Trigeminocardiac Reflex Associated With Orthognathic Surgery: An Illustrative Case Report and Review of the Literature
Asiya Yusuf, Ashley Ferro, Oliver Vij, Thomas Mathew, Jithesh Appukutty, Vijayarajan Santhanam

TL;DR
This paper reports a rare brainstem reflex during orthognathic surgery and reviews existing literature to understand its causes and outcomes.
Contribution
The paper presents a new case of TCR during Le Fort I osteotomy and systematically reviews existing cases to identify patterns and triggers.
Findings
Maxillary downfracture or mobilization were the most common triggers of TCR in orthognathic surgery.
Despite requiring cardiopulmonary resuscitation in two cases, all patients completed their procedures without long-term adverse outcomes.
More innocuous triggers of TCR were also identified in the reviewed cases.
Abstract
The trigeminocardiac reflex (TCR) is a rare brainstem reflex characterized by bradycardia and hemodynamic instability secondary to stimulation of branches of the trigeminal nerve. In maxillofacial surgery, the phenomenon has been reported in orthognathic surgery, foreign body removal, and fixation of midface fractures. Despite reasonably extensive reporting of the reflex in head and neck surgery in general, the mechanism and predisposing factors are poorly understood. The primary aim of this systematic review was to explore potential contributory factors and summarize outcomes of the TCR in patients undergoing orthognathic surgery. We additionally report a case of asystole in a 21-year-old male undergoing Le Fort I osteotomy. A systematic literature search was undertaken using MEDLINE, Embase, Web of Science, Scopus, and PubMed from inception to December 24, 2025, for articles reporting…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
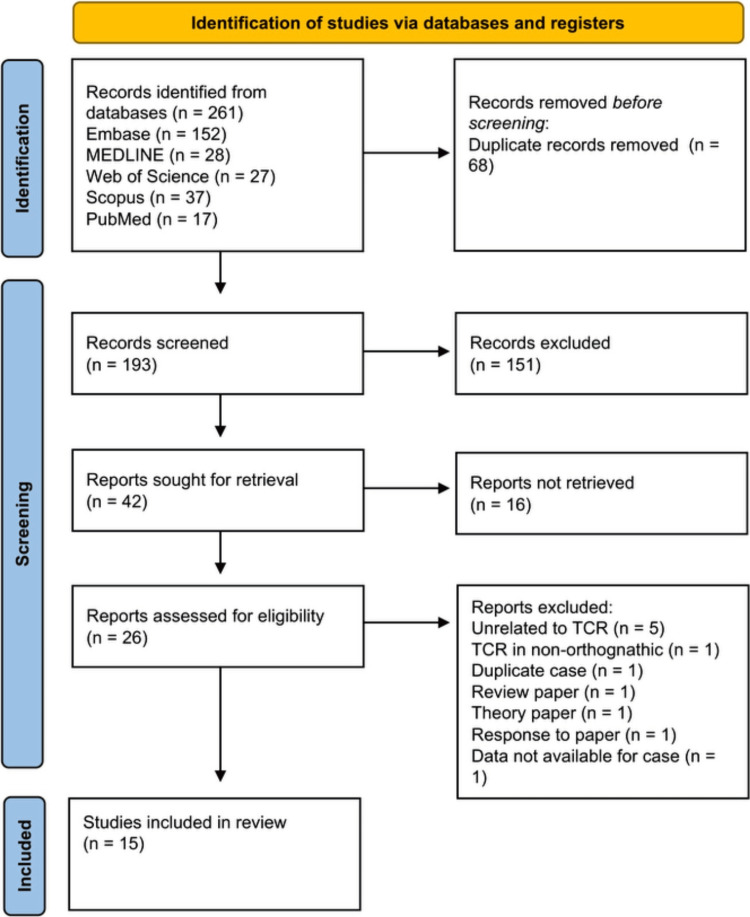 Figure 1
Figure 1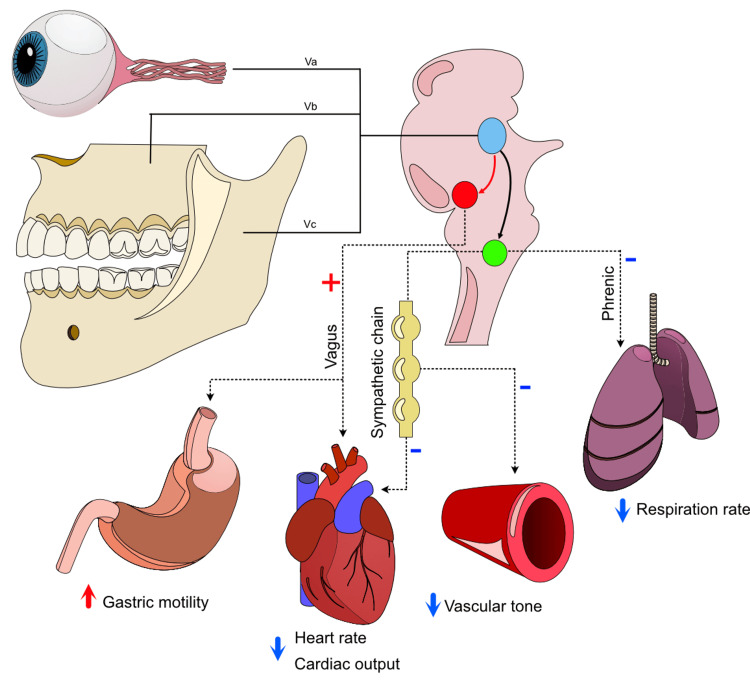 Figure 2
Figure 2| Phase of procedure | Pharmacologic agents |
| Induction and maintenance anesthesia | Propofol+remifentanil (TIVA) |
| Paralysis | Atracurium |
| MAP management | Magnesium infusion (2 mmol); clonidine bolus (105 µg) |
| Adjunctive agents at induction | Midazolam 2 mg; dexamethasone 6.6 mg; co-amoxiclav 1.2 g IV; Hartmann’s compound sodium lactate solution 200 mL |
| Local anesthesia | A 17.6 mL lidocaine hydrochloride 2%+1:80000 adrenaline via infiltration, divided between the maxillary and mandibular operative sites |
| During asystole | Atropine 60 µg |
| Case number | Study (citation) | Age (years)/sex | Past medical history | Planned procedure | Anesthetic details | Asystole/event | Inciting event | Management of reflex | outcome |
| 1 | Aggarwal K, et al. (2020) [ | 20 M | Cleft repair aged 6 years | Le Fort I osteotomy | Not reported | Transient bradycardia 40/min | Maxillary mobilization | Mobilization discontinued; procedure recommenced more gradually following HR recovery. | Follow-up not reported |
| 2 | Alshalawi H, et al. (2024) [ | 32 M | Nil | Le Fort I osteotomy, BSSO, and genioplasty | Not reported | Transient bradycardia 25/min | Downward digital pressure on maxilla following osteotomy | Mobilization discontinued; atropine administered | Admission for 2 days for observation; postoperative ECG unremarkable. Discharged |
| 3 | Barnard NA, et al. (1990) [ | 26 F | Nil | Le Fort I osteotomy | Premedication: diazepam; induction with sodium thiopental and vecuronium; maintenance with enflurane | Transient bradycardia to 25/min with a "notable drop in blood pressure" | Maxillary downfracture | Mobilization discontinued; atropine administered | Postoperative ECG unremarkable. Discharged |
| 4 | Baronos S, et al. (2019) [ | 26 M | Not reported | Le Fort I osteotomy, BSSO, and genioplasty | Premedication midazolam; propofol, fentanyl, and rocuronium induction; desflurane and remifentanil maintenance | Asystole for 10 seconds | Insertion of bite block following completion of both Le Fort and BSSO | Glycopyrrolate administered, and procedure completed | No postoperative interventions. Discharged |
| 5 | Campbell R, et al. (1994) [ | 35 F | Nil | Le Fort I and Hofer osteotomy | Premedication midazolam; thiopental, fentanyl and succinylcholine induction; maintenance enflurane | Asystole for 10 seconds | Tuberosity osteotomy | Surgical stimulus discontinued, and enflurane vaporizer switched off | Follow-up not reported |
| 6 | Hasegawa R, et al. (2025) [ | 39 F | Nil | Le Fort I osteotomy and BSSO | Induction propofol, remifentanil, and rocuronium; propofol and remifentanil maintenance | Transient bradycardia to 46/min | Maxillary downfracture | Downfracture discontinued, and recommenced following LA infiltration | No further investigation |
| 7 | Hasegawa R, et al. (2025) [ | 26 M | Nil | Le Fort I osteotomy and BSSO | Induction propofol, remifentanil, and rocuronium. Sevoflurane, remifentanil, and fentanyl maintenance | Transient bradycardia to 52/min, with associated drop in BP to 54/25 mmHg | Mandibular split during BSSO | Pause to surgical stimulus; administered ephedrine hypochloride | No further investigation |
| 8 | Kim H (2019) [ | 23 M | Nil | BSSO | Premedication midazolam. Propofol, remifentanil, and rocuronium induction. Sevoflurane and remifentanil maintenance | Transient bradycardia to 25/min | During fixation of BSSO (post-osteotomy) | Surgery paused, and resumed following recovery of HR | Postoperative ECG unremarkable |
| 9 | Lang S, et al. (1991) [ | 28 F | Congenital ventricular septal defect | Unilateral segmental maxillary advancement | Oral clonidine premedication. Induction with thiopentone, sufentanil, and atracurium. Isoflurane for maintenance | Asystole 3 seconds | Mobilization of maxillary segment | Pause to surgery and atropine administered | Patient monitored in recovery uneventfully and discharged |
| 10 | Lang S, et al. (1991) [ | 26 F | Nil | Le Fort I osteotomy, BSSO, and genioplasty | Induction using thiopentone, fentanyl, and succinylcholine. Maintenance using isoflurane and fentanyl | Asystole; duration not reported | Subperiosteal placement of channel retractor during BSSO | Pause to surgery and lidocaine (local) and atropine administered | Postoperative ECG demonstrated sinus arrhythmia only |
| 11 | Lang S, et al. (1991) [ | 38 F | Nil | Le Fort I osteotomy and BSSO | Induction using thiopentone, alfentanil and succinylcholine. Maintenance using halothane | Transient bradycardia from 95/min baseline to 65/min | Maxillary mobilization | Pause to maxillary mobilization | Follow-up not reported |
| 12 | Maharaj K, et al. (2020) [ | 45 M | Not reported | Le Fort I osteotomy and BSSO | Not Reported | Transient bradycardia; severity not specified | Maxillary mobilization | Pause to procedure. Recommenced following recovery of HR | Follow-up not reported |
| 13 | Miyamoto J, et al. (2012) [ | 18 F | Childhood asthma aged 5 years | Le Fort I osteotomy, BSSO, and genioplasty | Induction using propofol, rocuronium and fentanyl; sevoflurane and fentanyl for maintenance | Bradycardia 12/min; presumed asystole given CPR commenced | During closure of genioplasty incision (post-completion of all osteotomies) | CPR commenced; atropine administered, and procedure completed | Postoperative ECG unremarkable. Admission for continued observation and discharged 2 weeks post-procedure |
| 14 | Ortiz-Peces L, et al. (2025) [ | 36 M | Obesity | Le Fort I osteotomy and BSSO | Induction using midazolam, fentanyl, propofol, and rocuronium. Maintenance using propofol and dexmedetomidine | Asystole 5 seconds | During dysjunction of mandible following BSSO | Pause to surgery and atropine administered | Follow-up not reported |
| 15 | Ragno JR, et al. (1989) [ | 17 M | Acne | Le Fort I osteotomy and BSSO | Diazepam pre-medication. Induction using thiopental, succinylcholine. Maintenance using isoflurane and sufentanil | Asystole; duration not reported | Maxillary downfracture | Pause to procedure. Recommenced following recovery of HR | Overnight stay on the ward. Additional investigation not reported |
| 16 | Sanuki T, et al. (2009) [ | 31 F | Nil | BSSO | Induction using propofol and rocuronium. Maintenance using sevoflurane and remifentanil | Asystole 8 seconds | Soft tissue dissection to access mandible for BSSO | Pause to surgery and atropine administered | Follow-up not reported |
| 17 | Sugiyama S, et al. (2020) [ | 31 F | Nil | Le Fort I osteotomy and BSSO | Not reported | Transient bradycardia 29/min | During dysjunction of mandible following BSSO | Pause to surgery and lidocaine (local) and atropine administered | Follow-up not reported |
| 18 | Current case | 21 M | Nil | Le Fort I osteotomy and BSSO | Induction with propofol, remifentanil, and atracurium. Maintenance using propofol and remifentanil | Asystole 20 seconds | Maxillary mobilization | Pause to surgery and atropine administered; CRP commenced | Persistent bradycardia 44/min until morning following event. Discharged without complication. No cardiology follow-up recommended |
| Characteristic | Outcome | Frequency, n(%) |
| Age, Years (median(range)) | 27 (17-45) | - |
| Gender, female (n(%)) | 9 (50) | - |
| Planned procedure (n(%)) | Le Fort I osteotomy | 2 (11.1) |
| Le Fort I, BSSO, and genioplasty | 4 (22.2) | |
| Le Fort I and BSSO | 8 (44.4) | |
| BSSO only | 2 (11.1) | |
| Le Fort I, Hofer osteotomy | 1 (5.6) | |
| Segmental advancement | 1 (5.6) | |
| Anaesthetic induction (n(%)) | Thiopental sodium | 4 (28.6) |
| Propofol | 10 (71.4) | |
| Anaesthetic maintenance (n(%)) | Inhalation | 11 (78.6) |
| TIVA | 3 (21.4) | |
| Event (n(%)) | Bradycardia | 10 (55.6) |
| Asystole | 8 (44.4) | |
| Inciting event (n(%)) | Maxillary downfracture/mobilization | 9 (50) |
| BSSO dysjunction | 3 (16.7) | |
| Maxillary tuberosity osteotomy | 1 (5.6) | |
| Insertion bite block | 1 (5.6) | |
| Subperiosteal mandibular retraction | 1 (5.6) | |
| Fixation of BSSO | 1 (5.6) | |
| Soft tissue incision for BSSO | 1 (5.6) | |
| Post-osteotomy closure | 1 (5.6) | |
| Duration of asystole (if present), seconds (median(range)) | 9 (3-20) | |
| Management (n(%))* | Pause to surgery only | 5 (27.8) |
| Administration of atropine | 9 (50) | |
| Administration of LA | 3 (16.7) | |
| Administration of glycopyrrolate | 1 (5.6) | |
| Administration of ephedrine | 1 (5.6) | |
| Cardiopulmonary resuscitation | 2 (11.1) | |
| Outcome (n(%)) | Procedure completed | 18 (100) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTrigeminal Neuralgia and Treatments · Dental Anxiety and Anesthesia Techniques · Migraine and Headache Studies
Introduction
The incidence of intraoperative bradycardia in Oral and Maxillofacial surgery was initially described by Aschner and Dagnini in 1908 and attributed to the oculocardiac reflex [1]. The phenomenon, designated as the "Aschner phenomenon," revealed that transient bradycardia was precipitated by traction on the extraocular muscles and an increase in ocular pressure, and could be elicited by applying direct pressure on the globe. A similar response was subsequently noted in non-orbital procedures, prompting recognition of the trigeminocardiac reflex (TCR). Clinically, this reflex may manifest as sudden bradycardia, hypotension, or even transient cardiac arrest, resolving when the stimulus is removed. It is now understood that the reflex is mediated via an interaction between afferent fibers of the trigeminal nerve and both the brainstem reticular formation and motor nucleus of the vagus nerve, provoking the physiological changes observed during the reflex.
Orthognathic procedures such as Le Fort osteotomies, bilateral sagittal split osteotomies (BSSO), and genioplasty involve direct mechanical stimulation, traction, or pressure on branches of the maxillary and mandibular divisions of the trigeminal nerve. These procedures involve controlled osteotomies and mobilization of the midface and mandible, often requiring substantial mechanical force, and are recognized manoeuvres for triggering the TCR [2]. Despite this, the true incidence of TCR during orthognathic surgery remains uncertain, with reported rates varying widely across the literature. Inconsistencies in terminology, diagnostic criteria, and reporting practices further complicate the interpretation and comparison of published data.
Ragno et al. reported the first published case of the TCR in orthognathic surgery in 1989, whereby a 17-year-old patient developed asystole following downfracture of the maxilla during Le Fort I osteotomy [3]. With increasing recognition of the reflex beyond the context of oral and maxillofacial Surgery, there has been increasing interest in better understanding the underlying mechanism and identifying modifiable risk factors, and it is now recognized that there are peripheral, central, and ganglion Gasseri subtypes [4]. Several factors have been suggested to influence the occurrence of TCR, including the type and intensity of surgical stimulus, depth of anesthesia, patient-related characteristics, and perioperative physiological variables [5]. However, much of the available evidence is derived from isolated case reports, small case series, or mixed craniofacial cohorts, limiting the applicability of findings specifically to orthognathic patients. As a result, the contributory factors associated with TCR in this population have not been clearly defined.
Given the elective nature of orthognathic surgery and the typically young and otherwise healthy patient population, improved understanding of perioperative risks is essential. Failure to recognize TCR intraoperatively may result in unnecessary escalation, prolonged cardiac arrest, or premature termination of surgery. The primary aim of this case report, with an accompanying review of the literature, is to evaluate reported cases of TCR in patients undergoing orthognathic surgery and to identify potential contributory factors associated with its occurrence. By synthesizing the available evidence, this review seeks to clarify current knowledge and highlight areas requiring further investigation.
Case presentation
A healthy 21-year-old Caucasian male with a skeletal class III malocclusion was admitted electively for Le Fort I maxillary osteotomy and bilateral mandibular sagittal split osteotomy under general anesthesia. Pre-operative assessment and physical examination were unremarkable, and there was no relevant past medical history. He had no family history of cardiovascular or hematological disease.
Throughout the procedure, the patient underwent standard noninvasive anesthetic monitoring, including noninvasive blood pressure (NIBP), pulse oximetry, electrocardiography (ECG), and depth-of-anesthesia monitoring (entropy). General anesthesia was induced and maintained using total intravenous anesthesia (TIVA) with propofol and remifentanil infusions (0.2 µg/kg/min). The patient was paralyzed with an atracurium bolus prior to endotracheal intubation. A magnesium infusion (2 mmol) and clonidine boluses (105 µg) were administered to facilitate hypotension and analgesia. Additional agents administered before the episode included midazolam 2 mg, dexamethasone 6.6 mg, amoxicillin-clavulanate 1.2 g, and 200 mL of Hartmann’s solution (Table 1).
The surgery proceeded uneventfully with the patient positioned supine. Local anesthetic (17.6 mL of lidocaine hydrochloride 2% 1:80000 adrenaline) was administered, divided between maxillary and mandibular sites. A standard vestibular approach was used, and the Le Fort I osteotomy, including downfracture of the maxilla, was completed. No preceding changes in heart rate variability or physiological disturbance to this point were noted. During mobilization of the maxilla using Rowe’s maxillary disimpaction forceps, there was a rapid escalation into severe sinus bradycardia followed by complete ventricular asystole. An asystolic period, directly witnessed by the anesthetic and surgical team, lasted approximately 20 seconds, during which no return of QRS complexes was seen on the ECG. The operating table was immediately repositioned to allow cardiopulmonary resuscitation (CPR). Chest compressions were initiated, and atropine 600 µg IV was administered. These immediate interventions resulted in the return of spontaneous circulation within one minute. Electroencephalography (EEG) confirmed a deep plane of anesthesia. Upon resumption of the procedure, further manipulation of the maxilla again precipitated bradycardia, which resolved after a second 600 µg dose of atropine. No further episodes of bradycardia were noted. Following intraoperative consultation with cardiology, a postoperative 12-lead ECG was performed, which demonstrated sinus bradycardia at 53 bpm with normal morphology, as well as sinus arrhythmia.
Postoperatively, repeat 12-lead ECGs were carried out in recovery every 30 minutes until return to the ward was deemed suitable. A chest X-ray showed no evidence of pneumothorax or hemothorax, and no abnormalities apart from historic rib fractures. However, bradycardia of 44 bpm persisted until the next morning. The cardiologist indicated that follow-up Holter monitoring was not required, as this was considered a transient vagal response and not a sustained heart block. The patient was discharged the following day uneventfully (postoperative day 1) and has had an otherwise unremarkable recovery following orthognathic surgery.
Discussion
The present case illustrates a pronounced intraoperative manifestation of TCR during maxillary mobilization, prompting a review of the existing literature to better define its clinical features, precipitating factors, and outcomes in the context of elective orthognathic surgery. This review identified a small number of reported cases, underscoring both the rarity of the phenomenon and the importance of prompt recognition and management.
Methods
This study was undertaken in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines.
Search strategy and selection criteria
A systematic literature search was performed using MEDLINE, PubMed Central, Embase, Scopus, and the Web of Science Core Collection on December 24, 2025, with no limitation on the timing of publication. Search terms for the reflex included “trigeminocardiac reflex,” “trigeminovagal reflex,” and “oculocardiac reflex”; terms for outcomes included “asystole,” “bradycardia,” “cardiac arrest,” and “arrhythmia”; and terms for procedures included “orthognathic” and “maxillofacial.” Full search strings are provided in Appendix 1. Studies were considered for inclusion based on the following: any case report or case series reporting on patients undergoing orthognathic surgery who demonstrated sufficient bradycardia or hemodynamic instability to allow recognition of a TCR. Cases were considered consistent with the TCR if a sudden onset of bradycardia (≥20% reduction from baseline) or asystole occurred temporally with trigeminal nerve manipulation and resolved with cessation of the stimulus or administration of an anticholinergic.
Exclusion criteria included case reports or series of the TCR in the context of non-orthognathic surgery, reports providing no data on patient outcomes, literature reviews, theoretical studies, or studies on nonhuman subjects. Recommendations and expert opinions were also excluded if they did not conform to the inclusion criteria above. Titles, abstracts, and full texts were independently screened by two authors according to the inclusion and exclusion criteria. References of identified articles were iteratively screened for additional records.
Data extraction
The following fields were extracted from each study: year of publication, patient age, patient sex, comorbidities, indication for orthognathic surgery, baseline skeletal pattern and planned movements, estimated blood loss, anesthetic agents used for induction and maintenance, duration of asystole or severity of bradycardia, precipitating factor for the TCR, management of the reflex, patient outcomes, and follow-up investigations.
Critical appraisal
The quality of included case reports was assessed using the JBI Collaboration Case Reports Critical Appraisal Tool [6]. This tool consists of eight questions assessing the quality of the case presentation, the description of diagnoses and interventions, and the quality of any takeaway lessons. The output of the tool was modified in this study to provide a numeric score of overall quality (0-8).
Study selection
The initial literature search identified 261 studies from five databases, 68 of which were excluded following de-duplication (Figure 1). Of these, 15 studies met the inclusion criteria. Although Precious and Skulsky (1990) met the inclusion criteria, reporting six cases of the TCR in Le Fort I osteotomy, details could not be extracted specifically for orthognathic cases; therefore, this study is not included in the analyses below, although it is described in the discussion and included in the overall case count within the review, as shown in the PRISMA flow diagram (Figure 1). Within the 14 remaining studies, 17 cases are reported, in addition to the current case.
PRISMA flow diagram of study selectionPRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analysis; TCR: trigeminocardiac reflex
Assessment of case report quality
The JBI Collaboration Case Reports Critical Appraisal Tool was used to assess case report quality. The median score was 8 (range 5-8), indicating that the majority of case reports provided comprehensive details of the cases included. The generally high appraisal scores supported inclusion of all identified cases, although variability in reporting quality reinforced the descriptive nature of the analysis.
Patient demographics and planned procedures
The median age of the 18 included cases was 27 years (range, 17-45 years). Nine procedures were performed in male patients; the remaining nine patients were female. With respect to the planned procedure, two cases were scheduled to undergo Le Fort I osteotomy only; four cases were planned for Le Fort I osteotomy, BSSO, and genioplasty; eight cases were planned for Le Fort I osteotomy and BSSO; two cases were planned for BSSO only; and one case was planned for Le Fort I and Hofer osteotomy (Table 2) [2,3,7-17].
Anesthetic details
All studies, with the exception of four, provided details on induction anesthesia, paralysis, and maintenance [7,9,14,18]. Among the reported studies, IV induction was used in all cases. Thiopental sodium, as expected, was utilized in older studies, whereas propofol was used in the remaining reported cases [3,8,11,17]. Maintenance anesthesia was achieved through inhalation in 11 cases, and via intravenous propofol (TIVA) in the remaining cases (including the current case) [2,3,8,10-13,15-17].
Trigeminocardiac reflex and inciting events
The severity of hemodynamic disturbance was variably reported, limiting precise comparison between cases. Transient bradycardia and asystole were reported as the manifestations of the TCR, with 10 cases reporting bradycardia, and the remaining eight (including the current case) specifically reporting asystole [2,3,7-11,13-18]. Although Miyamoto et al. (2012) did not specify “asystole,” asystole (rather than bradycardia alone) was inferred, given that the surgical team reportedly commenced cardiopulmonary resuscitation, implying a loss of cardiac output [12]. Of those presenting with asystole, duration was not specified in Lang et al. or Ragno et al. [3,11]. In studies specifying duration, asystole ranged from 3 seconds to 20 seconds in the current case [11].
The most common identified trigger was maxillary downfracture or mobilization following Le Fort I osteotomy, reported in nine (50%) cases (including the current case) [3,7-9,11,13,14]. The reflex was otherwise noted in the following instances: three cases reported the reflex during completion of dysjunction following BSSO; following maxillary tuberosity osteotomy; following insertion of a bite block (post-completion of osteotomy); following subperiosteal mandibular insertion of a channel retractor; during fixation of the BSSO; during soft tissue access to the mandible for BSSO; and during closure following completion of a Le Fort I osteotomy, BSSO, and genioplasty [2,10,11-13,15-18].
Outcome
The procedure was completed in all cases. All reports described a surgical pause during the period of either bradycardia or asystole. Five cases reported simply continuing the procedure without complication following recovery of cardiovascular parameters; nine cases (including the current case) reported administration of atropine; three reported infiltration of additional local anesthesia prior to resumption; one reported administration of glycopyrrolate; and one reported use of ephedrine [2,3,7-16,18]. Cardiopulmonary resuscitation was commenced in two cases, including the current case, with recovery to baseline cardiovascular parameters in all other cases [12].
No cases reported any significant adverse complications postoperatively. In only one case, the patient was admitted for observation and discharged after a protracted period, though the exact reasons for continued admission for two weeks postoperatively were not documented [12]. Table 3 provides a summary of patient and operative characteristics of reported cases and outcomes.
Discussion
The TCR is a brainstem reflex resulting from stimulation of trigeminal afferents, manifesting as bradycardia or asystole, reduction in peripheral vascular tone, and apnea. The reflex is thought to be mediated via an interaction between stimulated trigeminal afferents and both sympathetic and parasympathetic outflow at the level of the midbrain (Figure 2) [4]. The current review aimed to assess the characteristics of the TCR in orthognathic surgery.
Afferent and efferent pathways of the TCRsTrigeminal afferents via the ophthalmic, maxillary, and mandibular divisions signal to the sensory nucleus of the trigeminal nerve (blue nucleus) through the Gasserian ganglion. The trigeminal sensory ganglion communicates through short internuncial fibers to the reticular formation (red arrow), and thence to the motor nucleus of the vagus nerve (red nucleus). Stimulation of the parasympathetic nerve coordinates bradycardia and gastric hypermobility. Sympathetic inhibition, via a poorly characterized mechanism (green nucleus), is thought to account for the profound drop in peripheral vascular tone and apnea observed during the reflex.TCR: trigeminocardiac reflexImage credits: Authors
This systematic review identified a small number of reported cases of TCR occurring during orthognathic surgery. This reflects the rarity of the phenomenon in the context of elective maxillofacial procedures. In total, 17 previously published cases were identified, in addition to the case presented in this review, spanning a wide age range and including both male and female patients undergoing a variety of procedures. Although the absolute number of reported cases is small, the reflex manifested in several instances as profound bradycardia or transient asystole, often occurring abruptly. Importantly, all reported cases, including the current case, resolved with prompt recognition and management, and no adverse long-term outcomes were documented.
The clinical manifestations ranged from transient bradycardia to complete ventricular asystole, with reported durations varying from a few seconds to twenty seconds in the present case. Despite the severity of some episodes, hemodynamic recovery was rapid following cessation of the stimulus, often supplemented by anticholinergic administration. Only two reported cases (including the current case) required cardiopulmonary resuscitation, with all procedures ultimately completed. An additional feature supporting the unpredictability and heterogeneity of this reflex is the timing during orthognathic surgery. While the majority of cases reported an obvious inciting stimulus, both Baronos et al. [10] and Miyamoto et al. [12] describe the onset of bradycardia post-completion of an uneventful osteotomy, during either closure or positioning of a bite block, suggesting that prior stimulation of the trigeminal nerve may contribute to sensitization to subsequent, relatively innocuous stimuli. Further, both in the current case and in the identified cases, there were no obvious changes in heart rate variability or physiology prior to the index event that may have been useful as a proxy to identify the likelihood of TCR occurrence.
The findings of this review are consistent with the observations reported by Precious and Skulsky in their prospective study of hemodynamic changes during orthognathic surgery [19]. In their cohort, significant bradycardia was most frequently observed during maxillary downfracture associated with Le Fort I osteotomy, with the authors proposing stimulation of maxillary branches of the trigeminal nerve as the likely mechanism. Although the term TCR was not widely used at the time, the clinical features described in the article align closely with contemporary definitions of the reflex, including abrupt onset, association with surgical manipulation, and prompt resolution following cessation of the stimulus. Importantly, Precious and Skulsky demonstrated that hemodynamic changes during maxillary mobilization were often transient and reversible, and they emphasized the effectiveness of immediate interruption of the surgical maneuver as the primary management strategy. These findings reinforce that, although largely unexpected, the TCR in orthognathic surgery is typically reversible when promptly recognized and managed appropriately.
In addition to the nature of the surgical stimulus, both the method and plane of anesthesia have been proposed as potentially contributory factors influencing the likelihood of the reflex occurring. Meuwly et al. demonstrated a strong association between lighter planes of anesthesia and increased susceptibility to the reflex, suggesting that insufficient suppression of brainstem reflex pathways may lower the threshold for activation [20]. With increasing reliance on and reliability of intraoperative depth of anesthesia monitoring, this relationship is of particular relevance to contemporary orthognathic practice. Clinical observations have suggested that propofol may exert an inhibitory influence on trigeminal reflex pathways, leading to speculation that TIVA could reduce the likelihood of the reflex compared with inhalational agents such as sevoflurane, particularly during procedures involving profound trigeminal stimulation such as a Le Fort I osteotomy, though evidence to support this observation is limited. However, cases in the present review occurred under both inhalational and intravenous techniques, and inconsistent reporting of anesthetic depth and physiological parameters precludes definitive conclusions.
The potential contribution of adjunctive anesthetic agents that modulate autonomic tone also warrants consideration. Remifentanil, a short-acting opioid widely used in orthognathic surgery, is known to increase parasympathetic activity and vagal tone. This, in effect, predisposes patients to bradycardia [20]. Clonidine, a centrally acting α2-adrenergic agonist, reduces sympathetic outflow and has been shown to enhance parasympathetic cardiac activity beyond its sedative and analgesic effects [21]. When administered in combination, remifentanil and clonidine may have a synergistic parasympathomimetic effect, potentially lowering the threshold for activation of vagally mediated reflexes such as the TCR. In the present case, the concurrent use of both agents may therefore have contributed to the severity of the observed response, although causality cannot be inferred from this single case.
Further to this, neither remifentanil nor clonidine should be regarded as independent precipitants of the reflex, and both agents are widely and safely used in anesthesia for maxillofacial procedures. Based on known autonomic physiology, rather, their combined autonomic effects may be clinically relevant in the presence of a strong trigeminal stimulus, especially when other permissive factors such as light anesthesia are present concurrently. At present, there is insufficient clinical evidence to support modification of standard anesthetic practice solely to mitigate the risk of an episode of the TCR, and indeed, causality cannot be inferred based on the identified cases presented here. Nonetheless, awareness of the potential additive vagotonic effects of these agents may assist anesthetists in anticipating and promptly managing hemodynamic instability during high-risk surgical maneuvers.
The elective nature of the discussed orthognathic surgeries and the typically young, otherwise healthy patient cohort heighten the clinical relevance of these findings. Episodes of severe bradycardia or asystole in this setting are unexpected and may cause significant intraoperative disruption if not promptly addressed. The consistent resolution of events following immediate cessation of surgical stimulation underscores the importance of close communication between surgeon and anesthetist, particularly during high-risk maneuvers such as maxillary mobilization. Anticipation and early recognition of the reflex remain central to effective management.
This review has several limitations. The available evidence is derived almost exclusively from isolated case reports or small case series, introducing publication and reporting bias. There is marked heterogeneity in terminology, diagnostic criteria, and reporting of perioperative variables, and denominator data are lacking, preventing accurate estimation of true incidence. In addition, incomplete reporting of anesthetic depth, physiological parameters, and postoperative investigations limits assessment of contributory factors. Consequently, the findings from this review should be interpreted as descriptive and hypothesis-generating rather than definitive.
Future research should focus on prospective data collection using standardized definitions of the TCR, with consistent reporting of surgical stimuli, anesthetic technique, depth of anesthesia, and autonomic responses. Such efforts would allow more accurate estimation of incidence and identification of modifiable risk factors. Until such data are available, heightened awareness, prompt recognition, and immediate interruption of the inciting stimulus remain crucial to effective management.
Conclusions
The TCR is an uncommon but clinically significant event that can occur during orthognathic surgery, most frequently precipitated by maxillary mobilization following Le Fort I osteotomy, although less forceful stimuli may also provoke the reflex. This systematic review, together with the presented case of intraoperative asystole, demonstrates that TCR can occur in young, otherwise healthy patients and may manifest as profound bradycardia or transient asystole. Importantly, all reported cases were managed successfully with prompt recognition, cessation of the inciting stimulus, and appropriate pharmacological intervention, with no documented long-term adverse outcomes.
Despite increasing recognition of TCR within craniofacial and maxillofacial surgery, the true incidence of the reflex in orthognathic procedures remains difficult to define. The available literature is limited predominantly to case reports and small case series, with substantial heterogeneity in terminology, diagnostic thresholds, anesthetic techniques, and reporting of perioperative variables. Consequently, definitive conclusions regarding patient-specific or anesthetic risk factors cannot yet be drawn. Nevertheless, the findings of this review highlight the need for heightened awareness of TCR among surgeons and anesthetists performing orthognathic surgery. Anticipation of the reflex during recognized high-risk maneuvers, careful attention to depth of anesthesia regardless of technique, close hemodynamic monitoring, and effective communication within the operative team are essential to minimize disruption and ensure patient safety. At present, no preventive strategy has been shown to reliably eliminate the risk of TCR.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A previously undescribed reflex from the eye to circulation and breathing: disappearance of the radial pulse with pressure on the eye Wien Klin Wochenschr Aschner B 15291530211908
- 2Trigeminocardiac reflex in bimaxillary orthognathic surgery: case review Med Oral Patol Oral Cir Bucal Ortiz-Peces L Álvaro-Martínez M Moreiras-SánchezÁD 0730202510.4317/medoral.27062 PMC 1222115340192110 · doi ↗ · pubmed ↗
- 3Asystole during Le Fort I osteotomy J Oral Maxillofac Surg Ragno JR Marcoot RM Taylor SE 10821083471989267727810.1016/0278-2391(89)90186-9 · doi ↗ · pubmed ↗
- 4Anesthetic influence on occurrence and treatment of the trigemino-cardiac reflex: a systematic literature review Medicine (Baltimore) Meuwly C Chowdhury T Sandu N Reck M Erne P Schaller B 094201510.1097/MD.0000000000000807 PMC 460252125950688 · doi ↗ · pubmed ↗
- 5Management of the trigeminocardiac reflex: facts and own experience Neurol India Arasho B Sandu N Spiriev T Prabhakar H Schaller B 3753805720091977053510.4103/0028-3886.55577 · doi ↗ · pubmed ↗
- 6Conducting systematic reviews of association (etiology): the Joanna Briggs Institute's approach Int J Evid Based Healthc Moola S Munn Z Sears K 1631691320152626256610.1097/XEB.0000000000000064 · doi ↗ · pubmed ↗
- 7Bradycardia in maxillofacial surgery Indian J Plast Surg Aggarwal K Prasad V Singh AK 1661685320203236794010.1055/s-0040-1709918 PMC 7192689 · doi ↗ · pubmed ↗
- 8Bradycardia and the trigeminal nerve J Craniomaxillofac Surg Barnard NA Bainton R 359360181990228340110.1016/s 1010-5182(05)80056-3 · doi ↗ · pubmed ↗