Abdominal wall inflammatory myofibroblastic tumor initially misdiagnosed as leiomyoma: a rare case report
Youssef T Youssef, Mohamed Baklola, Mohamed Abdelhai Mahmoud, Mohammed R Arrabyee, Eslam Ashraf Mustafa Ibrahim, Tamer Youssef

TL;DR
A rare case of an abdominal wall tumor initially mistaken for a benign growth is reported, highlighting the challenges in diagnosis and the importance of surgery for confirmation.
Contribution
This case report adds to the limited literature on abdominal wall inflammatory myofibroblastic tumors and their diagnostic difficulties.
Findings
The tumor was initially misdiagnosed as a benign leiomyoma based on biopsy.
Complete surgical excision confirmed the diagnosis of inflammatory myofibroblastic tumor.
The patient had an uneventful recovery but requires follow-up due to recurrence risk.
Abstract
Inflammatory myofibroblastic tumor is a rare mesenchymal neoplasm that most commonly arises in the lung and intra-abdominal soft tissues. Involvement of the anterior abdominal wall is exceptionally uncommon and can lead to diagnostic difficulty. We report a case of a 34-year-old male who presented with a painless, enlarging supraumbilical mass. Imaging demonstrated a heterogeneously enhancing lesion with intra-abdominal extension and close proximity to bowel loops. Core needle biopsy suggested a benign spindle cell tumor consistent with leiomyoma. Due to diagnostic uncertainty, complete surgical excision was performed. Final histopathology confirmed inflammatory myofibroblastic tumor with clear margins. The postoperative course was uneventful, and follow-up was arranged because of the risk of recurrence. This case highlights the diagnostic challenges of abdominal wall inflammatory…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
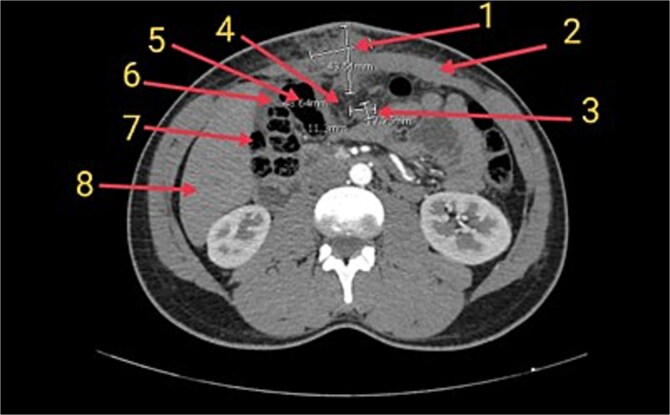 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIgG4-Related and Inflammatory Diseases · Soft tissue tumor case studies · Infectious Disease Case Reports and Treatments
Introduction
Inflammatory myofibroblastic tumor is an uncommon spindle cell neoplasm characterized by myofibroblastic proliferation with associated chronic inflammatory infiltrates [1]. Although originally described in the lung, it has been reported in various extrapulmonary sites, including the mesentery and retroperitoneum [1]. Primary involvement of the anterior abdominal wall is rare and often mimics other benign or malignant soft tissue tumors [2]. Clinical presentation and imaging findings are frequently nonspecific, making preoperative diagnosis difficult [3]. Surgical excision remains the mainstay of management and is often required to establish a definitive diagnosis [2]. We present a rare case of abdominal wall inflammatory myofibroblastic tumor initially misdiagnosed as leiomyoma on biopsy.
Case presentation
A 34-year-old male with a history of smoking and no prior surgery presented with a painless, progressively enlarging supraumbilical abdominal wall mass of two months’ duration. He reported no systemic or gastrointestinal symptoms, and physical examination showed no signs of inflammation.
Ultrasonography revealed a heterogeneous supraumbilical lesion extending intramuscularly and into the intra-abdominal cavity, measuring up to 6 cm, with surrounding edema and increased vascularity. MRI demonstrated an ill-defined, heterogeneously enhancing mass measuring approximately 5.2 × 5 cm, with low T1 and intermediate-to-high T2 signal intensity, associated fat stranding, and close proximity to adjacent bowel loops without a clear fat plane. Contrast-enhanced computed tomography (CT) confirmed extension through the rectus sheath with inseparability from the omentum and nearby colon, raising concern for an infiltrative process (Fig. 1).
Axial CT image of the abdomen showing the inflammatory myofibroblastic tumor (1) in the supraumbilical anterior abdominal wall. The mass is closely associated with the rectus sheath (2), a presumed lymph node (3), and the greater omentum (4), which appears inseparable from the tumor. Adjacent bowel loops including the transverse colon (5), hepatic flexure (6), and ascending colon (7) are noted in close proximity. The liver is also partially visible (8) in the field.
Tru-Cut biopsy showed a spindle cell proliferation within fibrous and focally myxoid stroma, accompanied by mixed inflammatory infiltrates. Tumor cells demonstrated mild atypia and sparse mitotic activity. Immunohistochemistry was positive for smooth muscle actin, while CD34, ALK, S100, and β-catenin were negative, favoring a benign spindle cell tumor such as leiomyoma.
Given the lesion’s intra-abdominal extension and diagnostic uncertainty, surgical excision was performed. Through a supraumbilical incision, the mass was dissected from the anterior abdominal wall and separated from the transverse mesocolon. Complete excision with clear margins was achieved, and the abdominal wall was reinforced with mesh.
Gross examination revealed a firm yellow-gray mass measuring 4.5 × 2 × 1.5 cm within a larger musculo-fatty specimen. Histopathological analysis confirmed inflammatory myofibroblastic tumor, composed of myofibroblastic spindle cells with chronic inflammatory infiltrates, fibrosis, focal suppuration, and foamy histiocytes. No malignant features were identified, and all margins were tumor free. The postoperative course was uneventful, and the patient was scheduled for regular clinical and radiologic follow-up due to the risk of local recurrence.
Discussion
Inflammatory myofibroblastic tumor is a rare mesenchymal neoplasm that predominantly affects children and young adults and may arise in both pulmonary and extrapulmonary locations [1, 4]. Involvement of the anterior abdominal wall is particularly uncommon, with only limited cases reported in the literature [5–7]. This rarity contributes to diagnostic uncertainty, especially when lesions present with nonspecific clinical and radiologic features.
The etiology of inflammatory myofibroblastic tumor remains unclear, although associations with inflammatory processes, trauma, and molecular alterations such as ALK gene rearrangements have been described [8]. ALK expression is more frequently observed in pediatric and pulmonary tumors, while extrapulmonary lesions in adults are often ALK negative, as in the present case [9].
Clinically, inflammatory myofibroblastic tumors typically present as slow-growing, painless masses without systemic symptoms [10]. Imaging findings are variable and may suggest aggressive behavior when tumors demonstrate ill-defined margins, infiltration, or close association with adjacent organs [9]. In our case, the proximity to bowel loops and loss of normal fat planes raised concern for malignancy [9].
Histopathological examination is essential for diagnosis, but core needle biopsy may be misleading due to limited tissue sampling and overlap with other spindle cell neoplasms such as leiomyoma, desmoid-type fibromatosis, or low-grade sarcoma [9]. This explains the initial misdiagnosis in the present case.
Complete surgical excision with negative margins remains the treatment of choice and is associated with favorable outcomes [11]. Although inflammatory myofibroblastic tumor is generally considered a tumor of intermediate biological potential, local recurrence and rare distant metastasis have been reported, particularly in ALK-negative tumors, warranting long-term follow-up [11].
In conclusion, complete surgical excision with negative margins remains the treatment of choice for inflammatory myofibroblastic tumor and is associated with favorable outcomes. Although generally considered a tumor of intermediate biological potential, inflammatory myofibroblastic tumor may recur locally and rarely metastasize, particularly in ALK-negative cases. Long-term clinical and radiologic follow-up is therefore recommended.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Choi JH . Inflammatory Myofibroblastic tumor: an updated review. Cancers (Basel) 2025;17:1327. 10.3390/cancers 1708132740282503 PMC 12026078 · doi ↗ · pubmed ↗
- 2Ali AA, Khurshid DH, Shareef FO et al. A huge abdominal wall inflammatory myofibroblastic tumor: a report of a rare case and literature review. Cureus 2024;16:e 54795. 10.7759/cureus.5479538529455 PMC 10961601 · doi ↗ · pubmed ↗
- 3Cantera JE, Alfaro MP, Rafart DC et al. Inflammatory myofibroblastic tumours: a pictorial review. Insights Imaging 2015;6:85–96. 10.1007/s 13244-014-0370-025519466 PMC 4330239 · doi ↗ · pubmed ↗
- 4Leivaditis V, Baltagianni M, Liolis E et al. Inflammatory myofibroblastic tumor of the lung: a comprehensive narrative review of clinical and therapeutic insights. Kardiochir Torakochirurgia Pol 2025;22:32. 10.5114/kitp.2025.14851440290717 PMC 12019978 · doi ↗ · pubmed ↗
- 5Pratap A, Tiwari A, Agarwal B et al. Inflammatory myofibroblastic tumor of the abdominal wall simulating rhabdomyosarcoma: report of a case. Surg Today 2007;37:352–5. 10.1007/s 00595-006-3396-117387574 · doi ↗ · pubmed ↗
- 6Zhao JJ, Ling JQ, Fang Y et al. Intra-abdominal inflammatory myofibroblastic tumor: spontaneous regression. World J Gastroenterol: WJG 2014;20:13625. 10.3748/wjg.v 20.i 37.1362525309095 PMC 4188916 · doi ↗ · pubmed ↗
- 7Li X, Li J, Liang C et al. Case report: intra-abdominal inflammatory myofibroblastic tumor with mucinous features: a case of rapid recurrence and dissemination post-surgery. Front Oncol 2024;14:1517710.39871941 10.3389/fonc.2024.1517710 PMC 11770369 · doi ↗ · pubmed ↗
- 8Chang JC, Zhang L, Drilon AE et al. Expanding the molecular characterization of thoracic inflammatory myofibroblastic tumors beyond ALK gene rearrangements. J Thorac Oncol 2019;14:825–34. 10.1016/j.jtho.2018.12.00330550870 PMC 6486847 · doi ↗ · pubmed ↗