Nationwide epidemiological study of tuberculosis and other respiratory pathogens among children and adolescents in Brazil: TBPed Brazil study protocol
Marcelo Comerlato Scotta, Márcia Polese-Bonatto, Fernanda Hammes Varela, Ivaine Tais Sauthier Sartor, Gabriela Oliveira Zavaglia, Caroline Nespolo de David, Ingrid Rodrigues Fernandes, Thais Raupp Azevedo, Annerose Barros, Anna Cristina C. Carvalho

TL;DR
This study aims to better understand and diagnose tuberculosis in children and adolescents in Brazil using new testing methods.
Contribution
This is the first nationwide prospective study on tuberculosis in children and adolescents in Brazil, evaluating diagnostic accuracy and prevalence.
Findings
Xpert MTB/RIF Ultra in induced sputum samples is being evaluated for diagnosing pulmonary tuberculosis in children.
The study will assess the prevalence of tuberculosis infection and associated risk factors in children and adolescents.
The accuracy of Brazil's national scoring system for diagnosing pulmonary tuberculosis will be evaluated.
Abstract
The burden of lower respiratory tract infections (LRTIs) caused by Mycobacterium tuberculosis (MTB) among children and adolescents is often underestimated due to challenges in obtaining lower respiratory tract samples, nonspecific signs and symptoms, the paucibacillary nature of tuberculosis (TB), and the low yield of microbiological tests. Xpert MTB/RIF Ultra in induced sputum (IS) samples is the most promising test for improving microbiologic diagnosis of pulmonary tuberculosis (PTB) in young children. We describe the TBPed Brazil study, a multicenter, cross-sectional study in participants aged 6 months to 15 years. We designed a two-arm study: a hospital-based arm with patients hospitalized with LRTI and an outpatient-based arm with children and adolescents referred to TB-specialized clinics. The main aim in the hospital-based arm is to determine the prevalence of PTB. In the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
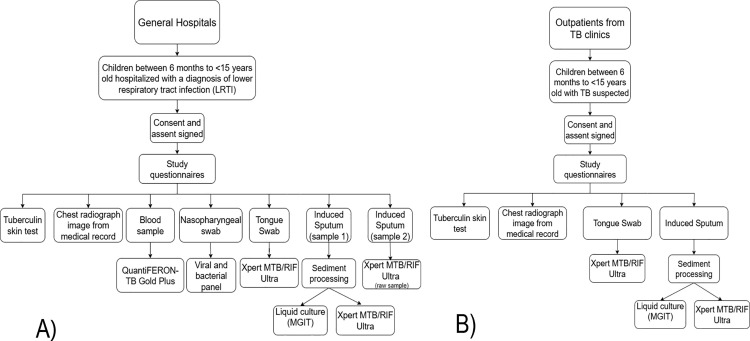 Fig 1
Fig 1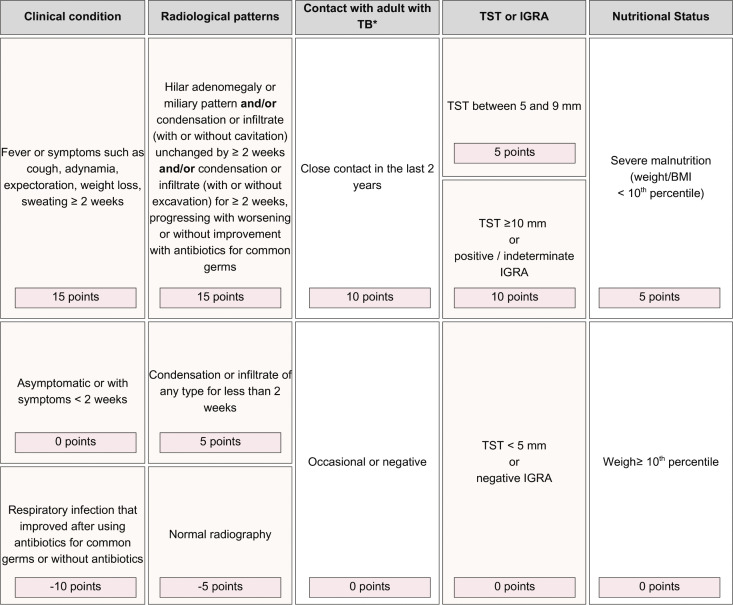 Fig 2
Fig 2- —Hospital Moinhos de Vento, supported by the Ministry of Health of Brazil, funds this study through the Program for Supporting the Institutional Development of the Public Health System (PROADI-SUS). So
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTuberculosis Research and Epidemiology · Pneumonia and Respiratory Infections · Respiratory viral infections research
Introduction
The burden of lower respiratory tract infections (LRTIs) due to Mycobacterium tuberculosis (MTB) among children and adolescents is usually underestimated, particularly in children under five years of age. In addition to the challenges of obtaining lower respiratory tract samples, nonspecific signs and symptoms, paucibacillary disease, and the low yield of microbiological testing contribute to its underdiagnosis and under-notification [1]. Most diagnoses of pulmonary tuberculosis (PTB) among children are presumptive, usually based on clinical and radiological prediction scores [2,3].
However, significant progress has been made in improving the microbiological diagnosis of PTB in children. The introduction of new molecular tests in clinical practice, such as Xpert МТB/RIF, has improved MTB detection in children [4]. Moreover, the development of a more sensitive Xpert MTB/RIF, i.e., the Ultra assay, which offers a 1–log improvement in the lower limit of detection, has increased diagnostic sensitivity across different clinical samples, such as nasopharyngeal, sputum, and stool [5–7]. Xpert MTB/RIF Ultra (Ultra) in induced sputum (IS) samples is the most promising for improving the diagnosis of PTB. In a large South African study, the sensitivity and specificity of the Ultra assay were 74.3% and 96.3%, respectively, when compared to liquid culture in a single IS sample. Two samples, IS and a nasopharyngeal aspirate, increased the sensitivity to 80% [8].
However, most studies originate from either low-income countries, particularly in Africa and Asia, or high-income countries [9–12]. In Brazil, one of the largest middle-income countries globally, tuberculosis (TB) has an overall intermediate incidence of 39.7 cases per 100,000 population in 2024 [13,14], which is high compared to high-income nations, but different from other lower and middle-income countries.
Current studies on PTB in Brazilian children and adolescents are based on retrospective data and do not evaluate the broader nationwide diversity [15,16]. The Brazilian Tuberculosis Pediatric (TBPed) study was planned on the assumption that PTB prevalence in children and young adolescents under 15 with LRTI would be between 2% and 3% and power calculations were based on these figures. Following the COVID-19 pandemic, new data suggest an increase in TB prevalence, due to poor treatment adherence (especially among adult patients), and higher rates of intra-domiciliary transmission [17–19].
The protocol includes children and young adolescents and was designed as a two-arm study in different settings. The first group consists of hospitalized participants with a diagnosis of LRTI, without necessarily a history or clinical signs and symptoms suggestive of TB. The second group consists of participants referred to TB-specialized clinics within the Brazilian public service TB network, to investigate and initiate treatment if the diagnosis is established.
The main aim of the hospital-based arm is to determine the prevalence of PTB among children and adolescents with LRTI. In the outpatient-based arm, the main objective is to evaluate Ultra’s accuracy in induced sputum samples compared to automated liquid culture. We assess in both study arms: tuberculosis infection (TBI) prevalence; the accuracy of Ultra in tongue swabs compared to sputum samples in Ultra and automated liquid culture; risk factors associated with PTB and TBI; accuracy of the Brazilian Ministry of Health scoring system for the diagnosis of PTB [20]. In the hospital-based arm, we also evaluate the prevalence of viral and/or bacterial pathogens associated with LRTI and describe the severity of hospitalized participants with LRTI without PTB.
Methods
Study design and setting
TBPed Brazil is a multicenter, cross-sectional study with prospective data collection. The study includes 27 sites in four of the five Brazilian regions (North, Northeast, Southeast, and South), in cities with a general incidence of TB higher than 50 cases per 100,000 population, or in TB clinics that serve as referral centers for TB patient care in the region. We excluded the Central-West region due to its lower TB incidence [21]. Enrollment began in December 2021 and is expected to be concluded in July 2026.
The study includes two different settings. In pediatric general hospitals, individuals hospitalized due to LRTI are eligible for enrollment. In outpatient referral TB clinics, individuals referred for PTB investigation are also eligible for enrollment.
Eligibility
Hospital-based study arm
Inclusion criteria.
Patients aged from 6 months to less than 15 years are eligible if admitted for less than 7 days, have a chest radiograph performed during the current admission, and present at least one of the following signs at enrollment:
age-specific tachypnea (6 months to 1 year: 50 breaths per minute, 1–4 years: 40 breaths per minute; 5–14 years: 30 breaths per minute) or respiratory retractions and/or;lower respiratory signs of wheezing, crackling, or diminished breath sounds and/or;danger signs of severe pneumonia according to World Health Organization guidelines [22] and/or;radiographic signs suggestive of intrathoracic TB (tracheal compression and/or displacement; soft tissue opacity suggestive of adenomegaly; alveolar opacity; nodular infiltrate suggestive of miliary TB; cavitation; calcification of the lung parenchyma; or pleural effusion [23].
Exclusion criteria.
Participants are excluded if not living in Brazil, if previously treated or on treatment for any form of TB disease for at least 72 hours, have a previous diagnosis of cystic fibrosis or bronchiolitis obliterans, a tracheostomy, clinically diagnosed at enrollment with a healthcare-associated infection, asthma exacerbation without associated LRTI, or being on invasive or non-invasive mechanical ventilation. After inclusion, the participant is excluded if a sputum sample cannot be obtained.
Outpatient-based study arm
Inclusion criteria.
Participants aged 6 months to 15 years at TB referral clinics are eligible if they have one of the following:
persistent, unremitting cough for more than two weeks and/or;unexplained axillary temperature above 37.8 °C for more than one week and/or;persistent, unexplained lethargy and/or;decrease in playfulness/activity reported by the parent/caregiver and/or;weight loss/failure to thrive (weight loss is defined as >5% reduction in weight compared with the highest weight recorded in the last three months, and failure to thrive is defined as clear deviation from a previous growth trajectory), and/or documented crossing percentile lines in the preceding 3 months, and/or weight-for-age z score of ≤ −2 in the absence of information on previous/recent growth trajectory, and/or weight-for-height z score of ≤ −2 in the absence of information on previous/recent growth trajectory and not responding to nutritional rehabilitation (or antiretroviral therapy if HIV infected).
Exclusion criteria.
Participants are excluded if previously treated or on treatment for any form of TB disease for at least 72 hours, have a tracheostomy, or have a known impediment to collecting respiratory samples. After inclusion, the participant is excluded if a sputum sample cannot be obtained.
Participant selection and study variables
On weekdays, a convenience sample is screened in both pediatric wards and outpatient clinics, based on the eligibility of potential participants. Potential participants’ legal caregivers are invited to be included. Study invitation and data collection is done by the research teams of the participating sites. To ensure consistency in all study procedures, the coordinating team trained all investigators and researchers involved in the study according to the Operational Manual, which contains the study’s standard operating procedures (SOPs). It required them to produce up-to-date Good Clinical Practice (GCP) certification. Study questionnaires are administered to the patient’s legal caregiver. Data collected in the TBPed Study are shown in Table 1. Fig 1 presents the study procedures performed in the hospital-based study arm (panel A) and in the outpatient-based study arm (panel B). Our study is cross-sectional; however, we conducted a small follow-up through medical record review to verify TB diagnoses and treatments administered after study entry. This medical record review is conducted for hospitalized participants at the time of hospital discharge or within 28 days of admission, whichever occurs first. Medical record review for outpatient participants occurs up to 60 days after study entry, the maximal time required for the release of liquid culture results.
Table 1: Data collected in the TBPed study.
Study procedures performed in the hospital-based study arm (panel A) and in the outpatient-based study arm (panel B).MGIT = Mycobacteria Growth Indicator Tube.
Chest radiograph (CXR)
The CXR image is obtained from the participant’s medical record, as requested by the attending physicians. All researchers are trained in the Standardized Operational Procedure (SOP) for chest radiograph acquisition and storage in the study electronic case report form. The assessment of intrathoracic TB and pneumonia in children will be evaluated by consensus of two expert radiologists blinded to the clinical data, with a third reader available to resolve discordant decisions using a standardized reporting form. The criteria for radiological classification are described elsewhere [20,23–25].
The Brazilian Ministry of Health’s score
The Brazilian Ministry of Health’s validated score [2,3] system for predicting PTB in children and adolescents, updated in 2022 [26], includes signs and symptoms, radiological findings, contact with adults with PTB, TST results, and nutritional status, as shown in Fig 2 and described elsewhere [3]. Diagnosis probability is classified as follows: at least 40 points = very likely diagnosis, 30–35 points = possible diagnosis, and 25 points or less = diagnosis is unlikely. The same score will be calculated using IGRA results instead of TST results when IGRA is available.
The Brazilian Ministry of Health’s score system for predicting PTB in children. RMT = rapid molecular test; TB = tuberculosis; TST = tuberculin skin test, IGRA = Interferon-Gamma Release Assay, BMI = Body Mass Index. More than or equal 40 points (very likely diagnosis) = it is recommended to start TB treatment; 30–35 points (possible diagnosis) = indicative of TB; it is advised to initiate treatment, at medical discretion; Less than or equal 25 points (diagnosis is unlikely) = investigation of the child should be continued.
TB-related diagnostic criteria
Pulmonary tuberculosis (PTB):
- Pulmonary tuberculosis confirmed: detection of MTB by liquid culture or by molecular biology tests;
- Pulmonary tuberculosis - clinical diagnosis: TB clinical diagnosis by the attending physician without microbiological confirmation of MTB, adjudicated by the Brazilian Ministry of Health’s validated score system mentioned above, considering the diagnosis if at least 40 points; Tuberculosis infection (TBI): a TST (≥5 mm) or IGRA positive, and negative microbiological, radiological, and clinical diagnosis (excluding presumptive PTB or other forms of active TB).
Study aims and outcomes
The main aim (primary outcome) in the hospital-based arm is to determine the prevalence of PTB. In the outpatient-based arm, the main aim (primary outcome) is to assess the accuracy of Ultra in IS samples compared to liquid culture. Table 2 describes the study aims and specifies the study arm involved, the statistical analysis plan, the missing data management, and the outcomes for each.
Table 2: Study aims, statistical analysis plan, missing data management, and outcomes.
Specimen collection
Trained research health professionals undertake all the sample collection and laboratory procedures, according to the study’s SOPs. All samples are transported to partner laboratories by a specialized company, in accordance with biosafety standards.
Tongue swab collection
Samples are collected using sterile swabs with an ejectable brush-shaped head convenient for DNA extraction (Whatman OmniSwab – Catalog number WB100035). The tongue swab sample is obtained before the sputum sample is collected. The collection is performed by brushing the swab on the tongue 6–8 times. After collection, the material is transferred to a 2 mL tube containing Tris-EDTA buffer (pH 8.0). The tongue sample is used for the Ultra test.
Nasopharyngeal swab collection
The collection is performed with a flexible rayon swab, carefully introduced along the nasal septum until the nasopharynx is felt. It is rubbed, rotated, and held in the nasopharynx for a few seconds. The swab is removed, and the process is repeated in the other nostril. After collection, the swab is placed into Universal Transport Medium – Room Temperature (UTM-RT Copan) (Catalog number 330C) or saline solution (Catalog number SAL00013 bioBoaVista). After collection, the nasopharyngeal sample is stored at −80°C and analyzed to perform a viral and bacterial panel through qualitative reverse transcription-polymerase chain reaction (RT-PCR) assay.
Induced sputum collection
All researchers involved in the study underwent standardized training in the induced sputum (IS) technique, following the study’s standard operating procedure, to ensure correct execution, participant safety, and site biosafety. As this technique is not widely used in Brazilian health services, such training was necessary to standardize collections and maintain sample quality, enabling researchers to collect specimens from all eligible participants in accordance with the study protocols.
Induced sputum training includes all steps of the technique, such as vital signs, pulse oximetry, and pulmonary auscultation. Then, two jets (100 µg) of Salbutamol with a spacer are administered before nebulization. Five mL of 5% hypertonic saline solution is nebulized for approximately 5 minutes. Nasopharyngeal aspiration (NPA) is performed to obtain secretions in all children aged 5 years or younger. Participants aged 5 years or older may have their samples collected through aspiration or spontaneously after induction. The study protocol does not require a minimum volume of sputum samples. Any volume obtained is sent for analysis. During the NPA procedure, the sputum could become trapped in the extension of the aspiration tube. To maximize sample use, the tube is washed at the end of the procedure by aspirating 3 mL of 0.9% saline solution into the collection bottle. As a standardization measure, the spontaneously expectorated samples are also diluted to 3 mL with 0.9% saline solution before being sent to the laboratory.
When possible, a second sample from hospitalized participants is obtained on the following day or at least 4 hours after the first specimen. A clinical evaluation is performed at the end of the procedure, and the child is monitored for 30 minutes afterward. Possible adverse reactions, such as mild epistaxis, increased coughing, and wheezing responsive to an inhaled bronchodilator, are recorded during or after the procedure. The first induced sputum sample is used for the Xpert MTB/RIF Ultra and liquid culture. The second sample is used only for Ultra among hospitalized participants.
Blood collection
Blood is collected in a 6 mL tube containing lithium or sodium heparin with a minimum volume of 4 mL. The tubes were packed in boxes at temperatures ranging from 17°C to 25°C for transfer to the processing laboratory, with a maximum storage time of 16 hours after collection. The blood samples are used for IGRA testing.
Tuberculin skin test (TST)
A trained professional apply 0.1 mL of PPD-RT-23 (tuberculin purified protein derivative – manufacturer AJ vaccines A/S) subcutaneously to the arm and reads the skin test reaction. After administration, the reaction occurs between 48 hours and 72 hours (maximum 96 hours), and is measured in millimeters (mm) of induration (firm swelling). The test is considered positive if the induration is greater than or equal to 5 mm. Participants who previously tested positive are not tested again.
Laboratory procedures (biological processing)
All sample processing and analysis procedures are conducted in a laboratory with trained technologists using standardized protocols.
Sputum sediment processing
The sputum is stored in a cool box (2°C to 8°C) until it is transported to the laboratory, and the specimens are processed within at least five days of collection. Specimens were measured and decontaminated using either N-acetyl-L-cysteine and sodium hydroxide (final concentration of 1.0%) or BD BBL Mycoprep (Becton, Dickinson and Company, catalog number #240862), in a 1:2 volume ratio. The mixture was incubated at room temperature (20–30°C) for 15 minutes and then neutralized with sterile phosphate-buffered saline (PBS, pH 7.0) to a final volume of 50 mL. After centrifugation at 3000 × g for 15 minutes, the pellets are resuspended in 1.5 mL of PBS buffer and divided for testing with Ultra (Cepheid, Sunnyvale, CA) and automated liquid culture (BACTEC MGIT; Becton Dickinson, Franklin Lakes, NJ, USA).
Sputum and tongue swab processing
The sputum and tongue swabs are maintained in a cold box (2° C to 8° C) until they are delivered to the laboratory, where the samples are handled within five days of collection. After homogenization, 1 mL of the sample is used for testing with Ultra (Cepheid, Sunnyvale, CA). This procedure is performed on the second sputum sample from hospitalized participants.
Liquid culture - Mycobacteria growth indicator tube (MGIT)
A 0.5 mL volume of resuspended sputum pellet is inoculated into an automated liquid culture (BACTEC MGIT; Becton Dickinson, Franklin Lakes, NJ, USA). If positive, the corresponding cultured isolate will undergo phenotypic testing, according to the established routine by the laboratory, confirming the growth of MTB, phenotypic resistance testing is done by automated liquid MGIT culture, BD BACTEC™ MGIT™ 960 Sire kit (Becton, Dickinson and Company, catalog number #245123). Liquid cultures are considered negative after 42 days of incubation without isolation of any Mycobacteria.
Molecular rapid test – Xpert MTB/RIF Ultra – sputum sediment
For sputum sedimented samples, 0.7 mL of the resuspended pellet (previously described in the sputum sediment processing) is added to 1.4 mL of the sample reagent included in the Ultra kit. Then, vortexed for 10 seconds, incubated at room temperature (20–30 °C) for 10 minutes, shaken again for 10 seconds, and incubated for 5 minutes (incubate for another 5 minutes if the sample is not completely liquefied). Two milliliters of the liquefied sample are slowly added to the Ultra cartridge and then inserted into the GeneXpert system to perform the test.
Molecular rapid test – Xpert MTB/RIF Ultra – sputum and tongue swab
One milliliter of sputum or tongue swab is added to 2 mL of the sample reagent included in the Ultra kit. Following 10 seconds in the vortex, the sample is incubated at room temperature (20–30 °C) for 10 minutes, shaken again for 10 seconds, and incubated for 5 minutes (or for another 5 minutes if the sample is not completely liquefied). Two milliliters of the liquefied sample are slowly added to the Ultra cartridge and then inserted into the GeneXpert equipment to perform the test.
Interferon-Gamma release assay – QuantiFERON-TB
Whole blood is collected as described in the blood collection. One milliliter (with a variation of 0.8 to 1.2 mL) is transferred to each QuantiFERON-TB Gold Plus tube kit (Nil, TB1, TB2, and Mitogen). To dissolve the antigens on the inner surface of the tube, homogenization is performed with a flat hand and uniform movements (exactly 10 inversions). The tubes are incubated at 37 °C in a vertical position for 16–24 hours and then centrifuged at 3000 × g for 15 minutes to separate the blood plasma. One hundred microliters of plasma are aliquoted for each tube and subsequently stored in a −80°C freezer until the QuantiFERON-TB Gold Plus ELISA is performed according to the manufacturer’s instructions.
Samples are analyzed in three research laboratories with expertise in the technique: the Immunology Laboratory at Fundação de Medicina Tropical Dr. Heitor Vieira Dourado (Manaus/AM), the Molecular Mycobacteriology Research Laboratory at Federal University of Rio de Janeiro Thoracic Diseases Institute (Rio de Janeiro/RJ), and the PROADI Research Laboratory at Moinhos de Vento Hospital (Porto Alegre/RS).
Viral and bacterial panel
The RNA and DNA from nasopharyngeal swab samples are extracted using MagMax™ Viral/Pathogenic Nucleic Acid Isolation (catalog number A42352 Applied Biosystems) on the KingFisher Duo Prime System platform (ThermoFisher, USA). All samples are quantified using a NanoDrop™ Lite Spectrophotometer (ThermoFisher, Wilmington, Delaware, USA) and diluted to a concentration of between 1.0 and 2.0 ng/µL. The RT-PCR assay is done using Path™ 1-Step RT-qPCR Master Mix, CG (catalog number A15299, Applied Biosystems) and TaqMan™ Microbe Detection Assay (catalog number A50137) in 10 µL total reaction, with 5 µL of RNA. Five microliters (1 x 105 copies/μL) of TaqMan™ Respiratory Tract Microbiota Amplification Control (catalog number A39178) are used for reaction control.
The panel assess the presence of a range of common community-acquired respiratory pathogens: seven bacteria (Bordetella pertussis, Chlamydophila pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, Mycoplasma pneumoniae, Staphylococcus aureus and Streptococcus pneumoniae) and 18 viruses (adenovirus 1 e 2; human bocavirus; human coronavirus types HKU1, 229E, NL63, and OC43; human enterovirus, influenza A virus types H1 and H3; influenza B virus; human metapneumovirus; human parainfluenza virus types 1, 2, and 3; human rhinovirus, respiratory syncytial virus (RSV) types A and B, and SARS-CoV-2 (S, N and ORF1ab genes). The samples are stored in different study sites and are transported to the PROADI Research Laboratory at Hospital Moinhos de Vento for analysis. Samples undergo quality control to verify transport time, temperature (if they remain frozen), tube identification, and volume, and are then stored at −80°C until analysis.
Data collection and management
Standardized case report forms (CRFs) were developed to collect demographic, clinical, and laboratory data. Study’s CRFs are available in ReBEC storage (https://ensaiosclinicos.gov.br/welcome - U1111-1332–7450). Data collection is paper-based, based on interviews and medical reviews. After collection, all study data are entered, stored, and managed using an electronic database on REDCap (Research Electronic Data Capture) software, hosted on a secure server [27]. The data are maintained in a study database on REDCap, and the research team has access to the platform through registration and login.
Blinding procedure
Radiologists are blinded to the clinical data and laboratory results during chest radiograph evaluation.
Sample size
The sample size to assess the prevalence of PTB in children hospitalized due to LRTI was obtained based on a systematic review summarizing the prevalence of TB in children aged less than 5 years hospitalized due to LRTI. The average prevalence reported for laboratory-confirmed TB was 7.5% in settings with an overall yearly incidence usually higher than 90 cases per 100,000 population [28]. Moreover, in a study with the most similar inclusion criteria to this study, the prevalence of laboratory-confirmed TB in 2,439 participants was 7%, and for unconfirmed TB was 17% [29]. As the yearly incidence reported in this study setting (South Africa) was 406 cases per 100,000 and the annual average incidence of the cities included in Brazil was around 70 cases per 100,000, a 3% prevalence of PTB is expected in this study. To determine this prevalence with 1% precision, we estimated a sample size of 1,118 individuals, using a 95% confidence interval (Binomial Exact Confidence Interval). Based on these parameters, we expect to include between 37 and 185 cases of PTB among children with LRTI.
A specific sample size was calculated to address the aim related to accuracy, which required a “boost” in sampling by recruiting outpatient participants treated at reference TB centers, considering 20% of PTB prevalence in children/adolescents referred to investigate TB [30]. Similar studies comparing the accuracy of microbiological methods (Ultra and liquid culture) for MTB diagnosis in children and adults reported sensitivities of 75% and 88%, respectively, using Ultra [5,31]. Thus, assuming a sensitivity of 85% and a precision of 0.05, a sample of 226 participants with PTB, confirmed or presumptive, is necessary. Considering a minimum of 37 hospitalized participants, an additional 189 participants are needed. To detect 189 participants who underwent induced sputum collection (nebulization with hypertonic saline solution) with a diagnosis of PTB at outpatient reference TB centers, it is estimated that the screening of 548 participants with signs, symptoms, or radiological exams will meet the inclusion criteria. Considering a loss rate of up to 20% among outpatients, the number of screened participants in this scenario should be 730. It is important to highlight that if the number of hospitalized participants with PTB exceeds 37, fewer outpatients are required if the total number of participants with PTB reaches 226. In summary, the total number of subjects expected for the study (hospitalized and outpatient), considering induced sputum collection, is 1,848 individuals (1,118 hospitalized with LRTI + 730 outpatients).
Statistical analysis plan
Data normality is assessed using the Shapiro-Wilk normality test. Descriptive analysis is used to characterize the study population, with categorical variables presented as absolute (n) and relative (%) frequencies, normally distributed variables as the mean and standard deviation, and asymmetrically distributed variables as the median and interquartile range.
The diagnostic accuracy will be calculated using the epiR package. The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and 95% confidence intervals for all estimates will be calculated. Univariate and multivariate logistic modeling are conducted to evaluate the relationship between the outcome (PTB and TB infection) and predictor characteristics (risk factors), as described in Table 1. Odds ratios (ORs) with 95% confidence intervals will be calculated.
Table 2 presents, in a more direct way, the population involved, the statistical analysis plans, and how we will handle missing data for each study aims and outcomes. Statistical analyses are performed in R 4.1.1 (R Foundation for Statistical Computing, Vienna, Austria; http://www.R-project.org), with a significance level of 5% for alpha error (P < 0.05).
Data sharing
The study protocol, case report forms, consent forms, and assent forms are available in the ReBEC repository, where the study is registered (U1111-1332–7450). The participant-level dataset and statistical codes can be shared upon request after the final analysis is published. In cases of data sharing, the confidentiality of each participant will be ensured by removing data that could identify them. In the case of data sharing, the confidentiality of each participant must be ensured by removing data that could identify them, such as their date and place of birth. Furthermore, this must comply with Brazilian resolutions on the conduct of research, including adherence to the rules for the development of research involving human beings and for data sharing.
Plan of study monitoring
The data quality collected and reported is systematically monitored for each participating center. Monitoring activities are carried out to verify adherence to Good Clinical Practices and the approved protocol. Remote monitoring focuses on data entry in REDCap and on reviewing regulatory documents. Centralized monitoring identifies missing data and distinguishes between reliable and potentially dubious data. Remote monitoring focuses on data entry in REDCap to identify systematic or significant errors in data collection and reporting, and on reviewing regulatory documents. On-site visits include verification of participant enrollment workflows, document storage and organization, consent and assent data, data consistency between CRFs and REDCap, adverse events, sample storage temperatures, and expiration of supplies. A report with corrective actions is provided following each visit.
Ethical approval and consent
Ethical approval was obtained by the ethical committee of the proposing institution (Hospital Moinhos de Vento, number 24730819.7.1001.5330). The study at the sites was initiated only after obtaining ethical approval from the local ethics committee. This study adheres to the Regulatory Guidelines and Norms for Research Involving Human Beings, as established by Resolution 466/12 of the Brazilian National Health Council and Law 14874/24, which regulates research involving human beings. Trained researchers obtain informed consent from participants’ legal caregivers before any study procedures. Assent is obtained from children aged 6 years or older who have the capacity to sign it. Study’s consent and assents form are available in ReBEC storage (https://ensaiosclinicos.gov.br/welcome - U1111-1332–7450).
Risk/harms
The risks include those inherent to the collection of biological material, such as nebulization (induced sputum), secretion aspiration, nasopharyngeal and nasal swabs, and venipuncture. The risks of nebulization for induced sputum include coughing, nasal itching, sneezing, nasal secretion, wheezing, discomfort during nebulization, or malaise. The collection of respiratory secretions (aspiration) can cause local pain, nosebleeds, vomiting, or coughing. The possible reactions are monitored and include: mild epistaxis, increased coughing, and wheezing responsive to an inhaled bronchodilator.
The collection of nasopharyngeal and nasal swabs can cause momentary discomfort, such as nausea, coughing, and tearing (due to the procedure’s cough reflex). Blood collection presents risks, including discomfort, pain, local bleeding, or bruising at the puncture site.
TST application can cause pain and burning at the time of application, and afterward, it can cause itching, local discomfort, local lesions, and blisters (known reactions of the test). These reactions are limited, resolve in a few days, and pose no serious risk to the participant.
To safeguard participant confidentiality and minimize potential risk or harm, participants’ identities remain anonymous, and any personal identifiers are replaced through pseudonymization procedures. Linkage between research data and individual participants will be possible exclusively to authorized members of the research team, who are also involved in the participant’s clinical care. No identifying information will be disclosed in publications or shared datasets.
If an adverse event occurs during study procedures, researchers follow local emergency protocols to ensure participants receive immediate medical attention. The principal investigators at both the local site and the coordinating center receive prompt notification and implement the necessary corrective measures. The study does not provide financial or non-financial incentives to participants.
Dissemination plan
All results from this study will be published in scientific journals, presented at relevant conferences in the field, and communicated to the study sponsor (the Brazilian Ministry of Health) through a report. Once published, the results will also be widely disseminated in the media.
Artificial intelligence tools and technologies
Microsoft Copilot and Grammarly were used to support the manuscript’s English revision. The authors revised the tool’s outputs for validity before they were accepted for inclusion in the manuscript. No article contents, data, or supporting files were affected or generated by the use of an artificial intelligence tool.
Discussion
This study represents the first nationwide investigation into the prevalence of PTB in children and adolescents hospitalized with LRTI in a large country with a high tuberculosis burden, such as Brazil. Additionally, the current study presents an opportunity to collect data in the years after the COVID-19 pandemic, when higher rates of intra-domiciliary transmission are expected. Notably, although Brazil has a recognized high TB burden, it has a significantly lower incidence compared to many countries in Africa and Asia [32]. Previous studies have been retrospective, relying on data from notification systems [15,16]. The present study will provide prospective data from a population with LRTI across multiple centers in Brazil, which may better reflect the true prevalence of PTB in Brazilian children and young adolescents. By addressing this critical gap in the literature, the study may contribute to a greater understanding of PTB epidemiology in pediatric populations with LRTI, providing essential data to guide public health strategies in similar settings.
Beyond the geographical coverage, one of the study’s strengths is its pioneering approach in Brazil, which combines induced sputum collection or tongue swabs and molecular biology techniques, such as Ultra, for diagnosing PTB in children and young adolescents. A significant increase in diagnostic yield has been demonstrated in settings with very high TB incidence in South Africa, reaching a sensitivity higher than 70% [8]. However, as mentioned above, the accuracy of these tests in a setting with intermediate TB incidence may differ significantly. Moreover, this study will provide novel data on the prevalence of TBI in Brazil and the accuracy of pediatric PTB prediction scores used in the country. It will also evaluate the role of IGRAs within these algorithms, which traditionally is based on the TST [20]. Other important data generated by the study will be the prevalence of viral and bacterial pathogens in children and adolescents hospitalized with LRTI, a leading cause of death in children, especially in children under five. Despite the significant progress made during the last decades, LRTIs are still responsible for over 500,000 deaths in under-fives, and close to 50,000 for those from 5 to 14 [33]. This information can serve as a basis for public policies related to immunization and epidemic control of viral and bacterial pathogens among children and adolescents in Brazil.
This study has some potential limitations. First, an inherent challenge remains in the laboratory confirmation of viral and bacterial LRTI, especially in children. Moreover, large multicenter studies investigating the etiology of childhood pneumonia that included asymptomatic controls, such as the PERCH study, have demonstrated that specific pathogens, such as Rhinovirus, are detected at similar rates in both pneumonia cases and controls, making etiological attribution challenging [34]. Second, given that the study’s primary objective in the hospital-based arm is to investigate the prevalence of PTB among patients with LRTI, the coordinating team emphasizes training and monitoring activities to ensure that participants with highly suggestive TB cases are not exclusively recruited, thereby preventing an overestimation of prevalence. Third, the second IS sample from hospitalized participants is not sedimented, which may reduce sensitivity. However, a sensitivity analysis will be conducted, excluding the non-sedimented samples, for the prevalence analysis. Finally, missing data is unavoidable due to the large volume of data and samples collected, as well as the study’s heterogeneous settings and extensive geographical coverage. However, training sessions and monitoring activities are conducted throughout the recruitment period to mitigate these risks. We also accounted for a 20% loss to ensure a sufficient sample size for the study’s primary aim in the outpatient arm.
In conclusion, the results of the TBPed Brazil study will provide critical epidemiological data on PTB and other respiratory pathogens in Brazil, serving as a baseline for future studies and guiding public health policies. Furthermore, based on the findings, the study could serve as a starting point for using a combination of induced sputum collection and molecular biology techniques in public health in Brazil, thereby enhancing the yield of laboratory tests to confirm PTB diagnosis in children and adolescents.
Supporting information
S1 TableChecklist SPIROS – Standardized protocol items: Recommendations for observational studies.(PDF)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Basile FW, Nabeta P, Ruhwald M, Song R. Pediatric Tuberculosis Diagnostics: Present and Future. J Pediatric Infect Dis Soc. 2022;11(Supplement_3):S 85–93. doi: 10.1093/jpids/piac 082 36314546 PMC 9620430 · doi ↗ · pubmed ↗
- 2Gunasekera KS, Marcy O, Muñoz J, Lopez-Varela E, Sekadde MP, Franke MF, et al. Development of treatment-decision algorithms for children evaluated for pulmonary tuberculosis: an individual participant data meta-analysis. Lancet Child Adolesc Health. 2023;7(5):336–46. doi: 10.1016/S 2352-4642(23)00004-4 36924781 PMC 10127218 · doi ↗ · pubmed ↗
- 3Carvalho RF, Carvalho ACC, Velarde LGC, Rossoni AMO, Aurilio RB, Sias SMA, et al. Diagnosis of pulmonary tuberculosis in children and adolescents: comparison of two versions of the Brazilian Ministry of Health scoring system. Rev Inst Med Trop Sao Paulo. 2020;62:e 81. doi: 10.1590/S 1678-9946202062081 33146310 PMC 7608063 · doi ↗ · pubmed ↗
- 4Detjen AK, Di Nardo AR, Leyden J, Steingart KR, Menzies D, Schiller I, et al. Xpert MTB/RIF assay for the diagnosis of pulmonary tuberculosis in children: a systematic review and meta-analysis. Lancet Respir Med. 2015;3(6):451–61. doi: 10.1016/S 2213-2600(15)00095-8 25812968 PMC 4756280 · doi ↗ · pubmed ↗
- 5Dorman SE, Schumacher SG, Alland D, Nabeta P, Armstrong DT, King B, et al. Xpert MTB/RIF Ultra for detection of Mycobacterium tuberculosis and rifampicin resistance: a prospective multicentre diagnostic accuracy study. Lancet Infect Dis. 2018;18(1):76–84. doi: 10.1016/S 1473-3099(17)30691-6 29198911 PMC 6168783 · doi ↗ · pubmed ↗
- 6Carratalà-Castro L, Munguambe S, Saavedra-Cervera B, de Haas P, Kay A, Marcy O, et al. Performance of stool-based molecular tests and processing methods for paediatric tuberculosis diagnosis: a systematic review and meta-analysis. Lancet Microbe. 2025;6(6):100963. doi: 10.1016/j.lanmic.2024.100963 39547244 PMC 12062341 · doi ↗ · pubmed ↗
- 7Olbrich L, Franckling-Smith Z, Larsson L, Sabi I, Ntinginya NE, Khosa C, et al. Sequential and parallel testing for microbiological confirmation of tuberculosis disease in children in five low-income and middle-income countries: a secondary analysis of the Ra Paed-TB study. Lancet Infect Dis. 2025;25(2):188–97. doi: 10.1016/S 1473-3099(24)00494-8 39312914 · doi ↗ · pubmed ↗
- 8Zar HJ, Workman LJ, Prins M, Bateman LJ, Mbhele SP, Whitman CB, et al. Tuberculosis Diagnosis in Children Using Xpert Ultra on Different Respiratory Specimens. Am J Respir Crit Care Med. 2019;200(12):1531–8. doi: 10.1164/rccm.201904-0772 OC 31381861 PMC 6909828 · doi ↗ · pubmed ↗