound scanning. Therefore, synchronous transmission may be preferable for the majority of obstetric cases. Additionally, synchronous transmission facilitates a timely interaction between the patient and operator which fosters collaborative discussion surrounding subsequent antenatal care management and supports a patient-centered care [34,52]. In areas whereby telecommunication services are unequipped to transmit full quality images via synchronous transmission, an alternative approach is Remote Tast Scale [4]. This encompasses synchronous transmission of low-quality images followed by asynchronous transmission of high-quality images. No studies in this review explored this option, however, prior literature has examined this transmission type [5].
Crucially, the implementation of telehealth services is frequently in relation to clinician attitudes for endorsement. Qualitative assessment is limited in prior reviews, but initial insight in this review suggests high provider acceptability, suggesting a potential turning point in obstetric teleultrasound adoption [95,96]. Endorsement from both patients and clinicians regarding the novel emergence of remote patient-operated teleultrasound devices is high. Patient-operated devices may be a potential avenue for digital innovation which could modify how current antenatal care pathways are delivered [104,105]. However, presently, the device capabilities are limited to only simple assessments of fetal wellbeing [44,65,67,70,87,89,92,93]. The adjunct of AI and integration of sophisticated fetal assessments, such as remote biometry and Doppler, may enable clinicians to sophistically monitor patients at home and reduce the capacity concerns within current outpatient services.
Irrespective of technological advancements: a lack of digital literacy, presence of language barriers, and distrust in healthcare services by patients will remain as the main inhibitors to implementation. Such factors are more prominent in lower socioeconomic groups and ethnic minorities [106–108]. Therefore, it is imperative for future studies to support these patient groups, ensuring to promote patient education and empowerment via suitable teaching strategies and collaboration with interpreter services. Synchronous transmission may be a preferable option for such patient groups, particularly in the case of patient-operated teleultrasound devices.
Fig 9 represents a selection of barriers and/or facilitators for teleultrasound implementation, which have been stratified based on the evidence consolidated from this review. Minimization of barriers and adoption of facilitators may enable clinicians to achieve important beneficial teleultrasound outcomes listed at the bottom of the figure.
A schematic diagram illustrating several barriers and facilitators to achieving successful teleultrasound implementation.AI, artificial intelligence.
The extensive search, including gray literature and subsequent evaluation of a wide range of factors regarding teleultrasound represent the main strengths of this review. Importantly, this review enables clinicians and researchers to understand the current state of teleultrasound and determine how best this technology can be safely implemented into obstetric care. This review further facilitates clinicians to consider the technological requirements for teleultrasound optimization, whilst determining the elements required for robust future research. Furthermore, included studies derived from a range of countries, thus improving the generalizability of results.
Due to the variable quality of data and methodological heterogeneity of the included studies, meta-analysis was limited, particularly pairwise meta-analysis. A lack of consistent outcome reporting currently limits a deep quantitative analysis of obstetric teleultrasound. Additionally, due to the experimental nature of teleultrasound, it is plausible that many studies yielding negative results were never formally reported. From a technological perspective, this may be less important, given that the included studies within this review were sufficient to evaluate the beneficial and negative technological applications of teleultrasound. However, the presence of publication bias may have a greater impact on more serious outcomes, such as patient safety and adverse perinatal outcomes, which were difficult to assess due to the few studies included using obstetric teleultrasound within a clinical context. It is important to rationalize these areas for future use and further studies are warranted to include all domains for adequate quality-of-care evaluation [109]. Finally, 21% of included studies were more than 20 years old. Given the ever-evolving digital landscape and escalation in technology sophistication, the age of these studies may limit the relevance of their results to modern obstetric practice.
This review has demonstrated the potential applicability and value of teleultrasound for obstetrics across a range of outcomes. The rapid development of teleultrasound services aimed to address the current capacity concerns within outpatient obstetric services and the subsequent impacts this has on patients and providers. This novel care model is everchanging and new ultrasound devices capable of telesonography are of clinical and scientific relevance. It is imperative that studies ensure sufficient methodological detail and consistent outcome reporting to inform future study design. Presently, additional high-quality evidence is required, particularly using obstetric teleultrasound within a clinical context before recommendations can be made regarding teleultrasound as an alternative avenue for antenatal care.
Supporting information
S1 TablePRISMA checklist.From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, and colleagues. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. https://doi.org/10.1136/bmj.n71. This work is licensed under CC BY 4.0. To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/. For more information please see: https://www.prisma-statement.org/citing-prisma-2020 – PRISMA.(DOCX)
S2 TableSearch strategy.(DOCX)
S3 TableCritical appraisal checklist for observational studies.(DOCX)
S4 TableExcluded studies and associated reasons for exclusion.(DOCX)
S5 TableCritical appraisal results for all studies.(DOCX)
S6 TableDescription of study methodology.(DOCX)
S7 TableDiagnostic accuracy of teleultrasound within reporting studies, stratified by indication.(DOCX)
S1 FigSingle variable proportional meta-analysis of identification rates for fetal and placental structures using teleultrasound, stratified by body system.(PDF)
S2 FigSingle variable proportional meta-analysis of diagnostic accuracy rates for teleultrasound.(*) represents the reference standard was conventional in-hospital ultrasound. (^) represented the reference standard was postnatal diagnosis.(TIF)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Statistics Of N. Birth characteristics in England and Wales: 2021 2023 [cited 02 Feb 2025]. Available from: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/livebirths/bulletins/birthcharacteristicsinenglandandwales/2021
- 2Kern-Goldberger AR, Srinivas SK. Telemedicine in obstetrics. Clin Perinatol. 2020;47(4):743–57.33153659 10.1016/j.clp.2020.08.007 · doi ↗ · pubmed ↗
- 3Kariman SS, van den Heuvel JFM, Adriaanse BME, Oepkes D, Bekker MN. The potential of tele-ultrasound, handheld and self-operated ultrasound in pregnancy care: a systematic review. Prenat Diagn. 2024.10.1002/pd.6679 PMC 1218057439390612 · doi ↗ · pubmed ↗
- 4Marsh-Feiley G, Eadie L, Wilson P. Telesonography in emergency medicine: a systematic review. P Lo S One. 2018;13(5):e 0194840. doi: 10.1371/journal.pone.0194840 29723198 PMC 5933714 · doi ↗ · pubmed ↗
- 5Ferreira AC, O’Mahony E, Oliani AH, Araujo Júnior E, da Silva Costa F. Teleultrasound: historical perspective and clinical application. Int J Telemed Appl. 2015;2015:306259. doi: 10.1155/2015/306259 25810717 PMC 4355341 · doi ↗ · pubmed ↗
- 6Gallimore ID, Matthews RJ, Page GL, Smith LK, Fenton AC, Knight M. MBRRACE-UK perinatal mortality surveillance: UK perinatal deaths of babies born in 2022—state of the nation report. Leicester: The Infant Mortality and Morbidity Studies, Department of Population Health Sciences, University of Leicester; 2024.
- 7Gyselaers W, Lanssens D, Perry H, Khalil A. Mobile health applications for prenatal assessment and monitoring. Curr Pharm Des. 2019;25(5):615–23. doi: 10.2174/1381612825666190320140659 30894100 · doi ↗ · pubmed ↗
- 8Britton N, Miller MA, Safadi S, Siegel A, Levine AR, Mc Curdy MT. Tele-ultrasound in resource-limited settings: a systematic review. Front Public Health. 2019;7:244. doi: 10.3389/fpubh.2019.00244 31552212 PMC 6738135 · doi ↗ · pubmed ↗