Evaluating Gait Quality in People with Hip Osteoarthritis During Habitual and Fast Walking Using a Trunk Inertial Measurement Unit in Clinical Settings
Jiahui Wang, Abner Sergooris, Kristoff Corten, Annick A. A. Timmermans, Benedicte Vanwanseele

TL;DR
People with hip osteoarthritis show reduced gait symmetry and stability during normal and fast walking, with limited ability to adapt, as measured by a trunk sensor in clinical settings.
Contribution
A single trunk IMU effectively captures gait impairments in hip OA patients, providing biomechanical insights beyond traditional speed-based assessments.
Findings
Hip OA patients show reduced gait symmetry and stability during habitual walking with vertical impairments.
During fast walking, hip OA patients maintain reduced step symmetry but not stability, with limited gait adaptation.
Hip OA patients exhibit constrained mediolateral gait and limited adjustments when transitioning from habitual to fast walking.
Abstract
What are the main findings? Hip osteoarthritis reduces gait symmetry and stability and shows vertical gait impairments during habitual walkingAt fast walk, hip osteoarthritis reduces step symmetry but not stability Hip osteoarthritis reduces gait symmetry and stability and shows vertical gait impairments during habitual walking At fast walk, hip osteoarthritis reduces step symmetry but not stability What are the implications of the main findings? A single trunk sensor effectively captures hip osteoarthritis gait quality in clinicsIMU-derived gait quality parameters provide additional biomechanical detail beyond speed-based clinical tests A single trunk sensor effectively captures hip osteoarthritis gait quality in clinics IMU-derived gait quality parameters provide additional biomechanical detail beyond speed-based clinical tests Hip osteoarthritis (OA) affects the entire joint…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
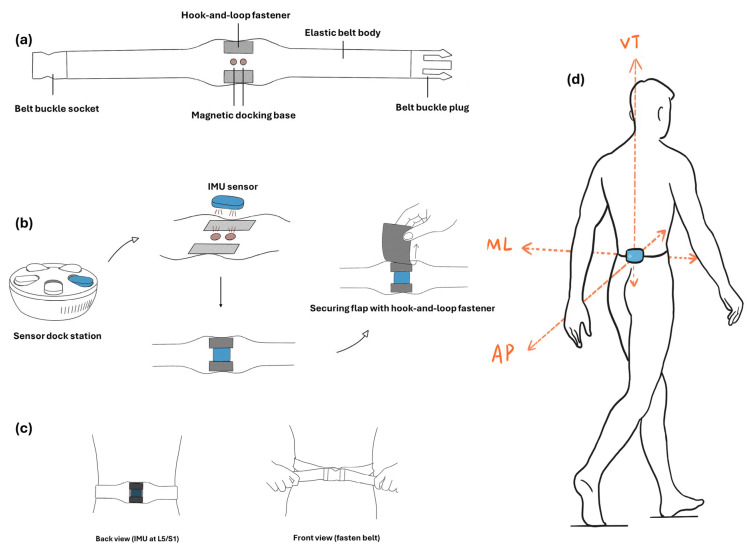 Figure 1
Figure 1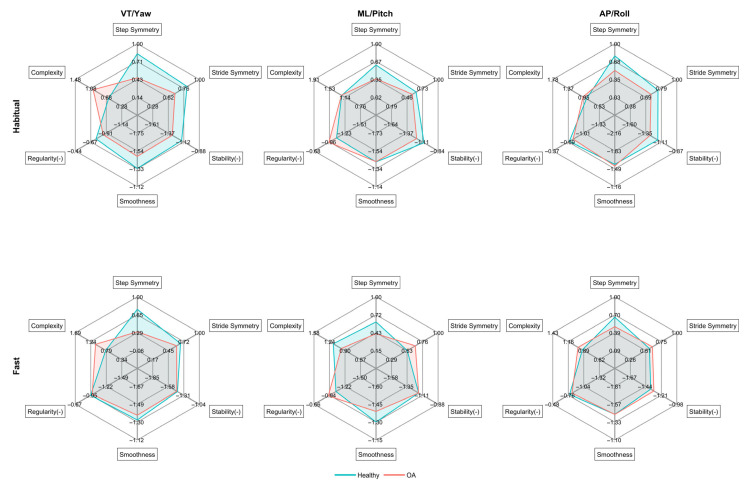 Figure 2
Figure 2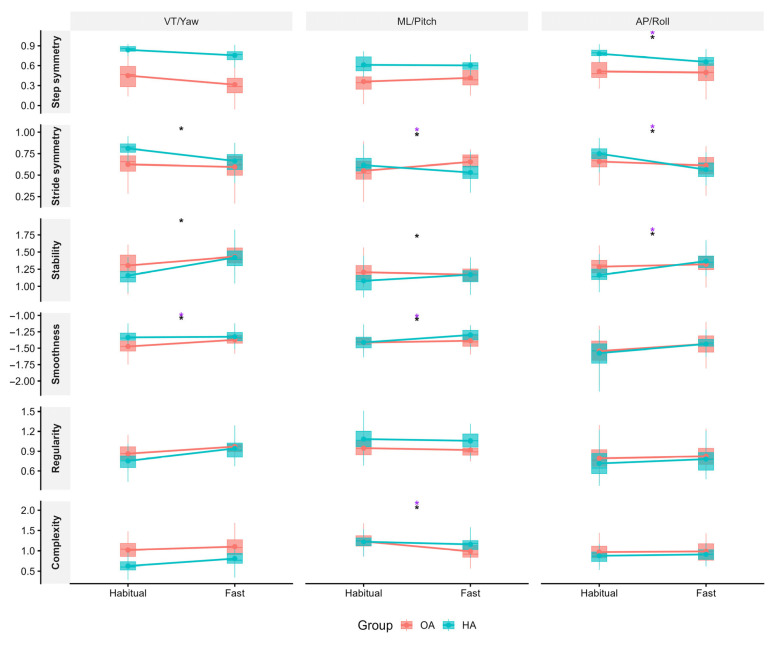 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBalance, Gait, and Falls Prevention · Osteoarthritis Treatment and Mechanisms · Prosthetics and Rehabilitation Robotics
1. Introduction
Hip osteoarthritis (OA) is an increasingly common and debilitating condition, representing a growing threat to global health [1]. From 1990 to 2019, the global incidence more than doubled from 0.74 million to 1.58 million cases, marking an increase of 115.40% [2]. It is estimated that every one in four people will likely develop symptomatic hip OA by the age of 85 [3]. Hip OA is a whole joint disorder, characterized by degenerative joint cartilage and alterations in subchondral bone, synovium, joint capsule, ligaments, and periarticular muscles. This whole joint involvement can lead to pain, stiffness, and functional limitations, making everyday activities challenging [1]. The notable effects of hip OA on mobility are primarily observed through significant changes in gait [4]. This emphasizes the need to explore how hip OA specifically impacts gait, a critical element of daily mobility.
Previous research indicated that individuals with hip OA typically have a shorter step length and walk 26% slower than healthy individuals [4]. Due to their limited hip range of motion, individuals with hip OA tend to exhibit a faster cadence and reduced step length to maintain pace [5]. Additionally, these persons adopt strategies such as a larger step width and a shorter single support phase to reduce pain and loading on the affected joint [4,6]. While these adaptations can reduce discomfort in the short term, they also lead to increased gait asymmetry over time, affecting both the affected and unaffected leg [6]. These modifications in gait parameters illustrate the considerable challenges faced by individuals with hip OA in maintaining normal gait locomotion.
Current methods for assessing gait in persons with hip OA predominantly rely on lab-based equipment, which presents significant limitations for use in clinical settings due to its complex setup and the need for specialized environments [7]. In contrast, clinical settings often utilize performance-based assessments such as the 40-m Fast Paced Walk Test (40m FPWT) as a more practical and highly reliable alternative for assessing walking function in patients with hip OA [8]. However, these tests lack detailed biomechanical insights that are critical for a more comprehensive analysis. Additionally, they may not accurately reflect a person’s natural movement behavior.
In the field of gait analysis, the use of inertial measurement units (IMUs) marks a pivotal advancement [9]. IMUs offer a portable solution that captures detailed biomechanical data while preserving the natural dynamics of walking movements. These systems, which integrate accelerometers, gyroscopes, and magnetometers, have proven particularly valuable in clinical settings where traditional lab-based equipment is impractical [10]. A notable application is the use of a single trunk IMU placed at the lower trunk level, which offers an unobtrusive way to assess several characteristics of gait biomechanics [10]. Single-trunk IMU gait analysis has been widely used in various populations, including elderly subjects, children, and individuals with neurological disorders such as Parkinson’s disease and stroke, as well as musculoskeletal diseases like orthopedic conditions and lower limb amputations [11,12,13,14,15]. The use of IMUs in clinical settings has increased recently, yet their application specifically for hip OA research remains limited.
Combining a single trunk IMU system with advanced signal processing, particularly nonlinear analysis, enables detailed characterization of gait quality beyond traditional measures [16], which is particularly relevant in individuals with hip OA. Symmetry metrics have been successfully used to detect differences between hip OA and healthy controls [12] and are also sensitive enough to identify subclinical gait alterations in pre-manifest Huntington’s disease carriers [17]. Gait instability, particularly in the mediolateral (ML) direction, has been reported in hip and knee OA [12], in Anterior Cruciate Ligament (ACL)-deficient, and ACL-reconstructed individuals [18,19]. Smoothness has shown sensitivity to aging-related gait changes and to early alterations in populations with central nervous system dysfunctions, such as multiple sclerosis [20]. Although not yet widely applied in hip OA, it may capture subtle disruptions in movement coordination due to pain-related compensations. Regularity is associated with impaired motor control and increased fall risk in populations with ACL reconstruction [19,21,22]. Lower complexity has been linked to higher fall risk in older adults [23,24]. Despite the clinical potential of these metrics, most existing studies have focused on a limited subset, typically in controlled environments and at a single walking speed. This study addresses these gaps by applying a full multidimensional gait analysis across multiple walking conditions to better understand functional deficits in OA and identify sensitive markers that could enhance current clinical evaluations.
Therefore, this study aimed to investigate (1) whether gait quality differs between persons with hip OA and healthy controls during habitual walking and fast walking, and (2) whether transitioning from habitual walking to fast walking induces different changes in gait quality between people with hip OA and healthy controls.
2. Materials and Methods
2.1. Study Design and Study Sample
This study included 40 persons with hip OA awaiting total hip arthroplasty surgery, who were included in a larger prospective longitudinal cohort study conducted at Hasselt University [25]. Ethical approval for this cohort was obtained from the medical ethics committee of Hospital East-Limburg and Hasselt University (B3712021000002). All participants were included based on a confirmed clinical or radiographic diagnosis of hip OA. Exclusion criteria included rheumatic diseases other than OA, avascular necrosis or other conditions explaining symptoms, significant neurological disorders (e.g., Parkinson’s disease, dementia), revision THA, history of pathological fractures, or planned surgeries in the one-year follow-up period. All assessments for the experimental group took place at Hospital East-Limburg in Genk, Belgium. Separate ethical approval was obtained for the healthy control group from the Ethics Committee Research (EC Research) UZ/KU Leuven (s68645). The control group was comprised of 40 age-matched healthy individuals who met the following criteria: aged 50 and above, Body Mass Index (BMI) under 30, the ability to walk 10 m unaided, and the capability to ascend and descend stairs. Exclusion criteria group were pain in the lower limbs, lower leg injuries, severe health conditions like heart failure or uncontrolled hypertension, recent major lower extremity surgeries, severe mobility impairments, or significant cognitive impairments. All exclusion criteria were assessed in person during a pre-measurement screening conducted prior to data collection and before obtaining written informed consent. Each exclusion criterion was systematically reviewed through a structured interview with participants. Cognitive status was assessed by confirming the absence of a self-reported diagnosis of cognitive or neurological impairment and by verifying the participant’s ability to understand study instructions and provide informed consent. Participants who did not meet the eligibility criteria were excluded. The control group performed all assessments in an indoor sporting hall (Building De Nayer, Leuven, Belgium). They completed the entire assessment twice, one week apart. For the main group-level analyses, only the first session was included for both groups. The second session for healthy participants was analyzed separately for reproducibility assessment and was not incorporated into the primary analyses.
2.2. Data Acquisition
At the start of the assessments, a single trunk IMU (Byteflies, Antwerp, Belgium; 200Hz, 16-bit, ACC: ±8 g; GYR: ±1000 degrees/s, 6.3 g) was attached to the lower back of each participant and recordings continued throughout the entire measurement. The IMU was secured using a customized waist belt designed for this study (Figure 1a). Embedded magnets precisely matched the sensor’s shape, ensuring a firm magnetic attachment that prevented rotation and positional changes. An additional fabric overlay further secured the sensor, eliminating the risk of accidental detachment (Figure 1b). The belt was tailored to follow the waist contour, and the belt length could be adjusted to accommodate different waist sizes, ensuring consistent positioning, minimal belt tension variation, and reducing potential movement artifacts (Figure 1c). Finally, the IMU was positioned at the L5/S1 level (Figure 1d). For the OA group, gait data were collected during a dedicated test session carried out by physiotherapists. Participants first performed the 40 m FPWT, in which they walked back and forth at maximal speed over a 10-m stretch marked by cones, completing four laps for a total of 40 m [8]. They then walked directly without additional instructions to a stair climbing task. On the way between test stations, they traversed a fixed 25-m straight indoor walkway. During this segment, habitual walking was captured. For the healthy control group, participants performed the same 40 m FPWT and also traversed a 25-m straight indoor walkway between test stations while wearing the IMU throughout the session, allowing extraction of habitual walking directly comparable to the OA group. Both cohorts completed the same assessment protocol in the same fixed order.
2.3. Data Processing
First, the sensor axis system was aligned to the global coordinate system, applying the triangulation method proposed by Moe-Nilssen et al. for tilt corrections [26]. Subsequently, segments of the fast and habitual walking signals were extracted, excluding parts of the data where participants turned, creating a continuous and stable time series from steady walking segments.
Step events were derived from the anteroposterior (AP) trunk acceleration signal using an automatic peak-detection approach based on the methodology of Zijlstra and Hof [27]. Characteristic peaks in the AP acceleration waveform were associated with successive step events, with each peak corresponding to one step. A stride was defined as two consecutive steps. In rare cases of gait asymmetry, two successive AP acceleration peaks occurred in close temporal proximity, causing the automatic peak-detection algorithm to identify only a single peak and thus missing one step. In these cases, manual inspection of the AP acceleration signal was performed to identify and add the missing step based on the presence and timing of the closely spaced AP peaks.
Afterward, the left and right steps were defined by the slope of the angular velocity around the vertical (VT) axis (yaw angular velocity). During walking, the sign of the yaw angular velocity was used to classify steps as left or right. No manual correction of step laterality was required.
All trials were visually checked to ensure accuracy. All visual inspections and manual corrections were performed by a single trained assessor following predefined criteria. In rare cases where pauses or interruptions occurred, these segments were manually excluded. The least number of strides observed among participants was 18, so the signal length of all participants was truncated to this number (±3600 data points).
2.4. Gait Quality Parameters
Gait quality was defined by six parameters: step symmetry, stride symmetry, stability, regularity, complexity, and smoothness.
Step and stride symmetry were assessed using autocorrelation to evaluate the similarity between the original signal and its one- and two-step delayed versions [17]. For step symmetry, the analysis considered the absolute value of the first dominant peak. Similarly, the second dominant peak represents stride symmetry. In both cases, the autocorrelation coefficient closer to 1 indicates higher symmetry.
Stability was quantified using the maximum Lyapunov exponent, which represents “the average exponential rate of divergence or convergence of nearby trajectories in state space” [28]. We implemented the Rosenstein algorithm [29], extended to multiple neighbors following Mehdizadeh [30]. The entire gait signal was resampled to a length of (number of strides × 200) data points, based on the sensor’s sampling frequency (200 Hz) and approximately 200 samples per stride (≈1 s). This resampling was applied once to the whole signal to preserve stride structure while normalizing length across participants. State-space reconstruction used embedding dimensions of 5 and time delay of 10. For each reference point, the 7 nearest neighbors were identified, excluding points within ±0.5 stride periods to avoid temporal correlation. The Euclidean distances between trajectories were tracked over a 10-stride window. Higher Lyapunov exponent values reflect faster divergence and thus lower dynamic stability, suggesting greater instability and an increased risk of falling.
Regularity and complexity were utilized by two related entropy measures. Regularity was measured by Sample Entropy (SaEn), quantifying the unpredictability in a signal [24]. We used the embedding dimension of 2 and a tolerance set to 0.2 times the time-series standard deviation, with the time-series length N matched that used in stability analysis. SaEn values ranged from nearly zero (high regularity) to infinite (low regularity). Complexity was measured using Multiscale Entropy (MSE) by generating multiple new time series from the original [31]. This process involves dividing the original series into non-overlapping windows, averaging the data within each window, and calculating SaEn for both the average series and the original. MSE was evaluated across 6 scales with higher MSE indicating greater complexity.
Gait smoothness was quantified using the Spectral Arc-Length Metric (SPARC), a robust, validated measure for gait analyses [22]. Angular velocity data (yaw, pitch, roll) were Fourier transformed to a frequency spectrum, then normalized to the spectrum’s maximum value for across-sample comparability. We used a 10 Hz cut-off frequency and an amplitude threshold set to 0.05 to determine the significant frequency components contributing to movement smoothness. SPARC was calculated by measuring the normalized arc length of this spectrum up to 10 Hz. SPARC values are conventionally reported as negative, smaller absolute values indicate smoother gait.
For visualization in the spider plots, sample entropy and the maximum Lyapunov exponent were inverted so that higher values correspond to greater regularity and stability, while tables report the original, non-transformed values.
All data processing was performed using MATLAB R2024b (MathWorks, Natick, MA, USA).
2.5. Statistical Analysis
The Intraclass Correlation Coefficient (ICC (3,1)) was calculated to assess test–retest consistency in healthy controls. All model assumptions (normality and homoscedasticity of residuals) were first assessed using visual inspection of Q–Q plots and residuals versus fitted plots.
To compare gait quality during habitual and fast walking between individuals with OA and healthy controls, each gait outcome was analyzed separately using linear regression including Group (OA vs healthy) as the predictor. To account for potential confounding by sex, all models were additionally adjusted for gender. We also adjusted for differences in speed by using Group as a fixed factor and Speed as a covariate alongside Group and gender.
To examine whether gait adaptations from habitual to fast pace differed between groups, linear mixed-effects models were fitted with Group (OA vs healthy), Condition (fast pace vs habitual pace), their interaction as fixed effects, and Participant as a random intercept to account for repeated measures. Walking speed was included as a covariate in the speed-adjusted analysis and gender was adjusted in all models.
For all analyses, p-values were adjusted for multiple comparisons using the Benjamini–Hochberg false discovery rate procedure. Statistical significance was set at p < 0.05. All analyses were conducted in R (version 4.4.1) using RStudio (version 2023.6.0.421, RStudio, Inc.).
3. Results
All gait-quality parameters demonstrated good to excellent test–retest reliability (Supplementary Table S1).
Subject characteristics are shown in Table 1. BMI was significantly higher in persons with hip OA and in their age-matched healthy controls. During both habitual and fast walking, persons with hip OA walked significantly slower. For both groups, walking speed at fast pace was significantly higher than at habitual pace.
Several gait quality parameters were different between persons with hip OA and age-matched healthy controls during habitual and fast walking (Figure 2). During habitual walking, persons with hip OA exhibited reduced step and stride symmetry in all three directions, indicating notable gait asymmetry (Table 2). Gait stability was also significantly reduced in persons with hip OA compared to healthy individuals. Moreover, persons with hip OA walked with lower regularity and higher complexity in the VT direction, along with higher regularity in the ML direction. In addition, persons with hip OA walked with less smoothness in yaw rotational motion. After adjusting for walking speed, most group differences were no longer significant. Only step symmetry in the ML direction remained significantly lower in persons with hip OA during habitual walking, suggesting this parameter reflects gait impairment beyond the influence of speed.
During fast walking, persons with hip OA showed lower step symmetry in all three directions. There were no significant differences in gait stability between persons with hip OA and healthy controls at fast walking. Persons with hip OA showed greater stride symmetry, increased regularity, and decreased complexity compared to healthy controls, along with higher complexity in the VT direction. In addition, persons with hip OA walked with less smoothness in yaw rotational motion. After adjusting for walking speed, step symmetry remained significantly lower in the OA group for all three directions. All significant differences in the ML direction remained. In the VT direction, complexity differences remained, while additional significant differences emerged, including lower stride symmetry and reduced yaw smoothness in persons with hip OA.
Significant interaction effects between Group (OA vs. healthy) and Condition (habitual vs. fast pace) were observed for several gait measures (Figure 3). For step symmetry, interaction effects were found in the AP direction. Stride symmetry and gait stability showed interaction effects across all three directions (VT, ML, and AP). Gait smoothness showed interaction effects in yaw and roll. For gait complexity, interaction effects were found in the ML direction. No interaction effects were observed for gait regularity in any direction. When walking speed was included as a covariate, significant interactions remained for AP step symmetry, ML and AP stride symmetry, yaw and roll smoothness, AP stability, and ML complexity.
4. Discussion
Based on this study’s findings, persons with hip OA walk significantly differently at their habitual pace compared to age-matched healthy controls, exhibiting less step and stride symmetry and lower gait stability across all three directions, with VT impairments present across all gait quality parameters. However, most of these differences were no longer significant after adjusting for walking speed. In contrast, during fast walking, hip OA showed lower step symmetry, but the stability of persons with hip OA did not differ from healthy individuals. Additionally, when transitioning to faster speeds, OA and control groups demonstrated different adjustment in gait quality. By examining six gait domains under two independent conditions, this study provides detailed biomechanical data on gait in hip OA, contributing to a more comprehensive understanding of disease-related gait alterations for clinical and research applications.
Persons with hip OA showed lower step and stride symmetry in all three directions compared to healthy people during habitual walking, which is consistent with earlier research findings [4,12]. All 40 participants in this study had unilateral end-stage hip OA, which typically results from degenerative changes that unevenly affect two sides of the hip joints, leading to asymmetries [32]. Rather than representing a mere deviation from normal gait, this asymmetry likely arises from pain, muscle weakness, and other sensorimotor deficits in the more affected limb, and may function as a compensatory adaptation to reduce mechanical load and mitigate pain on the affected side [33].
Persons with hip OA showed less stable gait across all directions during habitual walking. This aligns with existing literature, which consistently points to end-stage hip OA as a significant factor that markedly deteriorates overall stability and increases the risk of falls [34,35]. Laboratory studies further support this, showing impaired stability and elevated fall-risk indices even in mild to moderate disease [36]. In addition, individuals with unilateral hip OA performed worse on standardized functional and clinical stability measures such as the Berg Balance Scale and the Timed Up and Go test [37]. Consistently, nearly half of older adults with hip OA report at least one fall per year [38,39]. In contrast, some studies have reported no differences in gait stability between individuals with hip OA and healthy controls [12,40]. These studies were conducted under different conditions, such as walking 10 m in a laboratory at self-selected speed or with treadmill walking at controlled speeds and included participants with moderate rather than end-stage disease. Variations in experiment settings and disease stage may explain the different findings, as impairments in stability might be more apparent during habitual walking in individuals with end-stage hip OA.
Persons with hip OA walked with less regularity and higher complexity, together with reduced symmetry and stability in the VT. This aligns with previous studies demonstrating impairments in the VT direction in hip OA, reporting significantly lower step regularity [12,41]. Laboratory-based studies also indicated altered vertical loading patterns in hip OA, providing complementary evidence of gait differences in the vertical direction [42,43]. In addition, musculoskeletal modeling suggested disproportionate contributions of the gluteus maximus to the vertical center of mass acceleration in hip OA [44]. Our study complements this knowledge by showing that, during habitual walking, all domains of vertical gait quality are consistently impaired.
During fast walking, persons with OA continued to show marked gait asymmetry across all three directions. Interestingly, stability no longer differed between groups at fast walking. This suggests that OA persons were able to adapt by preserving stability under high demand, but they did so at the expense of other gait qualities mainly in the ML direction. Persons with OA showed greater regularity, higher stride symmetry, and lower complexity in the ML direction, indicating a more constrained and rigid gait movement. This is consistent with earlier research findings that persons with hip OA often display frontal-plane sideways compensations such as trunk lean and altered hip adduction moments as strategies to control stability [45]. These findings suggest that hip OA may alter ML gait movement in a way that may help preserve stability but results in more constrained movement during fast walking.
During both habitual and maximum speed walking, individuals with hip OA walked significantly slower than healthy controls. Although walking speed is a strong determinant of many gait parameters, it also reflects pain, functional limitation, and adaptive motor strategies that are intrinsic to the disease process. Therefore, both unadjusted as well as adjusted results are important as adjustment for walking speed may attenuate clinically meaningful between-group gait differences but can help to explore the extent to which observed impairments are velocity-dependent. After speed-adjustment, most group differences were no longer significant during the habitual walking, indicating that poorer gait quality in OA could be associated with persons slower habitual walking speed. Only ML step symmetry remained impaired, reflecting a gait deficit independent of speed. These results should be interpreted carefully as this does not mean that gait quality could simply be improved if individuals with OA walked faster as healthy persons. Although they were able to increase speed when explicitly instructed, transitioning to their fast walking revealed persistent and even greater asymmetry as well as some additional abnormalities in the ML and VT direction. These findings suggest that when challenged to walk closer to their physical limits, individuals with OA exhibit intrinsic gait control deficits that cannot be explained solely by slower speed. Moreover, in daily life, individuals with OA generally adopt slower self-selected speeds, likely due to pain, joint restriction, or fear of instability, and at these speeds they do exhibit less symmetrical and less stable gait. Overall, the results indicate that while some gait quality parameters in OA might be speed-dependent, there are impaired gait quality parameters representing disease-specific deficits that persist across walking speeds.
When comparing habitual with fast walking, differences between OA and healthy controls were found in the AP direction for step symmetry, stride symmetry, and stability, even correcting for speed. Post hoc contrasts showed that healthy adults exhibited significant decreases in AP step and stride symmetry and less stability when transitioning from habitual to fast walking, whereas the OA group did not change in any of these measures. These results are consistent with previous studies demonstrating comparable declines in dynamic stability and gait symmetry among healthy adults when speed increases [46,47]. In contrast, individuals with hip OA showed no significant change in AP symmetry or stability when transitioning to fast walking. This might be due to the fact that OA individuals’ stability and symmetry at habitual walking were already comparable to the reduced levels observed in healthy individuals during fast walking. In other words, OA individuals operate at a lower baseline of AP stability and symmetry at habitual speeds, and unlike healthy adults, they do not adapt further when challenged by speed demands. This pattern reflects a potential limitation in their adaptive capacity in the AP direction and may indicate underlying impairments in AP control. Supporting this interpretation, previous studies demonstrated that individuals with hip OA exhibit diminished hip-generated forward propulsion as well as reduced ankle push-off power and overall propulsive force compared to healthy adults [48,49].
Our study has several limitations that should be considered when interpreting the results. Notably, there was a significant difference in BMI between the healthy and OA groups. As increased BMI is associated with the development and progression of OA [50], recruiting BMI-matched healthy controls is challenging. Additionally, the healthy participants recruited for this study were particularly fit and free from pain to minimize the influence of pain on gait patterns, characteristics that may not be typical of the general population of similar age. This discrepancy in physical condition could lead to an overestimation of the differences in gait parameters between healthy individuals and those with OA, as the healthy group’s superior physical condition might not accurately represent an average older adult. Pain severity was not included as a covariate due to the limited sample size, and physical activity was not assessed and therefore could not be accounted for. These factors suggest that while our findings provide valuable insights, they should be generalized with caution to the broader population. Further studies are needed to confirm these findings across a more representative sample of middle-aged and elderly adults.
5. Conclusions
This study found that persons with hip OA walk differently from healthy controls across multiple gait quality parameters. During habitual walking, the OA group showed less symmetry and stability, with VT impairments present across all gait quality parameters. At fast walking, hip OA individuals showed decreased step symmetry and more constrained ML movement, while their stability was at the same level as healthy controls. When transitioning from habitual to fast walking, the healthy group experienced significant reductions in AP symmetry and stability, whereas the OA group showed no changes. This study provides biomechanical data that may support both clinical assessment and future research as the findings augment the interpretation of gait data beyond traditional speed-based tests such as the 40MFW, supporting the development of more personalized treatment strategies. As there is currently no evidence on how specific gait parameters can be modified through interventions in hip OA or related populations, further research is needed to expand on these results and address the distinct gait challenges faced by individuals with hip OA.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Woolf A.D. Pfleger B. Burden of Major Musculoskeletal Conditions Bull. World Health Organ.20038164665614710506 PMC 2572542 · pubmed ↗
- 2Fu M. Zhou H. Li Y. Jin H. Liu X. Global, Regional, and National Burdens of Hip Osteoarthritis from 1990 to 2019: Estimates from the 2019 Global Burden of Disease Study Arthritis Res. Ther.202224810.1186/s 13075-021-02705-634980239 PMC 8722328 · doi ↗ · pubmed ↗
- 3Murphy L.B. Helmick C.G. Schwartz T.A. Renner J.B. Tudor G. Koch G.G. Dragomir A.D. Kalsbeek W.D. Luta G. Jordan J.M. One in Four People May Develop Symptomatic Hip Osteoarthritis in His or Her Lifetime Osteoarthr. Cartil.2010181372137910.1016/j.joca.2010.08.005PMC 299806320713163 · doi ↗ · pubmed ↗
- 4Constantinou M. Barrett R. Brown M. Mills P. Spatial-Temporal Gait Characteristics in Individuals with Hip Osteoarthritis: A Systematic Literature Review and Meta-Analysis J. Orthop. Sports Phys. Ther.20144429129710.2519/jospt.2014.463424450373 · doi ↗ · pubmed ↗
- 5Bahl J.S. Nelson M.J. Taylor M. Solomon L.B. Arnold J.B. Thewlis D. Biomechanical Changes and Recovery of Gait Function After Total Hip Arthroplasty for Osteoarthritis: A Systematic Review and Meta-Analysis Osteoarthr. Cartil.20182684786310.1016/j.joca.2018.02.89729474993 · doi ↗ · pubmed ↗
- 6Porta M. Pau M. Leban B. Deidda M. Sorrentino M. Arippa F. Marongiu G. Lower Limb Kinematics in Individuals with Hip Osteoarthritis During Gait: A Focus on Adaptative Strategies and Interlimb Symmetry Bioengineering 202184710.3390/bioengineering 804004733924515 PMC 8069064 · doi ↗ · pubmed ↗
- 7Colyer S.L. Evans M. Cosker D.P. Salo A.I.T. A Review of the Evolution of Vision-Based Motion Analysis and the Integration of Advanced Computer Vision Methods Towards Developing a Markerless System Sports Med.-Open 201842410.1186/s 40798-018-0139-y 29869300 PMC 5986692 · doi ↗ · pubmed ↗
- 8Dobson F. Hinman R.S. Roos E.M. Abbott J.H. Stratford P. Davis A.M. Buchbinder R. Snyder-Mackler L. Henrotin Y. Thumboo J. OARSI Recommended Performance-Based Tests to Assess Physical Function in People Diagnosed with Hip or Knee Osteoarthritis Osteoarthr. Cartil.2013211042105210.1016/j.joca.2013.05.00223680877 · doi ↗ · pubmed ↗