NTDscope: A multi-contrast portable microscope for disease diagnosis
María Díaz de León Derby, Zaina L. Moussa, Carlos F. Ng, Abdul M. Bhuiya, Joana P. Cabrera, Dipayan Banik, Charles B. Delahunt, Matthew D. Keller, Anne-Laure M. Le Ny, Jaime Garcia-Villena, Elena Dacal, David Bermejo-Peláez, Daniel Cuadrado, Miguel Luengo-Oroz

TL;DR
The NTDscope is a portable diagnostic device that combines microscopy and molecular testing to detect diseases in resource-limited areas.
Contribution
The NTDscope integrates multiple imaging and molecular diagnostic methods into a single portable device for NTD diagnosis.
Findings
The NTDscope functions as a brightfield, darkfield, and fluorescence microscope for parasite detection.
It can quantify molecular assays like lateral flow tests and CRISPR-based assays.
The device improves robustness and expands diagnostic applications in low-resource settings.
Abstract
Accurate diagnostics are essential for disease control and elimination efforts. However, access to diagnostics for neglected tropical diseases (NTDs) is hindered by limited healthcare infrastructure in many NTD-endemic regions, as well as by reliance on time- and labor-intensive diagnostic methods, such as smear microscopy. New diagnostic tools that are portable, rapid, low-cost, and meet World Health Organization (WHO) sensitivity and specificity targets are urgently needed to accelerate NTD control and elimination programs. Here, we introduce the NTDscope, a portable microscopy platform that enables point-of-care imaging and automated detection of parasites and other pathogens in patient samples. The NTDscope builds on and extends the capabilities of the LoaScope, a device that turned the camera of a mobile phone into a microscope and used on-board image processing to automatically…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
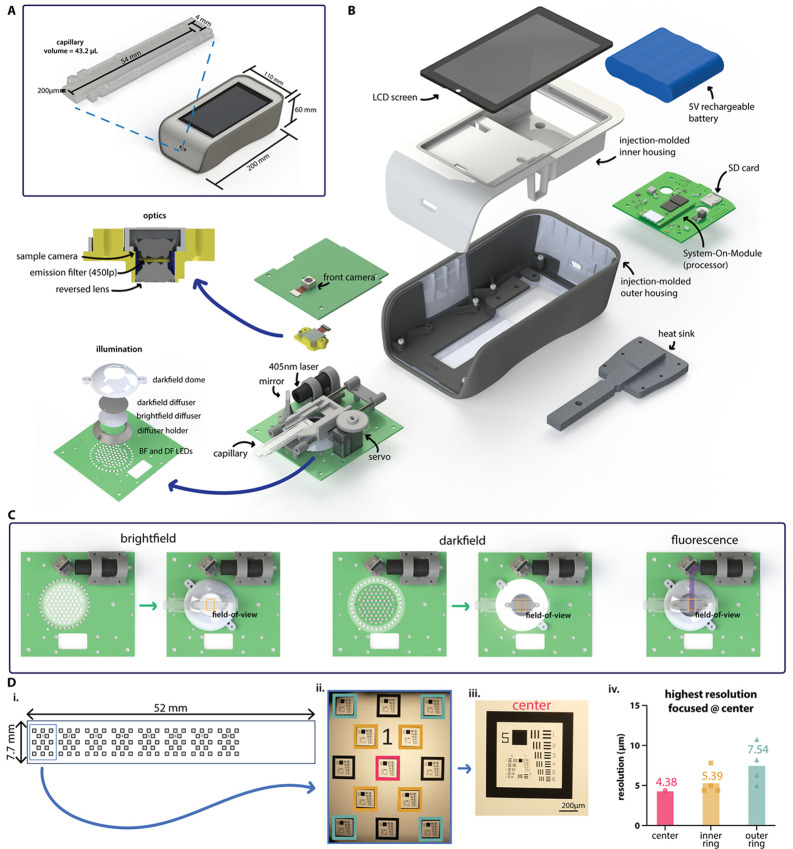 Fig 1
Fig 1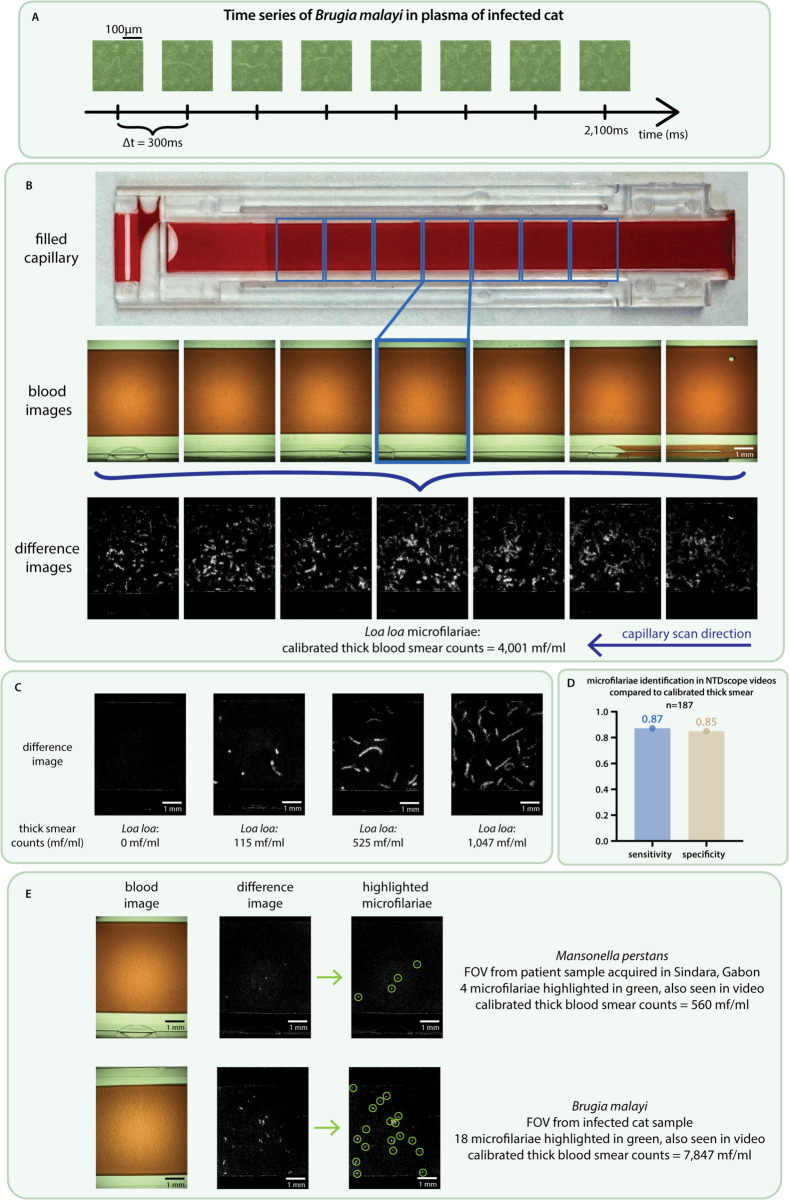 Fig 2
Fig 2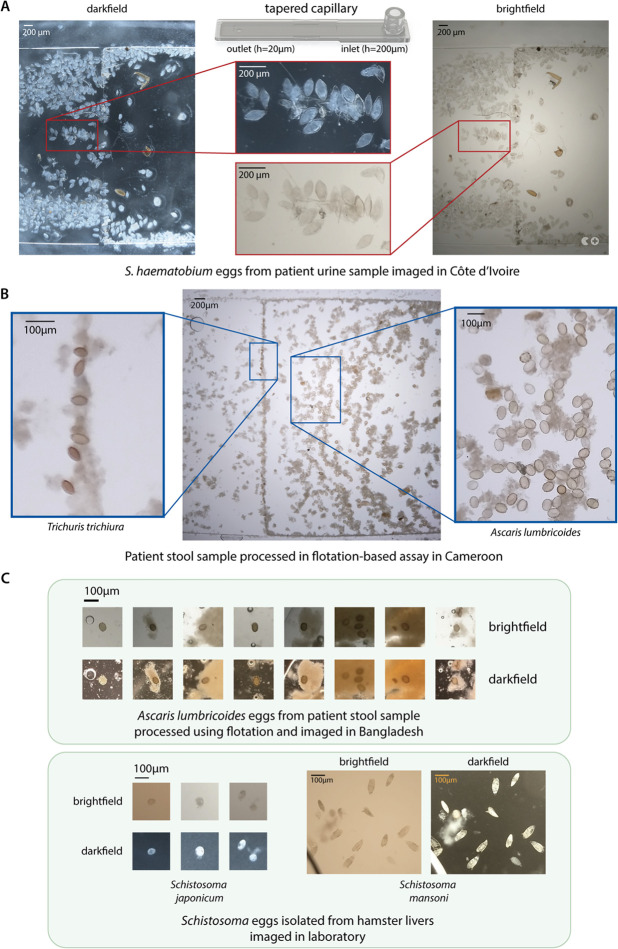 Fig 3
Fig 3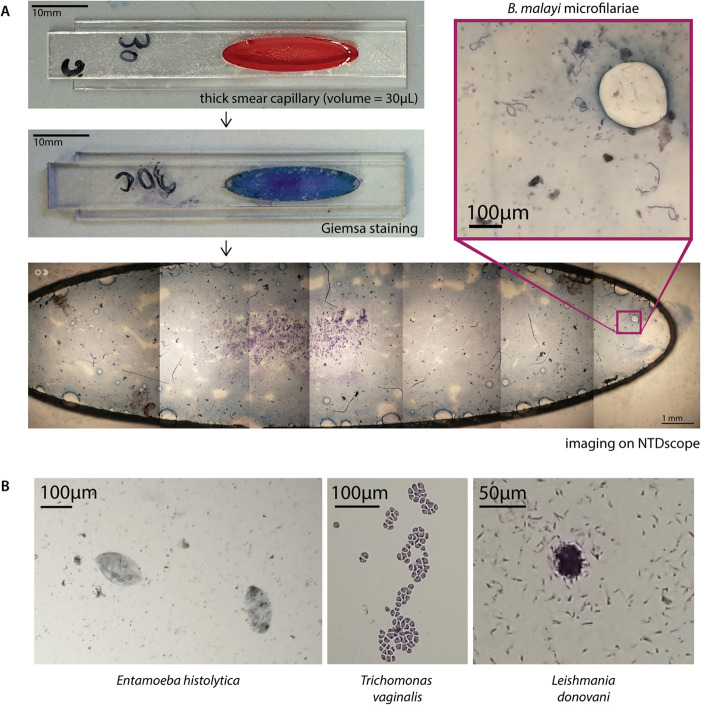 Fig 4
Fig 4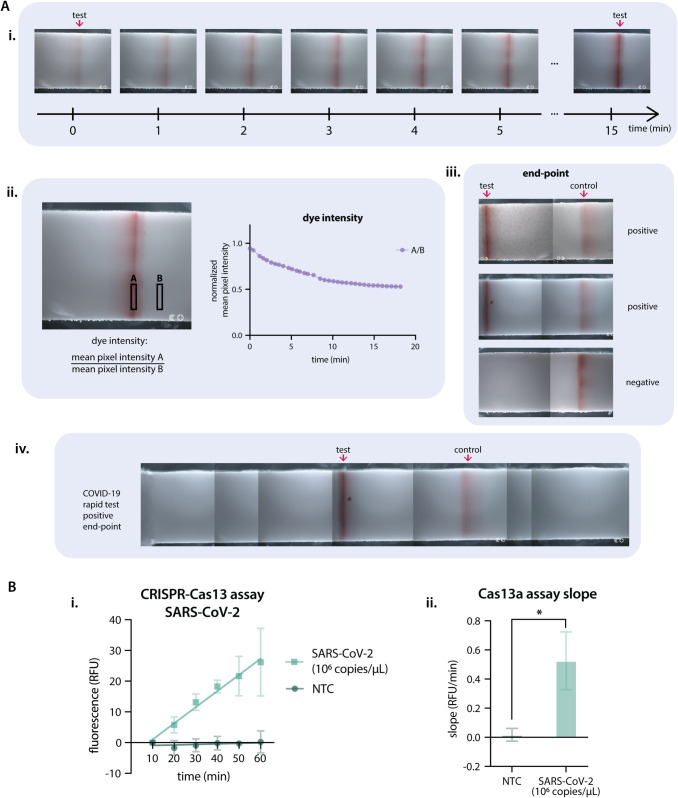 Fig 5
Fig 5- —http://dx.doi.org/10.13039/100000865Bill and Melinda Gates Foundation
- —Harvey and Leslie Wagner Foundation
- —Mitsuru and Lucinda Igarashi Fund
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParasitic Diseases Research and Treatment · Biosensors and Analytical Detection · Digital Imaging for Blood Diseases
Introduction
Despite ongoing disease control and elimination efforts, neglected tropical diseases (NTDs) impact over one billion of the world’s most vulnerable individuals. For some NTDs, identification of individuals in need of treatment or verification of mass drug administration efficacy remains a major challenge [1–3]. Limited healthcare infrastructure in some NTD-endemic regions means that diagnostics must be brought to individuals, rather than individuals going to local clinics for testing. In the absence of point-of-care diagnostics, samples must be transported to a centralized facility for preparation and analysis, resulting in long delays and challenges in returning test results to specific individuals. While lateral flow assays and other molecular tests have simplified identification of some diseases, point-of-care molecular tests for NTDs including schistosomiasis, soil-transmitted helminths, and filarial infections are in limited use or still in development [4–12].
As a result, diagnosis of many NTDs continues to rely on conventional methods, such as thick smear microscopy for filarial parasites like Loa loa and urine microscopy for Schistosoma haematobium eggs. New approaches that are faster, cheaper, and more accurate than conventional microscopy are urgently needed to accelerate NTD control and elimination programs, with an emphasis on diagnostics that can enable rapid point-of-care testing of individuals, support starting and stopping decisions for mass drug administration (MDA) campaigns, and monitor re-emergence and spread of infections [1–3,13–17].
Diagnostic strategies that can detect multiple NTDs are particularly compelling, given the limited resources in many NTD-endemic regions [14,17,18] and the need to keep costs per test as low as possible. It may be more cost-effective to have a single device diagnose multiple diseases than to develop separate assays using separate equipment. For example, automated slide-scanning microscopes that can image different types of prepared patient samples (e.g., blood, urine, or stool) have recently been developed [19–24], offering versatility in pathological diagnostics. However, these devices are often bulky, sometimes requiring the use of a separate computer, and are constrained by sample preparation methods that are typically slow and labor intensive, such as fixing and staining a blood smear. They also require technical expertise to run and interpret data, though machine learning algorithms are being developed to automate interpretation [19–21,23,25–34].
To increase accessibility of diagnostic strategies in low-resource settings, many groups have employed mobile phones (or mobile phone components) for the detection of NTDs and other infectious diseases [25,35–44]. For example, our group previously developed a point-of-care diagnostic device called the LoaScope to identify patients who should not be treated during onchocerciasis MDA campaigns to avoid the potential for serious adverse events that are known to occur at high Loa loa microfilarial loads [45]. The LoaScope was designed to be a portable, field-friendly microscope that involved minimal sample preparation and provided rapid (<5 min) point-of-care quantification of microfilariae in peripheral whole blood [46]. The device was successfully used to quantify the Loa loa microfilarial load of >16,000 people in Cameroon as part of a Test-and-Not-Treat program to resume ivermectin MDA for onchocerciasis in Loa-endemic regions [47]. The LoaScope harnessed the camera of a mobile phone and a reversed lens optical system [48], together with 3D-printed components and consumer electronics for illumination and sample translation. Sample preparation and imaging were simplified by loading patient peripheral blood into a disposable capillary with a rectangular cross-section that could be directly inserted into the LoaScope for imaging [46].
Since the LoaScope has sufficient resolution to capture images of parasite eggs, we tested whether the device could be used for the detection of Schistosoma haematobium eggs in urine samples. We developed a tapered version of the capillary that captures particles greater than 20μm and used it to filter and concentrate S. haematobium eggs from patient samples [32]. We used a new version of the LoaScope with darkfield illumination capabilities, called the SchistoScope, to image the concentrated eggs in Ghana and Côte d’Ivoire [32,49,50]. Darkfield images proved to be useful for identification of eggs, demonstrating that the LoaScope could expand its applications to other NTDs [34].
Here, we present the next generation of the LoaScope, renamed the NTDscope for its additional capabilities that expand the set of potential diagnostic applications. The NTDscope provides multi-contrast portable imaging for both microscopy applications and detection of molecular assays. Rather than using a phone itself, the NTDscope uses specific mobile phone components, such as camera modules, a rechargeable battery, and sensors, allowing the parts to be configured into an integrated and portable platform. As in the LoaScope, the new device takes advantage of a low-cost reversed lens optical system with a wide field of view (FOV) [48] and uses single-axis motion for acquisition of multiple images and videos of samples in capillaries. User-facing software is based on Android, and cloud connectivity enables data upload and remote software updates. The upgraded computing capabilities of the NTDscope support the use of machine learning (ML) algorithms for automated disease identification.
Below, we outline the technical specifications of the NTDscope and demonstrate both current and future use cases, including video capture of live microfilarial and Schistosoma samples, multi-contrast imaging of parasitic eggs, imaging of stained samples, and detection of molecular assays. The NTDscope has the potential to become a platform technology that addresses image-based and molecular diagnostic needs for multiple NTDs and serves as a key element of decentralized healthcare in the future.
Materials and methods
Ethics statement
This work contains images and videos of patient samples from four separate studies conducted in Cameroon, Gabon, Côte d’Ivoire, and Bangladesh.
The study in Cameroon was conducted in the Awae Health District, located in the Mefouet-Afamba Division, between September and October of 2023. Finger prick blood was collected from study participants. Ethical permission for this study was granted by the Centre Regional Ethical Committee for Research on Human Health (CRERSH-Ce; CE N^°^/CRERSHC/2023) and administrative authorization was obtained from the Centre Regional Delegation for Public Health of the Ministry of Public Health. Participants were recruited between September 26 and October 14 of 2023. Study participants signed informed consents.
The study in Gabon was conducted in the Sindara and Lambaréné regions in August of 2023. Finger prick blood was collected from study participants. Ethical permission for this study was granted by the Comité d’ethique Institutionnel du CERMEL (CEI-026/2022). Participants were recruited between August 13-24 of 2023. Adults 18 years or older were invited to participate and provided a written informed consent.
The study in Côte d’Ivoire was conducted around the town of Azaguié in January of 2024. Ethical permission was granted by the University Health Network, Toronto, Canada (REB #21-5582) and the Comité National d’Éthique des Sciences de la Vie et de la Santé, Abidjan, Côte d’Ivoire (REB #138-23/MSHPCMU/CNESVS-km). Ethical permission was also granted by the local health district officer. Community members aged five and older were asked to provide a urine sample. Adults provided written consent and assenting children who had written consent from a parent or guardian were included. Participants were recruited and data was collected from January 15-16, 2024.
The study in Bangladesh was conducted from October 2019 - December 2020 in the Rohingya Refugees camp in Bangladesh. Ethical permission for this study was granted by the International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b) Institutional Review Board (research protocol #PR-19014). Children who were residents of the camp and seeking care from icddr,b-operated Diarrhoea Treatment Centre were asked to participate by providing stool samples. Children were included if they assented and had written consent from a parent or guardian. Banked stool samples were used for the purposes of this paper, the samples were accessed from June 29, 2024 to October 20, 2024. Participants and their guardians were informed that unused samples would be stored for future use, and at any time participants and their guardians could contact the study team if they wished for the samples to be discarded and not saved. The study team had no access to information that could identify individual participants during or after data collection.
Inclusivity in global research
Additional information regarding the ethical, cultural, and scientific considerations specific to inclusivity in global research is included in the Supporting Information (S1 Checklist).
External dimensions
The NTDScope has dimensions of 200mm (L) x 110mm (W) x 60mm (H) and weighs 880 grams. A diagram of the device and its main components is found in Fig 1. The injection-molded top housing holds a rechargeable Lithium-ion 3.7V battery and an LCD screen display. The bottom housing is composed of two pieces: a structural carriage and an outer protective housing with an over-molded elastomeric shell. The bottom housing holds the electrical boards, optical system, and a heat sink for the System-On-Module (SOM) and illumination board. Charging of the battery is done via USB-C, and battery life in field settings in Cameroon and Gabon has been observed to be around 6 hours.
NTDscope design, illumination, and resolution.A: Diagram showing NTDscope and straight channel capillary external dimensions. B: Exploded view of NTDscope and main components. C: NTDscope illumination modes, showing brightfield, darkfield, and fluorescence illumination. D: NTDscope resolution measurements, showing design of custom slide with USAF resolution targets (D.i.), image of USAF resolution target array acquired on NTDscope used to measure resolution, with the resolution targets used in calculations color coded with pink (center), yellow (inner ring) and green (outer ring) (D.ii.), close-up of center resolution target (D.iii.), and resolution measurements at each target location, showing root mean square of horizontal and vertical resolution measurements (D.iv.). Data was processed and visualized using GraphPad Prism 10.
Electronics and processor
Instead of a mobile phone, the NTDscope uses a series of three electronics boards containing connections to power, processors, sensors, and actuators. It is based around a System-On-Module (SOM)(Open-Q 660μSOM, Intrinsyc) that features a Qualcomm SDM660 processor. The main control carrier board (CCB) connects the battery, LCD screen, SD card for storage (256GB), and SOM board. The illumination board has connections for the brightfield and darkfield LEDs and laser for fluorescence, as well as to a servomotor used to move the capillary carriage. Certain hardware components, including the carriage translation system, the fluorescence illumination components, and the servomotor, are also attached to the illumination board. Finally, the camera board contains connections for the sample and front cameras.
Imaging system
The sample camera uses a SONY IMX586 sensor, with a 6.4mm x 4.8mm active area comprised of 48 megapixels of 0.8μm pitch, arranged in a quad-Bayer array which thus has an effective pixel pitch of 3.2μm for the red and blue pixels and 2.3μm for the (45^°^ rotated compared to red and blue) green pixel array [51]. The optical train is a reversed-lens configuration using Largan Precision lenses and provides a measured on-axis resolution of 4.4μm (Fig 1D) with a (measured) magnification of M=1.00. The optical image area exceeds the sensor dimensions, resulting in a sensor-limited field of view. The system also includes an external front camera, with a SONY IMX214 sensor (13 megapixels and 1.12μm effective pixel size [52]), which is not a part of the reversed lens system but can be used to scan patient barcodes during diagnostic field studies.
Optical resolution
The NTDscope optical system consists of a reversed-lens system [48] with lenses of f-number f/1.8 and a camera sensor with a quad-Bayer array as described above [51,53]. The green pixels in the array have a peak transmission of 525nm, and for that wavelength theoretical on-axis optical resolution is, per the Rayleigh formula, δr 1.2μm. Actual obtained resolution is limited by undersampling of the image by the sensor pixel array; typical mobile-phone cameras are designed to have significant modulation transfer function (MTF) at Nyquist (i.e., undersampling) to increase field of view at the expense of aliasing. In the case of the NTDscope, for an f/1.8 undersampling is >4.8X in the green, based on the 2.3μm pitch (for green pixels) and the magnification, wavelength, and f-number based Nyquist sampling pitch requirement. This leads to a rough expected (aliasing-limited) on-axis resolution of δr ∼ 5.5μm, consistent with measurements using a custom glass resolution target the size of a capillary, containing numerous arrangements of the 1951 USAF target (Opto-Line International), which yield consistent on-axis resolution better than 4.4μm (228 lp/mm, the limit of the resolution target, Fig 1D). The best resolution in the horizontal and vertical directions at different locations in the field of view was measured using Fiji ImageJ. A line was drawn over the horizontal and vertical USAF target line pairs starting with those corresponding to the highest resolution, a line scan was generated, and the Michelson contrast was calculated using the maximum and minimum pixel values in the line scan. The resolution at each FOV location was considered to be that corresponding to the first elements with a Michelson contrast above 10%. The slightly better-than-expected on-axis resolution is attributable to the uncertainty in estimating sampling-limited resolution as well as the image processing done in the camera firmware based on the additional true 0.8μm pitch of the pixels in the quad-Bayer arrangement. Optical resolution at the extreme edge of the field of view (at 4mm radius) is expected to degrade by a factor of about (to δr ∼1.8μm along the radial direction) due to NA-limiting from pupil obliquity and increased image distance based on the 37^°^ maximum field angle. USAF target data for extreme field radii are consistent with this, limited again to ≥4.4μm (optically, by expected aliasing issues as discussed, and, in terms of measurement, by the available feature sizes of the test target.) Focus gradients due to imperfect stage alignment in these (small-batch produced, and thus larger-toleranced) devices resulted in worst-case resolution of 10μm at the extrema of the FOV (measurements were taken at an average 2.7mm from the FOV center, (Fig 1D.iv.)), which remains more than sufficient for use with 100μm or greater sized filarial worms as well as for Schistosoma and soil-transmitted helminth eggs.
Brightfield and darkfield illumination
The system is illuminated by an inner ring consisting of 74 LEDs and an outer ring of 35 LEDs. Illumination of the inner ring is used to produce brightfield imaging, while illumination of the outer ring allows for darkfield capabilities, as shown in Fig 1C. Directly above the illumination LEDs, a diffuser holder hosts a brightfield diffuser, creating uniform illumination across the field of view, and a black, darkfield diffuser, which is used to prevent reflections during darkfield illumination while allowing transmission of brightfield LED illumination. A dome-shaped plastic part, the darkfield dome, surrounds the illumination LEDs and directs light from the outer LED ring towards the edges of the field of view during darkfield illumination.
Fluorescence illumination and emission
Fluorescence illumination uses a laser (405 nm, 50 mW), a mirror, and a set of interference filters suitable for fluorophores such as Alexa Fluor 405, Alexa Fluor 430, ATTO 390, ATTO 425, ATTO 465, etc. The laser is positioned parallel to the NTDscope sample holder, such that the beam hits a mirror oriented at 45^°^ to direct the beam towards the edge of the sample. The excitation filter (CT405/10x, Chroma Technology Corp) is attached directly to the laser. The emission filter (CT450lp, Chroma Technology Corp) is positioned between the reversed lens and the camera module on the collection optics. A diagram showing fluorescence illumination is shown in Fig 1C.
Sample capillary and translation
The NTDscope sample carriage accepts capillaries or other samples with outer dimensions 12mm x 59mm x 1mm, compatible with the original LoaScope capillaries. The carriage moves in one dimension and is able to capture seven distinct FOVs. The original capillary, developed for imaging Loa loa microfilariae (mf) in peripheral blood, has a channel with dimensions of 54mm x 4mm x 200μm (Fig 1A), holding a total blood volume of 43.2μL. Each of the seven distinct FOVs that can be imaged covers a volume of 4.96μL of blood, for a total of 34.72μL per capillary. In addition to the rectangular capillary, we iterated on the design to create capillaries for other use cases, conserving the external dimensions to retain compatibility with the NTDscope carriage. Examples of this include, a tapered capillary for processing urine and stool samples, shown in Fig 3, and a thick smear capillary, shown in Fig 4.
Software
The NTDScope runs on Android 9 operating system (OS). Given the operating system, machine learning (ML) algorithms tailored to specific neglected tropical diseases can be loaded onto the device for automatic pathogen detection [54,55]. We developed custom Android applications (apps) for the NTDscope, enabling control of the sample location, focus, capture of images and videos, etc. The location of the sample is controlled via software by rotating a servomotor gear attached to the capillary carriage. Focus is controlled by vertical translation of the camera lens module. Brightfield and darkfield illumination are controlled via software by turning on the central (brightfield) or outer ring (darkfield) LEDs. Flourescence illumination is achieved by activating the laser. A custom app was developed for the quantification of Loa loa burden, and was tested in rural field settings in Cameroon and Gabon. This app allows the user to capture patient information (with an option to read patient-associated barcodes), and insert a blood-filled capillary, after which it automatically captures five-second videos in seven different locations along the capillary, translating it before each new acquisition. After imaging, the sample videos are processed and the Loa loa burden is quantified and reported.
Sample preparation
Microfilariae sample preparation.
Samples of patients infected with Loa loa and Mansonella perstans, as validated by calibrated thick blood smears, were acquired in Cameroon and Gabon. To fill the capillaries, a patient fingertip was pricked with a lancet and peripheral blood was wicked into the capillaries via capillary action (as described in [46]). The blood-filled capillaries were then inserted into the NTDscope, and five-second videos of seven distinct FOVs of each sample were captured, with the capillary automatically translated by the servomotor between each imaged FOV. Videos can be automatically analyzed for mf detection using software loaded on the device. Patient sample videos were processed by an algorithm that subtracts subsequent frames to generate difference images (as described in [46]).
We used patient sample videos collected in Gabon to compare the performance of manual counts of microfilariae in videos acquired on the NTDscope to microfilariae detection in calibrated thick smears. Data from 187 patients in the Lambaréné and Sindara regions of Gabon, both endemic for Loa loa and M. perstans, was used. For each patient, two calibrated 50μL thick blood smears were prepared and analyzed using a standard light microscope. Patients were considered microfilariae-positive via thick smear if at least one worm of either Loa loa or M. perstans was found in the total examined volume. Original videos and the difference images generated from those videos were used to count microfilariae. A patient was considered positive on the NTDscope if microfilarial motion was observed at least once in the seven videos acquired, and negative otherwise.
We also used blood and plasma samples of cats infected with live Brugia malayi microfilariae (provided by the Filariasis Research Reagent Resource Center for distribution through BEI Resources, NIAID, NIH). For these samples, blood and plasma were pipetted directly into the NTDscope capillaries. To capture videos of plasma, the cat blood was left to separate into its components overnight, after which 43.2 μL of the supernatant (corresponding to plasma) were pipetted into a NTDscope rectangular capillary for video acquisition. We used whole blood to determine the expected correlation between the actual microfilariae concentration in a sample and the number of microfilariae that could be identified from the videos acquired on the NTDscope. We prepared three capillaries and two calibrated thick smears from a sample of a cat infected with B. malayi. We then manually counted worm movements in the videos and counted the visible mf in the calibrated thick smears.
Schistosoma and STH sample preparation.
We used a tapered capillary to process urine and stool samples for imaging on the NTDscope. The capillary has a rectangular channel with a height that tapers down from 200μm near the inlet to 20μm near the outlet hole. These capillaries can be connected to a syringe to easily flow liquids through, including urine and stool processed with a flotation solution. The tapered design ensures that parasite eggs are trapped along the channel, at a location dependent on their size. The external dimensions of the tapered capillary are such that it can be inserted into the NTDscope carriage for imaging.
The Mini-FLOTAC technique [58] was used to image soil-transmitted helminth (STH) eggs found in patient stool samples. The stool was homogenized and mixed with a flotation solution (using a kit called the Fill-FLOTAC), such that eggs can be concentrated and separated from stool particulates. After flotation, the samples were loaded into the Mini-FLOTAC apparatus, which is used for microscopic examination of the sample and identification of parasitic eggs. We used the FLOTAC technique to process stool samples taken from a patient with known STH infection in Cameroon. The floated stool solution was then injected into a tapered capillary and imaged on the NTDscope.
A device called the Fecalyzer, which is commonly used for veterinary applications, was used to process stool samples for imaging [59]. 0.2 grams of stool were homogenized and 14 mL of a zinc sulfate (ZnSO4) flotation solution was added such that a meniscus formed. We developed a prototype capillary using two thin pieces of laser-cut acrylic coated with a hydrophilic solution (Tetronic 904 dissolved in isopropanol alcohol), that could be inserted into the NTDscope for imaging. We placed the coated acrylic pieces on top of the meniscus and waited 15 minutes to allow the STH eggs in the stool sample to float to the top and adhere to the acrylic surface. The acrylic pieces were then removed and imaged on the NTDscope.
Thick smear and LFA sample preparation.
To image thick smears on the NTDscope, a compatible capillary was made from laser cut-pieces of acrylic and coated with a hydrophilic solution (Tetronic 904 in isopropanol alcohol). We prepared a thick smear capillary using a 30μL blood sample of a cat infected with B. malayi microfilariae, stained using Giemsa and imaged with the NTDscope.
To test the ability of the NTDscope to quantify lateral flow assays (LFAs), we imaged two commercially-available lateral flow assay strips for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) antigen detection, one processed using a positive patient sample and one using a negative patient sample. The lateral flow strips were removed from their plastic housing and attached to a glass support with dimensions of the NTDscope carriage. The patient nasal swabs were collected and processed according to the manufacturer, and the three drops of swab solution and assay components were added to the strips and immediately imaged using the NTDscope. For the positive sample, images of the test line were acquired every minute for five minutes. End-point images were also acquired 15 minutes after the start of the assay.
CRISPR-Cas13a assay preparation.
As previously described [62], we used CRISPR (Clustered Regularly Interspaced Short Palindromic Repeats)-Cas13a with a CRISPR RNA (crRNA, also known as a guide RNA) to recognize a specific sequence in the SARS-CoV-2 N gene. The crRNA is incubated with the Cas13a enzyme to form a ribonucleoprotein that is activated to nonspecifically cleave a ssRNA reporter-quencher upon target sequence recognition. The enzyme Cas13a was expressed and purified as previously described, and the crRNA for SARS-CoV-2 and a synthetic target were ordered from Synthego [62]. The ssRNA reporter-quencher was modified from [62] to include a 5’ ATTO425 fluorophore and a 3’ IowaBlack FQ quencher. The assay was prepared by preassembling Cas13a-crRNA RNP complexes for 15 minutes at room temperature, after which the ssRNA reporter and the target RNA at either 1 × 10^6^ copies of RNA per μL (cp/μL) for positive controls or 0 cp/μL for the non-target control (NTC) were added.
For NTDscope fluorescence measurements, the CRISPR-Cas13a reactions were loaded individually into two-5μL glass capillaries (Vitrocom, cat# 5010-050), which were attached to a modified glass slide (12mm x 75mm x 1mm) using a double-sided adhesive (ARcare 90445Q) to fit the NTDscope carriage. In each of the three glass slides prepared, there were two glass capillaries containing two reactions (Positive and NTC). We used the fluorescence imaging capabilities of the NTDscope to image each glass slide every 10 minutes for 60 minutes after equilibration to the assay temperature of 37^°^C. Fluorescence signal was quantified using ImageJ Fiji by taking an average of pixel intensity of a fixed pixel area across all images in the time series for the positive and the NTC reactions. A plot of the fluorescent signal over time was generated using the measured pixel intensities (Fig 5B.i.). Slopes of the curves were calculated by performing simple linear regression of the data for each replicate (Fig 5B.ii.). Slopes of the positive samples were compared to the NTC using an unpaired t-test.
We compared the assays run on the NTDscope to a conventional plate reader. To make the plate reader measurements, 15 μL reactions were loaded into individual wells from a 384-well plate and incubated in a plate reader (TECAN, Spark) for 60 minutes at 37^°^C, with fluorescence intensity measurements taken every 2.5 minutes ( : 425 nm; : 500 nm). The slope of the reactions starting at 10 minutes (to account for assay temperature equilibration) was calculated by linear regression of the mean background-subtracted reaction rate (RFU/sec) with SEM. All data were compared using an unpaired t-test.
Results
Quantification of live microfilariae in blood samples
The NTDscope can be used to capture videos of moving samples, such as microfilariae (mf) of Loa loa and other filarial parasites. The videos can be processed to detect live parasites without the need for staining or additional sample preparation, allowing for point-of-care diagnosis and quick time-to-result. We demonstrate this by using the original rectangular capillaries to acquire videos of microfilariae in blood and plasma, as shown in Fig 2.
NTDscope for live imaging of microfilariae in blood and plasma samples.A: Time series showing the movement of a Brugia malayi microfilaria in plasma of an infected cat. B: (top) image of a capillary filled with peripheral blood of a human patient infected with Loa loa, collected and imaged in Cameroon, (middle) screenshots of the videos corresponding to the 7 FOVs imaged for the capillary, (bottom) difference images generated from the 7 videos. The patient had calibrated thick smear counts of 4,001 mf/ml. A video of the middle (highlighted) FOV is shown in S1 Video. C: Difference images generated from videos from four different patients in Cameroon, three of whom were infected with Loa loa mf (thick smear counts 115-1,047 mf/ml) and one patient who was negative for Loa loa. D: Sensitivity and specificity of manual identification of microfilariae on videos of patient peripheral blood acquired on the NTDscope in Gabon, compared to the presence of microfilariae of Loa loa and Mansonella perstans in calibrated thick smears. E: Snapshots of videos and corresponding difference images of samples containing M. perstans (top) and B. malayi (bottom) mf. The mf identified in videos and difference images are circled in green. Data was processed and visualized using GraphPad Prism 10.
The total imaging and processing time for diagnosis is less than 3 minutes. Fig 2B shows a picture of one capillary filled with blood from a Loa loa-positive patient in Cameroon, followed below by screenshots of the 7 videos acquired (blood images), and showing the capillary regions that the FOVs correspond to. A video of one of these FOVs is shown in S1 Video. Difference images generated by processing patient sample videos show regions of high intensity in locations of the FOV where there was movement, in this case due to the presence of microfilariae in the sample. The bottom row of Fig 2B shows representative difference images, with corresponding calibrated thick smear counts of 4,001 mf/ml. The higher number of high intensity regions in difference images corresponds to higher Loa loa mf concentration in patient samples. This is demonstrated in Fig 2C, where the difference image corresponding to one FOV of four different patients is shown. The corresponding thick smear counts for those patients (ranging from 0-1,047 mf/ml) are shown below each image.
We used patient sample videos collected in Gabon to compare the performance of manual counts of microfilariae in videos acquired on the NTDscope to microfilariae detection in calibrated thick smears. Sensitivity and specificity of the NTDscope were 87% and 85%, respectively, compared to gold standard thick smear counts (Fig 2D). If false negatives, defined as videos where microfilaria are observed but the thick smear count was zero, are excluded, the specificity of the NTDscope is 99.2%.
We used blood and plasma samples of cats infected with live Brugia malayi microfilariae (provided by the Filariasis Research Reagent Resource Center for distribution through BEI Resources, NIAID, NIH). Snapshots of a video of plasma are shown in Fig 2A, and the full video can be found in S2 Video. We compared manual counts of microfilariae in cat blood videos to visible microfilariae in calibrated thick smears. The thick smear and manual capillary counts are shown in S1 Fig. There is a decrease in the manual capillary counts compared to the thick smears, which was also seen in [46].
Different filarial species have distinct movement signatures, which can be seen by examining difference images from samples with mf of different species. Fig 2E shows a difference image of a sample of a human patient infected with M. perstans, collected in Gabon, and a difference image of a blood sample of a cat infected with B. malayi. The intensity peaks corresponding to the location of mf movement in the FOVs are marked by green circles. The peaks are smaller for M. perstans when compared to those produced by B. malayi and even Loa loa (seen in Fig 2B and C).
Multi-contrast imaging of helminth eggs
The NTDscope can be used to image parasite eggs in urine and stool samples with minimal processing. For imaging of Schistosoma haematobium eggs in patient urine samples, we used a tapered capillary described in [32] and shown in Fig 3A. A study on the detection of S. haematobium using the NTDscope was performed in Côte d’Ivoire in January of 2024 [56]. Fig 3A shows a representative image collected in this study, showing S. haematobium eggs in patient urine samples that were imaged using brightfield and darkfield illumination on the NTDscope. When comparing manual counts of Schistosoma eggs in images acquired on the NTDscope to gold standard microscopy, the sensitivity ranged from 94-100% and the specificity ranged from 59.1-72% [56].
The NTDscope can image parasitic eggs in urine and stool.A: Images of Schistosoma haematobium eggs from a urine sample of a patient in Côte d’Ivoire, acquired using brightfield (BF) and darkfield (DF) imaging. B: Image of soil-transmitted helminth (STH) eggs from a patient stool sample processed using a flotation-based assay and imaged using the NTDscope in Cameroon. Insets showing Trichuris trichiura (left) and Ascaris lumbricoides (right) eggs captured in different locations of the NTDscope tapered capillary. C: (top) images of A. lumbricoides eggs from a patient stool sample, processed with a flotation solution and imaged using BF and DF illumination on the NTDscope in Bangladesh. (bottom) Schistosoma japonicum and Schistosoma mansoni eggs isolated from hamster livers and imaged on the NTDscope using BF and DF illumination. All patient samples were confirmed as positive via gold standard microscopy.
The NTDscope can also be used to image soil-transmitted helminth (STH) eggs found in patient stool samples. We used the mini-FLOTAC technique and tapered capillaries to process stool samples for imaging on the NTDscope. As seen on the image in Fig 3B, the bigger Ascaris lumbricoides eggs (45-75 μm thick) were concentrated on the right side of the image, corresponding to the region of the capillary closest to the inlet, while the smaller Trichuris trichiura eggs (20-25 μm thick) were concentrated on the left side, closest to the capillary outlet hole.
We also explored an alternative method for stool sample processing using the Fecalyzer, a device that is similar to the Fill-FLOTAC but simpler, cheaper, and more commonly used for veterinary applications [59]. Fig 3C (top) shows A. lumbricoides eggs from stool samples of patients that were confirmed STH-positive via standard microscopy. These samples were collected and processed as described above, in an STH-endemic area in Bangladesh.
Lastly, we show that the NTDscope can be used to image Schistosoma eggs of different species, including S. japonicum and S. mansoni. Using viable schistosoma eggs extracted from livers of infected hamsters (provided by the Schistosomiasis Resource Center of the Biomedical Research Institute (Rockville, MD)), we observed that the NTDscope resolution is sufficient for the eggs of different species to be differentiated by eye on the NTDscope images (as shown in Fig 3C (bottom)). We also acquired videos of S. mansoni miracidia hatched from liver-extracted eggs in brightfield and darkfield illumination, one of which is shown in S3 Video.
Imaging of stained patient samples
We explored the use of the NTDscope for imaging of fixed and stained slides, which could be useful in clinical laboratory settings where fixing and staining of samples is routine. We imaged a custom capillary with a thick smear prepared using cat blood infected with B. malayi (Fig 4A). Given the large field of view of the NTDscope, only seven images were required to cover the entire sample. The stitched images are shown in Fig 4A. The NTDscope could resolve the B. malayi microfilariae well, and this is another demonstration of how the NTDscope can be adapted for other relevant assays.
The NTDscope can image parasites on fixed and stained slides.A: (Top left) picture of a thick smear capillary designed to be imaged with the NTDscope, including 30μL of blood from a cat infected with Brugia malayi. (Middle left) Thick smear capillary after Giemsa staining. (Bottom) stitched images of Giemsa-stained capillary, collected with the NTDscope, with an inset showing six B. malayi microfilariae (top right). B: Images of fixed and stained slides with parasites, collected on the NTDscope, showing (left) Entamoeba histolytica, (middle) Trichomonas vaginalis, and (right) Leishmania donovani promastigotes.
To explore whether the NTDscope could be used for imaging other relevant parasites, we modified a device slightly such that it could fit standard microscope slides and imaged fixed and stained slides sourced from Carolina Biological. We imaged Entamoeba histolytica, Trichomonas vaginalis, and Leishmania donovani promastigotes. The L. donovani promastigotes were too small (1-2μm) to fully resolve with the NTDscope.
Imaging of lateral flow assays
We next used the NTDscope to quantify lateral flow assays (LFA) of commercially-available SARS-CoV-2 tests. Fig 5A.i. includes a time-lapse of the test band for the positive patient, showing how the intensity of the band increases in time (as shown by a decrease in pixel intensity, Fig 5A.ii.). We also show the control and test bands for two positive samples and one negative sample (Fig 5A iii.) and a scan of the entire strip showing the control and test band for a positive patient.
The NTDscope can be used to image lateral flow test strips and CRISPR-Cas molecular assays.A: Lateral flow assays imaged on the NTDscope. A.i. Time series (15 min) of the test line on a COVID-19 antigen test, tested on a positive patient. A.ii. Measurement of the dye intensity over time, of the test line shown in A.i., calculated by dividing the mean pixel intensity of a rectangular region of interest (ROI) over the test line by an ROI outside of the test line. Pixel intensity was measured using Fiji (ImageJ). A.iii. End-point images after 15 minutes for three COVID-19 tests (2 positive, 1 negative), showing the test and control lines. A.iv. Scan of the entire COVID-19 test strip, showing the control and test bands for a positive patient after 15 minutes. B: Results of a CRISPR-Cas13 assay run on NTDscope. B.i. Measurement of fluorescence intensity over time for a Cas13 assay with a guide RNA specific to SARS-CoV-2, in the presence (SARS-CoV-2 1e6 copies/μL) and absence (non-target control — NTC) of synthetic SARS-CoV-2 RNA. Fluorescence intensity was measured during the first 60 minutes of assay time; measurements were acquired every 10 minutes. The data from the first 10 minutes was discarded to allow assay components to equilibrate to temperature. Experiment performed in triplicate. B.ii. Slopes of the curves calculated by performing simple linear regression of the data for each replicate of B.i., slopes of the positive samples were compared to the no target RNA controls (NTC) using an unpaired t-test. * is p≤0.05. Data were processed and visualized using GraphPad Prism 10.
Imaging a CRISPR-Cas assay
Detection of RNA or DNA with CRISPR is a promising approach for diagnosis of infectious diseases [61]. To demonstrate the ability of the NTDscope to detect a CRISPR reaction, we leveraged the device’s fluorescence capabilities to image a CRISPR-Cas13a assay for the detection of SARS-CoV-2 (Fig 5B). The slope of the fluorescence increase for the positive sample measured on the NTDscope was significantly larger than the slope of the non-target control, confirming SARS-CoV-2 RNA detection by Cas13a. Additionally, the slope of the line for cp/μL produces similar results to slopes seen when the assay was run on a temperature-controlled plate reader (S2 Fig).
Discussion
In this work, we presented the design of the NTDscope, a portable, multi-contrast microscope that enables diagnosis of neglected tropical diseases at the point-of-care. We demonstrated its imaging capabilities for microfilariae in peripheral blood, Schistosoma eggs in urine samples, and STH eggs in processed stool samples. We also showed that the device is capable of reading molecular assays by imaging both lateral flow assays and fluorescence-based CRISPR-Cas assays. Sample preparation is simplified for these applications by the use of disposable plastic capillaries, including rectangular straight channel capillaries for defined blood volumes, tapered capillaries for filtering eggs from urine and floated stool samples, as well as a prototype capillary for thick blood smears that is compatible with the NTDscope.
Using data acquired in field settings in Gabon, we showed that manual counting of microfilariae in videos acquired on the NTDscope is sensitive and specific when compared to calibrated thick smears, the gold standard technique. Interestingly, we could see movement consistent with the presence of microfilariae in the NTDscope videos for 20 patients who were found to be thick smear negative for microfilariae. The majority of these videos have less than a total of 10 visible microfilariae. This suggests that the NTDscope may be a particularly useful tool for patients with low intensity infections, potentially out-performing the current gold standard.
We used cat blood samples infected with Brugia malayi microfilariae to explore the relationship between thick smear counts and NTDscope counts of microfilariae. There was an observed decrease in manual counts compared to thick smears. This could be due to a fraction of dead mf that are counted in the thick smears but are not captured in difference images, or due to live mf that do not enter into the capillaries. We also observed differences in the red blood cell displacement of samples with Brugia malayi microfilariae, Loa Loa, and M. perstans. Smaller intensity peaks seen on difference images generated from videos with M. perstans implies that M. perstans microfilariae consistently create much smaller areas of blood displacement as compared to Loa loa and B. malayi. These signatures could eventually be used to distinguish between filarial species. Additionally, the NTDscope could be suitable for veterinary diagnostic applications, as evidenced by our ability to detect live B. malayi microfilariae in blood samples of infected cats.
As new diagnostic applications are developed for the NTDscope, new capillary designs that fit the carriage dimensions and focal plane can be designed. The original straight channel capillary was designed to easily load a peripheral blood sample for quantification of microfilariae, but it can also be loaded with other liquids for other uses. Previous applications have included imaging of parasitic eggs isolated from a flotation solution using the Fill-FLOTAC or Fecalyzer devices, as well as imaging of diatoms in marine samples for educational purposes. The tapered capillary that was designed to isolate Schistosoma eggs from urine has also proven useful for other applications that require size-exclusive filtering and concentration, such as separating two different species of STH eggs. STH is traditionally detected using the Kato-Katz method, a time-consuming technique that involves sieving, staining and smearing a stool sample onto a glass slide for imaging using a microscope [57]. In addition to decreasing cost, sample preparation steps, and required materials for STH detection, this is an example of how new assays and sample processing techniques can be easily adapted for imaging on the NTDscope.
The prototype thick smear capillary demonstrates potential for integrating common clinical laboratory assays into the device, including wet mounts for protozoa and fungi, three-part blood counts, and parasitic egg viability assays [63,64]. Some samples were not fully resolveable; computational imaging techniques have the potential to improve the resolution of the NTDscope such that these and other parasites (e.g., malaria) can also be imaged on the device [60]. The ability to capture images of live parasites has the potential to provide new information about infections and response to treatment. For example, NTDscope videos of Loa loa microfilariae motion inherently capture only live parasites rather than dead microfilariae that could appear in conventional thick smear microscopy. In the case of low parasitemia, additional FOVs and multiple capillaries from a single patient can be analyzed, which could improve sensitivity for treatment stopping decisions in near-elimination settings.
The diagnostic power of the NTDscope is enhanced by integrating machine learning (ML) for automated analysis of patient samples. Importantly, the use of ML can significantly reduce the time required for sample analysis, including manual counting of parasites that can take a minimum of 10 minutes per slide for well-seasoned technicians [65] and can have high variability [66,67], reducing fatigue as well as increasing throughput. Automated parasite detection could also potentially allow for the examination of greater patient sample volumes, which would reduce the Poisson variability in disease elimination settings by increasing the sample size [68]. Use of the Android OS environment allows existing ML models designed for mobile applications to be easily run on the device. Furthermore, the portability of the NTDscope simplifies data collection for NTDs, increasing the amount of available training data for ML models, which is particularly important for capturing patient samples in NTD-endemic regions where microscopes with digital cameras are unavailable. Beyond classification of parasites in static images, ML models have the potential to differentiate microfilarial species based on movement signatures, which we have observed to be different for M. perstans, B. malayi, and Loa loa microfilariae (Fig 2). As more field data is collected, ML algorithms could be developed to distinguish between multiple filarial species. For some diagnostic uses cases, visualizing an ML-highlighted parasite on the screen of the NTDscope could help to build confidence in the tool for both providers and patients.
The multi-contrast imaging capabilities of the NTDScope could prove useful for future diagnostic applications that involve species differentiation, such as for distinguishing soil transmitted helminth species and S. mansoni eggs in stool samples. Darkfield imaging has proved beneficial when used for ML-based identification of S. haematobium eggs, where models trained on darkfield images performed better than those trained on brightfield images [34]. Darkfield illumination is particularly helpful when distinguishing eggs from other debris found in samples, which is typically achieved through staining, which requires extra steps and assay components. Given that many parasitic eggs and worms exhibit autofluorescence [69–72], the NTDscope could further facilitate speciation with its fluorescence capabilities.
The fluorescence capabilities of the NTDscope provide the potential to replace bulky laboratory equipment, such as plate readers for molecular assays. Fluorescence-based molecular assays, such as those based on CRISPR-Cas enzymes, are of growing interest for infectious disease diagnosis as they avoid the need for conventional PCR machines and temperature cycling (amplification-free CRISPR-Cas reactions are isothermal). CRISPR-Cas diagnostic assays have been demonstrated for the detection of neglected diseases including Schistosomiasis [73,74], Trypanosomiasis [75], Leishmaniasis [76], Malaria, [77], Zika, Dengue [78], and others [79–81]. These reactions can be read using portable devices [62,82], and could be adapted to be read using the NTDscope. We also showed that the NTDscope can be used to read the results of lateral flow assays. While multiple portable LFA readers exist [83–88], the potential to read test strips with a magnified imaging system could improve sensitivity in cases of light infection, help digitize results for future use, and open the possibility of combining multiple tests onto a single test strip, reducing the quantity of reagents needed [89–94]. The requirements for reagents and temperature control for many molecular assays are such that they tend to be more expensive than microscopy-based methods. However, for particular applications such as parasite speciation and resistance, or in disease elimination settings, the high sensitivity and specificity of molecular assays make them uniquely useful.
Presently, the main limitation of the NTDscope lies in device availability. The NTDscope presented here is a prototype built to demonstrate the feasibility of a fully-integrated diagnostic device for multiple NTDs, and 80 devices were built in a limited manufacturing run. Collaborators in Cameroon, Gabon, Côte d’Ivoire, and Bangladesh continue to work with the device to establish efficient workflows for expanded use, as well as explore additional diagnostic and disease mapping applications. With additional feedback from ongoing field work, future versions of the device have the potential to be manufactured or assembled in the countries where they are used. The NTDscope represents an important step toward increasing access to disease testing in regions with limited healthcare infrastructure through portable diagnostic technology, a direction that may also benefit regions beyond those with NTDs.
Conclusion
The NTDscope is a portable, multi-contrast microscope designed to diagnose neglected tropical diseases at the point-of-care. It features high-resolution imaging at a low cost, achieved by taking advantage of high-quality, mass-produced consumer electronic parts, such as mobile phone lenses. The device is compact, user-friendly, and does not require mains electricity to run. Here, we demonstrate use of the NTDscope for a diverse set of assays and samples in laboratory and field settings including Cameroon, Gabon, Bangladesh, and Côte d’Ivoire. When combined with machine learning for automated diagnostics, the NTDscope has the potential to increase the reach and impact of healthcare professionals. The portability of the NTDscope can also increase the amount of image data collected from patients with NTDs, a necessary step for training of machine learning models that has been difficult to achieve in NTD-endemic regions. We envision the NTDscope as a platform technology that addresses diagnostic needs for multiple NTDs and supports ambitious disease control and elimination programs.
Supporting information
S1 FigComparison of manual counts of microfilarial movement in videos to counts of Brugia malayi microfilariae in calibrated thick smears.Comparison of B. malayi microfilariae counted manually from videos acquired on the NTDscope and microfilariae counts in calibrated thick smears, from a blood sample of a cat infected with B. malayi.(TIFF)
S2 FigCRISPR-Cas13a assay results on plate reader.i. Measurement of fluorescence intensity over time for a Cas13 assay with a guide RNA specific to SARS-CoV-2, in the presence (SARS-CoV-2 1e6 copies/μL) and absence (non-target control — NTC) of synthetic SARS-CoV-2 RNA. Fluorescence intensity was measured on a Tecan Spark plate reader during the first 60 minutes of assay time; measurements were acquired every 10 minutes. The data from the first 10 minutes was discarded to allow the assay components to equilibrate to temperature. Experiment performed in triplicate. ii. Slopes of the curves were calculated by performing simple linear regression of the data for each replicate of i. Slopes of the positive samples were compared to the no target RNA controls (NTC) using an unpaired t-test. Data are expressed as mean ± standard error of the mean (SE). is p < 0.05; ^^ is p < 0.01; ^^ is p < 0.001; ^***^ is p < 0.0001. Data was processed and visualized using GraphPad Prism 10.(TIFF)
S1 VideoLoa loa microfilariae in peripheral blood.Video showing a field-of-view (FOV) of a capillary filled with peripheral blood of a human patient infected with Loa loa, collected and imaged in Cameroon. This corresponds to the fourth FOV from left to right in Fig 2B. The patient had calibrated thick smear counts of 4,001 mf/ml.(MP4)
S2 VideoBrugia malayi microfilariae in plasma.Video showing multiple B. malayi microfilariae in plasma of an infected cat.(MP4)
S3 VideoS. mansoni miracidia.Video showing S. mansoni miracidia hatched from eggs extracted from livers of infected hamsters. The sample was imaged under brightfield and darkfield illumination.(MP4)
S1 ChecklistInclusivity in global research checklist.(PDF)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization. Ending the neglect to attain the Sustainable Development Goals: A road map for neglected tropical diseases 2021 –2030; 2020. https://www.who.int/publications/i/item/9789240010352
- 2World Health Organization. Global report on neglected tropical diseases 2023 ; 2023. https://www.who.int/publications/i/item/9789240067295
- 3Amoah AS, Hoekstra PT, Casacuberta-Partal M, Coffeng LE, Corstjens PLAM, Greco B, et al. Sensitive diagnostic tools and targeted drug administration strategies are needed to eliminate schistosomiasis. Lancet Infect Dis. 2020;20(7):e 165–72. doi: 10.1016/S 1473-3099(20)30254-1 32595046 · doi ↗ · pubmed ↗
- 4Siqueira LMV, Couto FFB, Taboada D, Oliveira ÁAde, Carneiro NF de F, Oliveira E, et al. Performance of POC-CCA® in diagnosis of schistosomiasis mansoni in individuals with low parasite burden. Rev Soc Bras Med Trop. 2016;49(3):341–7. doi: 10.1590/0037-8682-0070-2016 27384831 · doi ↗ · pubmed ↗
- 5Casacuberta M, Kinunghi S, Vennervald BJ, Olsen A. Evaluation and optimization of the Circulating Cathodic Antigen (POC-CCA) cassette test for detecting Schistosoma mansoni infection by using image analysis in school children in Mwanza Region, Tanzania. Parasite Epidemiol Control. 2016;1(2):105–15. doi: 10.1016/j.parepi.2016.04.002 27430027 PMC 4946158 · doi ↗ · pubmed ↗
- 6Yunus MH, Arifin N, Balachandra D, Anuar NS, Noordin R. Lateral flow dipstick test for serodiagnosis of strongyloidiasis. Am J Trop Med Hyg. 2019;101(2):432–5. doi: 10.4269/ajtmh.19-0053 31218996 PMC 6685572 · doi ↗ · pubmed ↗
- 7Watts MR, James G, Sultana Y, Ginn AN, Outhred AC, Kong F, et al. A loop-mediated isothermal amplification (LAMP) assay for Strongyloides stercoralis in stool that uses a visual detection method with SYTO-82 fluorescent dye. Am J Trop Med Hyg. 2014;90(2):306–11. doi: 10.4269/ajtmh.13-0583 24323513 PMC 3919238 · doi ↗ · pubmed ↗
- 8Rashwan N, Diawara A, Scott ME, Prichard RK. Isothermal diagnostic assays for the detection of soil-transmitted helminths based on the Smart Amp 2 method. Parasit Vectors. 2017;10(1):496. doi: 10.1186/s 13071-017-2420-1 29047387 PMC 5648480 · doi ↗ · pubmed ↗