Establishing diversity, equity, inclusion and justice task forces for District of Columbia area cancer centers: Lessons learned implementing efforts in oncology
Katarina E. AuBuchon, Anne McDonnell, Hannah Arem, Teletia Taylor, Yasmine M Kanaan, Marjorie C. Gondré-Lewis, Barbara W. Harrison, Nicole P. Chapell, Julie E. Bauman, Christopher J. King, Pavani Chalasani, Christopher Gallagher, Carla D. Williams, Mandi L. Pratt-Chapman

TL;DR
This paper describes efforts to reduce cancer health inequities by establishing DEIJ task forces in three Mid-Atlantic cancer centers and shares lessons learned.
Contribution
The paper introduces a multi-center DEIJ task force model with an educational curriculum aligned with CLAS and DC Health Equity Framework standards.
Findings
Task forces made progress on improving patient information accessibility and expanding implicit bias training.
Challenges included limited data, competing priorities, and insufficient institutional resources.
Clear data collection, staff time, leadership commitment, and resources are critical for DEIJ success.
Abstract
To address observed cancer health inequities resulting from historically-embedded structural bias in quality, equity, and access to health care delivery, we organized and coordinated Diversity, Equity, Inclusion, and Justice (DEIJ) Task Forces across three cancer centers in the Mid-Atlantic region. We recruited multi-disciplinary, diverse faculty and staff for each task force to optimize capacity to implement sustainable, effective strategies for institutional change. We developed an educational curriculum aligned with enhanced National Culturally and Linguistically Appropriate Services (CLAS) Standards and the DC Hospital Health Equity Framework. Over 18 months, task force members were invited to 14 sessions designed to help teams assess and prioritize critical areas for improvement through organizational assessments and then create and implement action plans. Task force goals…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
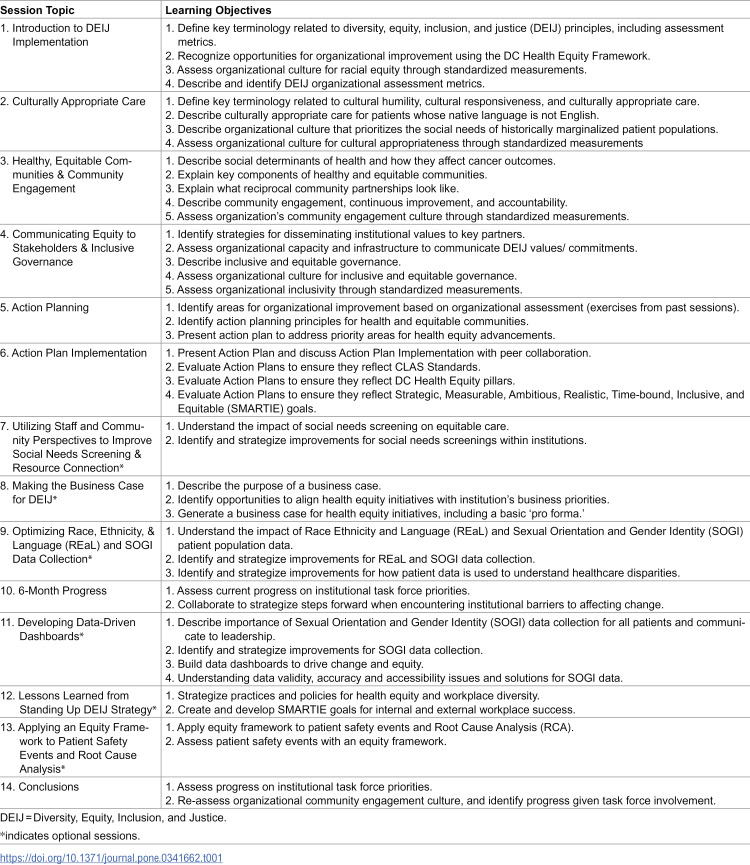 Figure 1
Figure 1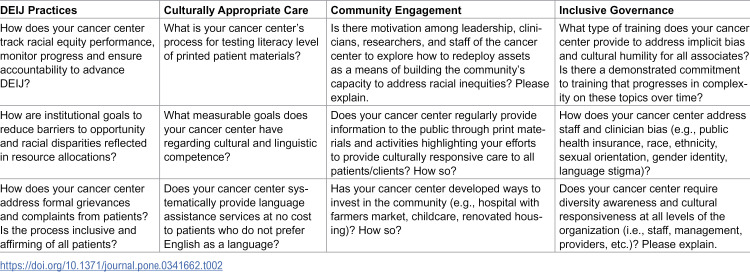 Figure 2
Figure 2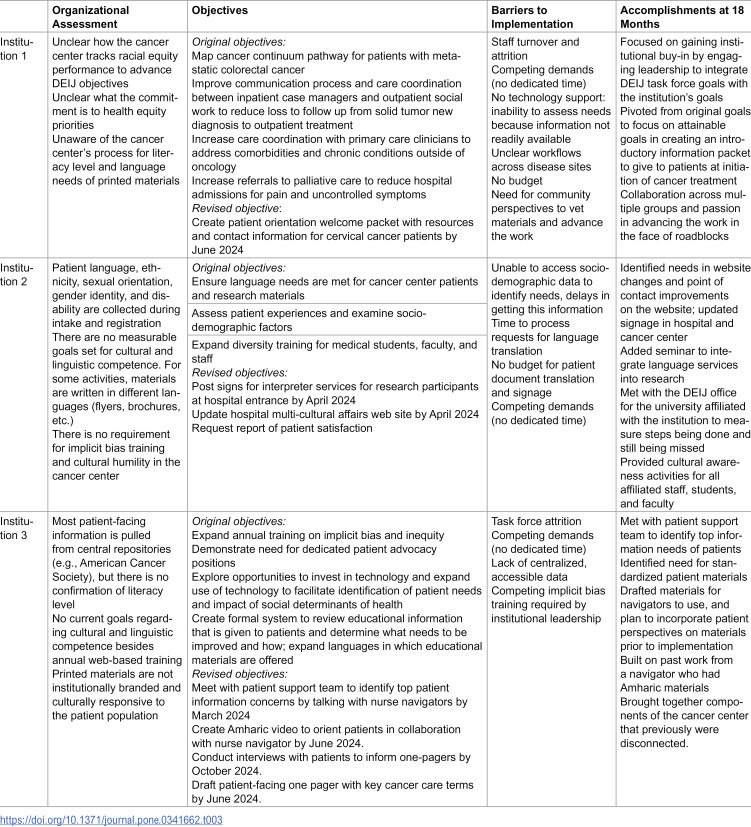 Figure 3
Figure 3- —http://dx.doi.org/10.13039/100000030Centers for Disease Control and Prevention
- —http://dx.doi.org/10.13039/100000054National Cancer Institute
- —http://dx.doi.org/10.13039/100000030Centers for Disease Control and Prevention
- —http://dx.doi.org/10.13039/100006108National Center for Advancing Translational Sciences
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Cancer Incidence and Screening · Cultural Competency in Health Care · Economic and Financial Impacts of Cancer
Introduction
Cancer inequities are unfair, unjust, and avoidable differences in cancer burden and outcomes that are caused by social, economic, and environmental disadvantages [1,2]. Observed cancer health inequities among historically marginalized people (e.g., Black people, LGBTQ+ people) are caused by structural classism [3], racism [4–6] sexism [7], cis-heterosexism [8,9], and their intersections. Ultimately, cancer inequities require multi-level interventions to dismantle systemic biases and address long-standing barriers to care access [10–12]. Diversity, Equity, Inclusion, Justice (DEIJ) commitments implemented in cancer centers – from the clinic to the leadership – can meaningfully advance health equity.
To address observed cancer health inequities [13–15] we organized and coordinated three DEIJ Task Forces in their respective cancer centers, each with distinct clinical environments and diverse patient populations. The task forces assessed, prioritized, and implemented strategies to address structural inequities impacting historically marginalized patients.
Methods
This study was approved by the Georgetown University IRB (#00004397). All participants consented verbally or in writing to participate in DEIJ Task Force activities. Decisions made in the course of operations to advance DEIJ Task Force work have been summarized here.
Framework
To build capacity for task force members, we developed a curriculum [16] aligned with enhanced National Culturally and Linguistically Appropriate Services (CLAS) Standards [17] and the District of Columbia (DC) Health Equity Framework [18]. These frameworks ensured alignment of task force goals with pre-existing hospital leadership commitments.
Curriculum development
The curriculum was organized into eight required educational sessions and six optional technical assistance sessions (Table 1). Sessions progressed from evaluating individual-level biases to examining institutional-level policies and practices to exploring successes at other institutions initiating structural changes. Optional technical assistance sessions from external subject matter experts were available to learn from successful efforts at other institutions. All sessions were open to the public for individuals to promote collaborative information sharing [19]. All sessions were recorded and made publicly available [16].
Table 1: DEIJ task force educational sessions.
Task force development
Institutional Principal Investigators (PIs) identified five to eight multidisciplinary champions from diverse occupational backgrounds (e.g., research, clinical) and roles (e.g., physicians, nurse managers, community health workers, research associates) to join their respective institutional task force. By recruiting task force members from diverse backgrounds and roles, we aimed to identify individual blind spots and implement sustainable and effective strategies for institutional change.
Development of DEIJ goals
In July 2023, each task force began an organizational assessment (see Table 2) which guided the task forces’ action plan development. Each task force developed a 12-month action plan with goals based on needs identified during the organizational assessment.
Table 2: Select questions from organizational assessment.
Task forces refined goals into specific, measurable, achievable, relevant, time-bound, inclusive, and equitable (SMARTIE) goals, which evolved over time based on what was within the authority and capacity of task force members (see Table 3) [20].
Table 3: Evolution of task force goals and accomplishments.
Peer learning approach
Each task force shared their action plan with and obtained feedback from peer task forces. The three task forces convened at 6, 12, and 18 months for cross-institutional sharing to discuss their progress and share lessons learned.
Results
Action plans prioritized improving patient information accessibility, expanding the reach of implicit bias training, and improving accurate socio-demographic data collection to assess inequities. Overall, SMARTIE goals evolved over time (see Table 3). Progress was made in improving accessibility of patient information and expanding reach of implicit bias training, but little progress was made on improving accurate socio-demographic data collection.
Improving patient information accessibility
All three task forces improved accessibility of patient-facing materials by creating new patient information resources, lowering the reading level of existing resources, and/or translating materials into additional languages. Institution 1 developed an introductory packet to provide to patients at the initiation of cancer treatment and began work on disease-specific information packets for patients. Institution 2 identified major language needs. Working with their institutional DEIJ office, they created an expedited assessment and review process for materials, revised the institution’s website to direct people to language services, and hosted an educational seminar on language services available within the institution. This work resulted in improved integration of interpretation services across departments. Institution 3 worked with nurse navigators to develop a standardized information sheet with definitions of common cancer-related terminology for patients.
Implicit bias training
All three institutions expanded implicit bias training for cancer center staff and providers [21]. Institutions 1 and 2 attained a high training completion rate, but institution 3 was challenged by receiving notice of a competing implicit bias training that was made mandatory at their institution. Because the rollout of the mandatory training was independent from the task force, the total percentage of clinicians and staff that completed any kind of implicit bias training at institution 3 was unavailable. Thus, while the completion rate was low for the task force provided training, exposure to some bias training was likely higher.
Improving accurate socio-demographic data
Data gaps led to incomplete organizational assessments at the very beginning of the 18-month quality improvement process. These challenges led the task forces to try to improve accessibility of accurate socio-demographic data. However, little progress was made on this goal due to lack of task force authority to change data collection processes, workflows, and relevant medical record forms.
Discussion
There is an urgent need to advance cancer health equity in the US [22]. Our quality improvement project contributes to the literature by documenting accomplishments and challenges in implementing DEIJ initiatives in clinical cancer care environments. Though many academic medicine DEIJ initiatives focus on a sense of belonging for historically marginalized faculty and staff [23], and increasing knowledge of systemic injustices [24–26], our task forces specifically sought to improve equity for patients in the context of cancer care delivery.
A major overall accomplishment of the task forces was to infuse DEIJ efforts into operations and higher-level discussions at three University-affiliated cancer centers in Washington, DC. DEIJ initiatives at other US academic institutions are often led by assistant professors [26]; however, we were able to recruit leaders across multiple levels of influence (administrative, patient care, research) to collaborate on our DEIJ task forces. Across the three institutions, steps were taken toward advancing CLAS standards in practice and integrating DEIJ values into institutional culture. Our focus on patient education and quality improvement aligns with needs identified in the literature. For example, in a study of individuals initiating DEIJ work in radiation oncology, 23 of 34 (76%) respondents expressed that patient education was a primary focus [26].
Lessons learned included the importance of leadership engagement and buy-in and the critical need for protected time and designated staff to advance specific DEIJ work. DEIJ champions in other institutional settings have reported challenges such as fatigue from individuals spearheading initiatives in their institutions, limited time/competing demands and lack of leadership buy-in [27]. Our experience suggests that providing protected time for staff whose roles align with and are rewarded by DEIJ work can contribute to more rapid achievement of DEIJ goals. Additionally, we found that when DEIJ principles were centered in an organization’s mission, requests for increased resources and staff to advance DEIJ goals were more successful. Integrating goals with quality improvement requirements for cancer committee accreditation also facilitated greater success.
Barriers to success included limited human resources (e.g., staff turnover, competing demands) and institutional support (e.g., data access, protected time). For institutions 1 and 3, DEIJ work was not explicitly rewarded. Without clear resources, protected time or institutional incentives, members at institutions 1 and 3 were unable to devote the effort they wished to achieve their team goals, reporting structural barriers to success related to capacity and commitment. Members at these two institutions reported an underlying perception that DEIJ work is approved, but pragmatically un-supported (e.g., protected time). Staff turnover slowed down task force work at these two institutions. Our experience aligns with previously reported limitations to DEIJ work documented in the literature. For example, among 50 radiation oncology departments with DEIJ initiatives, only 38.2% of DEIJ leaders had administrative support, only 29.4% had funding, and only 23.5% had protected time [26].
All task forces faced barriers with hierarchal, bureaucratic departments and structural or cultural barriers, as well. For example, institution 1 reported a heavily siloed structure that impeded cross-departmental collaboration. Institution 2 struggled to identify patient information needs, as patient materials were not clearly identifiable and organized for sharing with the task force. Additionally, institution 2 reported issues assessing patient experience disparities due to limited access to patient socio-demographic data, creating a “no data, no problem” problem.
Despite these obstacles, each institution made significant progress by refining their objectives to focus on more attainable goals and fostering collaboration across departments. The success of the task forces was driven by the dedication, enthusiasm, motivation, and cross-departmental collaboration of its members. This propelled progress and energized efforts. All task forces were committed to sustaining DEIJ work through collaborative efforts, expanded engagement of clinical leadership, and improved institutional alignment.
This study is limited to the experiences of only three cancer centers clustered in one geographic area. However, sharing these lessons will be helpful for institutions seeking structural change in other institutional and geographic settings. Other clinical settings wishing to improve DEIJ can leverage our lessons learned by obtaining early leadership buy-in, integrating manageable DEIJ goals within institutional strategic imperatives, distributing tasks among task force members with the authority and capacity to advance group goals, and rewarding DEIJ work in practice through workload reductions, dedicated time, and other recognition aligned with institutional values.
While we discussed at great length whether to include patient representatives in each task force, we opted to forgo patient representatives to encourage candor around internal challenges. Yet, this does limit our perspective to that of internal team members at each cancer center. Future work should, when possible, include patient perspectives to ensure meaningful improvements align with patient needs. Future work could also consider establishing a platform for community collaboration where task force members can share resources, learnings, and best practices with community members [22]. Collaboration with external community organizations may provide valuable support and motivation to overcome challenges.
Finally, while the findings of our assessments and action plans are specific to the institutions involved in our study, the educational recordings of task force sessions and affiliated resources of sessions are published and accessible to all on the www.cancercontroltap.org technical assistance web site [16]. Resources include downloadable templates that other institutions may use to conduct their own organizational assessment and action planning.
Conclusion
Developing a multi-disciplinary task force to advance DEIJ goals created meaningful improvements in our study. However, strong institutional leadership buy-in, alignment with strategic priorities, protected time and resources, and authority to advance structural change are critical to build an inclusive organizational culture and operationalize DEIJ values into policies and practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1National Cancer Institute. Cancer Disparities. https://www.cancer.gov/about-cancer/understanding/disparities. 2024.
- 2AACR Cancer Disparities Report 2024. American Association for Cancer Research. 2024. https://cancerprogressreport.aacr.org/disparities/
- 3Levit LA, Byatt L, Lyss AP, Paskett ED, Levit K, Kirkwood K, et al. Closing the rural cancer care gap: three institutional approaches. JCO Oncol Pract. 2020;16(7):422–30. doi: 10.1200/OP.20.00174 32574128 · doi ↗ · pubmed ↗
- 4Best AL, Roberson ML, Plascak JJ, Peterson CE, Rogers CR, Hastert TA, et al. Structural racism and cancer: calls to action for cancer researchers to address racial/ethnic cancer inequity in the United States. Cancer Epidemiol Biomarkers Prev. 2022;31(6):1243–6. doi: 10.1158/1055-9965.EPI-21-1179 35642391 PMC 9306268 · doi ↗ · pubmed ↗
- 5King CJ, Buckley BO, Maheshwari R, Griffith DM. Race, place, and structural racism: a review of health and history in Washington, D.C. Health Aff (Millwood). 2022;41(2):273–80. doi: 10.1377/hlthaff.2021.01805 35130070 · doi ↗ · pubmed ↗
- 6Gondré-Lewis MC, Abijo T, Gondré-Lewis TA. The opioid epidemic: a crisis disproportionately impacting black americans and urban communities. J Racial Ethn Health Disparities. 2023;10(4):2039–53. doi: 10.1007/s 40615-022-01384-6 36068482 PMC 9447354 · doi ↗ · pubmed ↗
- 7Keenan BP, Barr E, Gleeson E, Greenberg CC, Temkin SM. Structural Sexism and Cancer Care: The Effects on the Patient and Oncologist. Am Soc Clin Oncol Educ Book. 2023;43:e 391516. doi: 10.1200/EDBK_391516 37155944 · doi ↗ · pubmed ↗
- 8Matthews AK, Breen E, Kittiteerasack P. Social determinants of LGBT cancer health inequities. Semin Oncol Nurs. 2018;34(1):12–20. doi: 10.1016/j.soncn.2017.11.001 29373163 · doi ↗ · pubmed ↗