Auranofin Combination Therapy: A New Frontier in Cancer Treatment
Diana Laura Guzman-Gomez, Srinivasa Reddy Telukutla, Ruchika Ojha, Suresh K. Bhargava, Magdalena Plebanski

TL;DR
Auranofin, originally used for arthritis, shows promise as a cancer treatment that can work well with other therapies.
Contribution
The paper highlights auranofin's potential as a synergistic agent in cancer therapy and its role in overcoming drug resistance.
Findings
Auranofin inhibits thioredoxin reductase and induces reactive oxygen species in cancer cells.
It synergizes with chemotherapy, immunotherapy, and targeted therapies to enhance cancer treatment.
Auranofin shows potential in overcoming drug resistance and as an adjuvant in precision medicine.
Abstract
Auranofin, a gold(I)-based compound initially developed for the treatment of rheumatoid arthritis, has emerged as a promising anticancer agent with a multimodal mechanism of action. This review comprehensively examines the therapeutic potential of auranofin in oncology focusing on its ability to synergize with conventional and emerging cancer treatments. Here, we discuss the unique pharmacological properties of auranofin, including thioredoxin reductase inhibition, reactive oxygen species induction, and modulation of key apoptotic pathways. Moreover, this article highlights new recent evidence on its ability to synergize with other cancer treatments such as chemotherapy, immunotherapy, and targeted therapies. Particular emphasis is placed on the role of auranofin in overcoming drug resistance and its potential as an adjuvant in precision medicine. By analyzing both preclinical and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
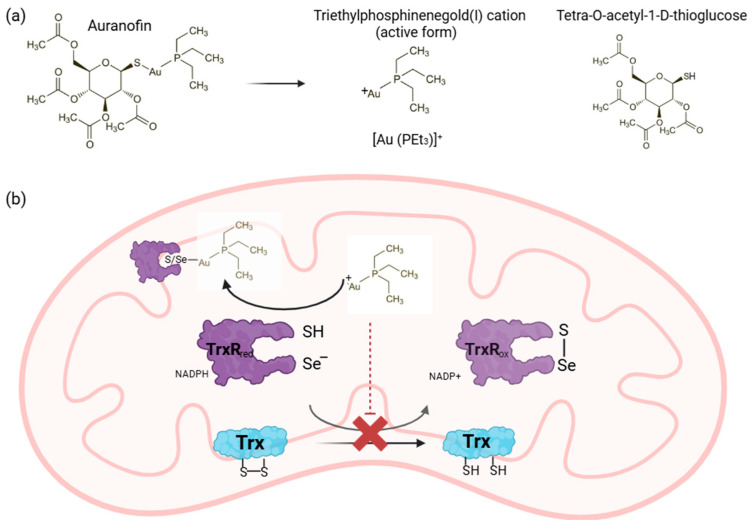 Figure 1
Figure 1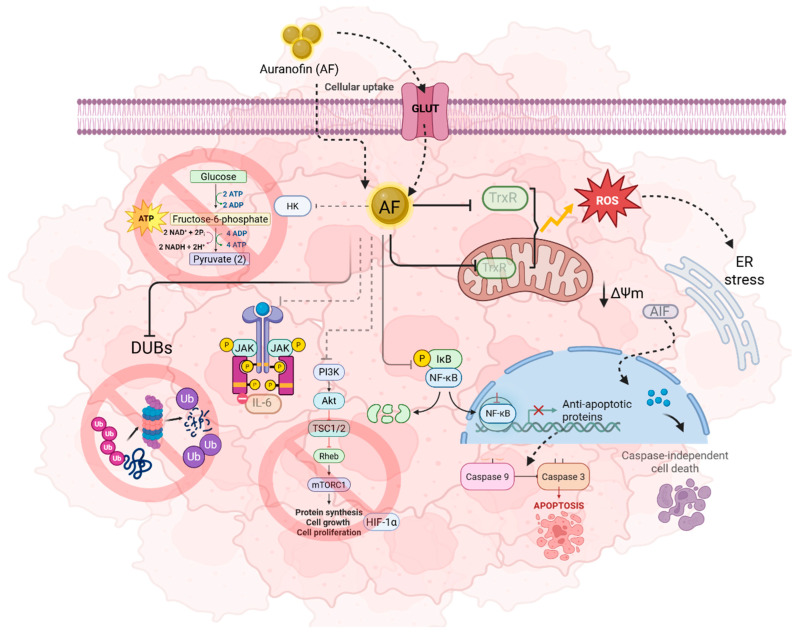 Figure 2
Figure 2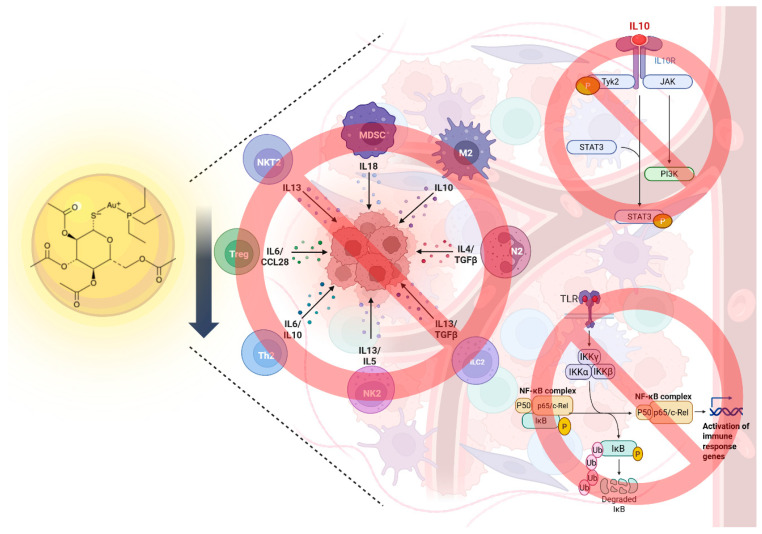 Figure 3
Figure 3- —Australia–India Strategic Research Fund
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRedox biology and oxidative stress · Ferrocene Chemistry and Applications · Ferroptosis and cancer prognosis
1. Introduction
Cancer is a group of diseases characterized by abnormal cells growing uncontrolledly forming tumors and invading surrounding and distant tissues, the latter known as metastasis. It remains one of the leading causes of death worldwide with an estimated 20 million new cases and nearly 10 million deaths in 2022 [1]. According to global cancer statistics, the most prevalent types of cancer in 2022 are lung (2.48 million cases), breast (2.29 million cases), colorectum (1.92 million) and prostate (1.46 million cases), whereas the most lethal, with 5-year survival post-diagnosis below 50%, include lung, pancreatic, liver, stomach and ovarian cancer. However, factors such as age, sex, geographic location, and socioeconomic status change the distribution of cancer around the world with different impacts and variations across populations [1,2,3,4,5].
Cancer poses a significant global health burden due to multiple factors such as lifestyle, environment, genetics and the presence and influence of specific infectious pathogens. Moreover, the lack of appropriate cancer management and palliative care in low resource settings can obstruct the progress and successful implementation of cancer treatments. Nevertheless, the disease burden might be reduced by the avoidance of risk factors, improvement of early detection techniques, and novel therapeutic approaches [2,6,7]. Current cancer therapies include surgery, chemotherapy, radiotherapy, immunotherapy, and targeted therapies, each of which changes its effectiveness depending on the type and stage of the cancer. For instance, surgery is commonly used in the early stages, but it is ineffective in the advanced stages, and the toxicity of chemotherapy and radiotherapy on normal cells becomes a limitation because it involves remarkable side effects despite being a potent treatment. In contrast, immunotherapy and targeted therapies are limited to specific conditions or cancer cell characteristics, thus limiting their utility [8].
One of the major obstacles in cancer is the recurrence or relapse of the disease accompanied by drug resistance which makes the therapy insufficient for full recovery slowing the impact of the treatment. In addition, tumor features such as heterogeneity and rapid adaptability remain paramount challenges to overcome. Therefore, the need for novel therapeutic approaches that can target cancer cells to minimize negative effects on normal tissues is important. Among the strategies used to improve the treatment effects is combination therapy, which has been broadly applied for decades due to the advantages provided by the administration of multiple therapeutic agents; for instance, the amelioration of efficacy by targeting different pathways simultaneously, the reduction in side effects by decreasing drug doses, and the attenuation of relapse and drug resistance. Hence, complementary interactions, known as synergism, are valuable for enhancing therapeutic effects in complex diseases such as cancer and controlling its progression. Moreover, this strategy coupled with a drug repurposing approach, which consists of identifying new applications for existing therapies, has recently gained momentum to accelerate the development of novel treatments in oncology, curtailing time, costs, studies, and repercussions in the long-term survival rate. In other words, given the limitations and complexity of the disease, the potential of combining novel agents or repurposed drugs with existing therapies allows the exploration of cancer from different perspectives and finding a better approach [9,10].
2. Auranofin
Gold complexes have gained relevance as potential anticancer drugs because of their antitumor activity against cancerous cells and unique mechanism of action which may be beneficial for established chemotherapies [11,12]. Auranofin (AF), a gold(I) compound initially developed for rheumatoid arthritis, is a prime example of a compound with anticancer potential across various cancer types including lung, ovarian, pancreatic, colon, hepatic and breast carcinoma [13,14]. The predominant molecular mechanism of AF is inhibition of thioredoxin reductase (TrxR), an enzyme overexpressed in aggressive tumors that is essential for maintaining cellular redox homeostasis [15]. Following administration, AF undergoes rapid ligand exchange reactions with biological thiols in the blood stream leading to displacement of thiosugar moiety and generation of pharmacologically active triethylphosphinegold(I) cation [Au(PEt_3_)]^+^ [16]. The thiosugar ligand contributes to pharmacokinetic properties and reduced systemic toxicity and is not directly responsible for the cytotoxicity, which is attributed primarily to the gold(I) cation. Cellular uptake of AF is thought to occur predominantly via glucose transporters, owing to its thiosugar ligand, and passive diffusion attributable to its hydrophobic character. Following the internalization, the released triethylphosphinenegold(I) cation [Au (PEt_3_)]^+^, targets redox-active selenocysteine residue located in C-terminal active site of TrxR. Nucleophilic attack of selenolate on the gold(I) center results in the formation of a stable Au-Se bond leading to irreversible inhibition of the enzyme. This disrupts electron transfer from NADPH to thioredoxin leading to functional inactivation of TrxR [16,17,18,19]. Inhibition of mitochondrial and cytosolic TRXR impairs antioxidant defense systems, leading to intracellular reactive oxygen species (ROS) accumulation, cell cycle arrest, reduced cancer cell resistance and ultimately induction of cell death (Figure 1) [13,14,20].
Notably, non-specific oxidative damage may affect healthy tissues inducing DNA damage, and excessive ROS levels can activate compensatory mechanisms that promote cell survival. Likewise, TrxR is not only involved in maintaining redox balance, but it also plays a critical role in DNA synthesis, cell proliferation and apoptosis; consequently, the inhibition of this system may contribute to unpredictable therapeutic outcomes or toxicity. Furthermore, AF’s affinity to thiol groups may cause off-target interactions with other cellular systems leading to non-specific toxicity [22].
Alternative signaling pathways associated with AF’s cytotoxic role in cancer as a consequence of the disruption of redox homeostasis through irreversible inhibition of TrxR include the activation of caspase-3 and -9 enzymes that triggers apoptosis, nuclear factor-kappa B (NF-kB) signaling pathway inhibition, which is crucial in inflammation and immunity, and the prevention of the degradation of the Forkhead box O3 (FOXO3) tumor suppressor factor, which in turn can modulate cytokine production, including interleukin 6 and 1β (IL-6 and IL-1β) and tumor necrosis factor alpha (TNF-α), thereby promoting cancer cell survival. Other altered mechanisms include glycolysis by hexokinase enzyme inhibition which participates in autophagy regulation, ubiquitin-proteasome system inhibition involved in cell cycle and DNA damage regulation, and downregulation of the PI3K/AKT/mTOR pathway which produce an anti-angiogenic effect [14,20,23,24] (Figure 2).
Immunomodulation is a key focus for the development of effective cancer treatments. A reduction in immune infiltration in the tumor microenvironment (TME) has been associated with tumorigenesis, angiogenesis, metastasis and oncogenic mutations. Recent studies have suggested that AF can modulate the TME by regulating TGF-β cytokine expression, which promotes immunosuppression, while also inducing immunogenic cell death (ICD) in a dose-dependent manner [25,26]. Boullosa et al. [27] reported ICD through a significant increase in damage-associated molecular patterns (DAMPs) and mature dendritic cells (DCs) in mutant p53 lung cancer cells. Moreover, they demonstrated that some of the observed caspase-independent cell death is mediated by NK cells. In contrast, the inhibition of IkB kinase by AF modulates the activity of NF-kB, a key regulator of inflammation, tumor aggressiveness, immunosuppression and cell survival, with high levels associated with pro-inflammatory cytokines and chemokines such as IL-6, IL-1, TNF, CCL2, and CXCL12, as well as the presence of M2-polarized tumor-associated macrophages (TAMs), myeloid-derived suppressor cells (MDSCs), and Tregs (Figure 3) [23,28].
Importantly, cancer cells possess evasion strategies that limit AF’s long-term efficacy. For instance, targeting a single component of the PI3K/AKT/mTOR pathway (deregulated in cancer) can result in compensatory signaling that attenuates therapeutic efficacy [29]. Similarly, NF-κB signaling can either promote or suppress tumorigenesis depending on the microenvironment. Acute NF-κB activation during inflammation facilitates rapid immune cell recruitment and is often associated with favorable outcomes, whereas chronic activation promotes cancer cell proliferation, survival, and malignancy [30]. Therefore, understanding the complexity of these alternative pathways is critical for optimizing AF-based therapeutic strategies and minimizing off-target toxicities.
3. Potential of Auranofin Combination Therapy in Cancer Treatment
AF represents a potentially valuable adjunct to existing cancer treatment paradigms, particularly in overcoming resistance to other drugs, which is a significant obstacle in the current oncological treatments. Its ability to target multiple molecular pathways offers an opportunity to enhance the efficacy of established cancer therapies and open multimodal cancer treatment regimens for synergistic integration with chemotherapy, immunotherapy and targeted therapies [14]. In vitro and in vivo studies have demonstrated that auranofin potentiates the efficacy of chemotherapeutics, immunomodulators and targeted compounds by sensitizing current complexes and overcoming the mechanisms of drug resistance that limit the success of monotherapies [26,31].
3.1. Preclinical In Vitro Studies Auranofin Combination Therapy
Overall, preclinical studies have demonstrated that AF may be a valuable tool for cancer therapy by synergizing with other conventional drugs, leading to reduced tumor growth and enhanced efficacy (Table 1) [23]. Furthermore, the integration of AF can potentially reduce the need for high doses of single-agent treatments, boosting therapeutic outcomes and reducing off-target effects in multiple malignancies [31]. The following table summarizes some of the current in vitro combination studies on different cancer cell lines and their impact when combining auranofin with other drugs.
Potential Mechanisms of Synergistic Effects
As shown above, multiple in vitro studies have demonstrated significant synergy of auranofin when combined with various anticancer agents by exacerbating oxidative and proteotoxic stress, disrupting redox balance, and modulating tumor and immune signaling pathways in various types of cancer. One of them is L-BSO, a glutathione (GSH) inhibitor, which is highly elevated in cancer, is associated with tumor progression and drug resistance, and shows synergistic cytotoxicity by interfering with both TrxR and GSH antioxidant systems in ovarian, lung, pancreatic carcinoma, mesothelioma, and glioblastoma. Moreover, this combination exhibited lethality in both conventional drug-sensitive cancer and resistant cancer cells, decreasing viability by more than 20% above the other drug alone [32,34]. Potential mechanism of synergy includes the reduction in ROS scavenging capacity by blocking both antioxidant systems; additionally, it has been found that high levels of glutathione transferases are involved in metal detoxifications, which means that the inhibition of GSH may decrease gold efflux from cancer cells, leading to cytotoxic effects [52].
Menin is an essential oncogenic cofactor for the resulting mixed-lineage-leukemia (MLL) fusion protein in acute leukemia. Menin-MLL inhibitors have demonstrated effects against diverse types of cancer, including breast, ovarian and pancreatic cancer. According to Kato et al. [35], MI-463 and auranofin synergistically potentiate growth inhibition activities reducing viability by 80–90% in human ovarian, pancreatic, lung and breast cancer cells by inducing ferroptosis.
In HGSOC, approximately 50% of patients exhibit MYC amplification, an oncogenic transcription factor that plays a critical role in tumorigenesis and metabolism. Raninga et al. [36] found that auranofin is involved in glycolysis inhibition, resulting in a switch to glutamine metabolism for survival. To enhance the anti-neoplastic activity, they proposed the addition of a glutaminase inhibitor (CB-839), exerting a synergistic growth suppressive effect against MYC-high HGSOC cells by altering glutamine metabolism and glycolysis and oxidizing various proteins involved in proteasome, RNA transport, and the REDOX system.
Celecoxib, a nonsteroidal anti-inflammatory drug (NSAID) and sulfasalazine, a disease-modifying anti-rheumatic drug (DMARD) used to treat arthritis, have been shown to have anticancer activity due to their anti-inflammatory properties. Therefore, Han et al. and Li et al. [37,38] studied their synergistic effect in combination with AF demonstrating more than a 40% increase in cytotoxicity in colon and lung cancer cells by oxidative damage and ferroptosis respectively. Mechanistically, this combination induces severe oxidative stress, causing a disruption of glycolysis leading to ATP imbalance in cancer cells.
Nitazoxanide (NTZ), an antiprotozoal agent, has exerted anti-neoplastic activity in prostate, ovarian, colon, cervical, and lung cancer using a concentration between 25 and 45 μM by targeting 20S proteasome causing RE stress. Recent studies have demonstrated the advantage of AF and NTZ used together, to synergistically enhance their anti-proliferative and anti-migratory activities in anaplastic thyroid cancer, by inducing oxidative stress, cell cycle arrest in the phase G0/G1, autophagy and ferroptosis [39,53].
Mesupron, a second-generation serine protease inhibitor prodrug, has been recognized as the first class urokinase-type plasminogen activator inhibitor that is highly expressed in human breast cancer by regulating cell proliferation, invasion, and death. Therefore, Lee et al. [41] assessed the potential of Mesupron combined with AF to increase anticancer effects reporting about 60 to 70% of cell growth inhibition compared to the treatment with Mesupron alone, which showed only about 10% inhibition at 24 h. These studies further indicated a synergistic effect in one out of two breast cancer cell lines, by inducing PARP cleavage, mitochondrial disruption, and AKT phosphorylation inhibition. The accumulation of AF in the mitochondria combined with mitochondrial dysfunction caused by Mesupron triggers a synergistic effect on mitochondrial membrane potential depolarization, producing apoptosis mediated by caspase 3 activation [14].
ICG-001, an inhibitor of β-catenin/TCF mediated transcription, exhibits antitumor activity against a wide variety of cancer types including colon, pancreatic gastric and uveal carcinomas triggering cell cycle arrest and apoptosis. Lin et al. [40] tested the effect of AF and ICG-001 to evaluate their interactions and found that this combination produced better migration, colony formation and invasion suppression in colon cancer cell lines than treatment alone, inhibiting cell growth with moderate synergy (CI between 0.7 and 0.85). Moreover, it showed enhanced proliferation inhibition in 3D cell culture models by measuring the diameter changes in spheroids. In addition, they proposed that the mechanism of action might involve downregulation of p-STAT 3 and Bcl-xL and upregulation of cleaved-caspase 3, inducing apoptosis.
Spermidine, a polyamine, has been identified as a potential anticancer molecule due to its biological role in proliferation, angiogenesis, and inflammation suppressing hepatocellular carcinoma (HCC). Therefore, Hwangbo et al. [42] investigated the role of auranofin in combination with spermidine in HCC and showed more efficient toxicity against these cancer cells than the use of each drug alone in a synergic manner. Likewise, the proposed mechanism of action involves apoptosis via ROS accumulation and suppression of the PI3K/Akt signaling pathway.
Numerous preclinical studies have demonstrated that auranofin can synergize with conventional chemotherapies such as paclitaxel, doxorubicin, and cisplatin sensitizing their effects mainly attributed to AF’s ability to amplify oxidative stress. For instance, Wang et al. [51] reported 50% improvement in cytotoxicity, ROS accumulation, and cell apoptosis in liver cancer and melanoma when doxorubicin was incorporated with AF in both sensitive and resistant cell lines; Deepika et al. [50] demonstrated a synergic interaction between AF and paclitaxel in breast cancer cell lines promoting an increase in FOXO3 expression implicated in proliferation and apoptosis. Moreover, Natarajan et al. [49] illustrated the chemo-sensitizing properties of this combination to promote oxidative stress in breast cancer cells. Combining AF with cisplatin also enhances antineoplastic activity in urothelial, lung and ovarian carcinomas, by amplifying oxidative stress and mitochondrial disruption, making cells more vulnerable to cisplatin induced DNA damage [46,47,48].
The therapeutic landscape of oncology has evolved dramatically in recent years, moving beyond traditional cytotoxic agents to more targeted and immune-based treatments. Consequently, both strategies have been studied in combination with AF to disrupt the compensatory signaling pathways exerted by cancer cells. Boullosa et al. [45] highlighted the promising combination of AF and Olaparib, a PARP inhibitor, that plays a major role in DNA repair and genomic stability, demonstrating the improvement of treatment effectiveness via ROS-dependent apoptosis and ferroptosis in pancreatic and lung cancer cells. Additionally, kinase inhibitors such as Trametinib and Ibrutinib have explored a new window in cancer therapy, given that when combined with AF these drugs work by blocking enzyme decreasing growth signals, enhancing p38 MAPK signaling, inhibiting the MEK/ERK pathway, and inducing AIF-mediated apoptosis in a synergistic manner [43,44].
3.2. Preclinical In Vivo Studies Auranofin Combination Therapy
Similarly, combination strategies have been increasingly explored in vivo in animal models (Table 2). The following table summarizes some of the latest in vivo combination studies.
As described above, several animal model studies have confirmed the enhanced efficacy of dual treatment regimens previously shown in vitro, by inhibiting tumor growth without increasing systemic toxicity in models of lung, colon, and breast cancer. For instance, AF combined with vitamin C, Olaparib, celecoxib, ICG-001, sulfasalazine and nitazoxanide not only exhibited potent effect in vitro (Table 1), but also delayed tumor growth and metastasis in mice; these are the most promising combinations for clinical translation and confirm the mechanistic basis of synergy described by the authors including TrxR and GSH synthesis inhibition, disruption of redox homeostasis, mitochondrial dysfunction, DNA damage, cell cycle arrest, DUB system inhibition and enhanced apoptosis. Additionally, conventional chemotherapeutic drugs including cisplatin, doxorubicin and fluorouracil have shown good synergy when combined with auranofin in animal models enhancing the sensitivity and reduction in tumor growth (Table 2).
In recent years, immune check points as another therapeutic approach have been gaining importance, since upregulation of programmed death-1 receptor and ligand (PD-1/PD-L1) has been found to be a drug resistance mechanism in many types of cancer including ovarian, breast, pancreatic, colon and gastric carcinomas due to the neutralization of T cell activity [63]. Raninga et al. [63] proposed the simultaneous application of AF and an anti-PD-L1 antibody as a novel therapeutic strategy for triple-negative breast cancer sensitizing breast tumors to AF. Increased T-cell infiltration mediated by AF combined with the blockade of T-cell inactivation using PD-L1 antibodies enhances anticancer effects and reduces tumor chemoresistance, making it a promising therapeutic approach [14].
Targeted therapies such as ibrutinib, an irreversible kinase inhibitor have revealed anti-carcinogenic activity in lymphoma and leukemia by EGFR inhibition and boosting the immune response. Therefore, Hu et al. [43] tested the repercussions when combined with AF in lung xenograft models showing that this amalgamation led to 82% tumor inhibition compared to monotherapies which reduced tumor growth by approximately 60%. Likewise, VE822, a selective ATR (Ataxia-telangiectasia and Rad3-related) inhibitor, enabled complete regression of tumor xenografts when added simultaneously with auranofin, showing no significant body weight change in comparison with the control [60].
Collectively, these preclinical studies underscore the therapeutic potential of auranofin as an adjuvant therapy in combination with diverse drugs, across multiple cancer types. By targeting redox homeostasis and cellular stress responses, auranofin acts as a sensitizer to enhance the efficacy of a broad range of anticancer agents. These findings provide a strong rationale for clinical translation and further mechanistic studies to optimize combination protocols. However, the limitations of the studies summarized above should be considered. The therapeutic efficacy observed in some in vitro studies did not correlate with the results of corresponding in vivo studies. On the other hand, the absence of reported adverse effects is likely because most studies evaluated only body weight, without assessing other common toxicities. Additionally, the short duration of these studies may have contributed to the lack of observable physical symptoms. Therefore, long-term treatments are needed to properly assess the safety of the novel combinations. Moreover, a deeper understanding of the mechanisms of action of combination therapies is critical to ensure beneficial outcomes in clinical trials.
3.3. Clinical Trials
AF has been extensively supported by preclinical studies as a promising anticancerogenic drug alone or in combination with cytotoxic agents used for cancer or other types of diseases due to its established safety profile in RA and its novel supplementary mechanism of action in cancer therapy. Its translation into clinical oncology is still in phase 1 and II and ongoing trials; it is being investigated in leukemia, glioblastoma, ovarian and lung carcinoma [65]. Crucial insights into toxicity profiles, dosage optimization, progression-free survival, and safety will soon become available. Currently, four clinical trials using AF are being studied, among which two used AF as monotherapy in patients with chronic lymphocytic leukemia (CLL) (NCT01419691) and recurrent epithelial ovarian cancer (NCT01747798) without posted results. The lack of significant results may be related to the limited efficacy of AF alone at these tested doses or to the presence of mild to moderate adverse events; however, study completion suggests that the treatment was generally well tolerated and may be suitable for use as maintenance therapy [66]. Notable phase I and phase 2 trials of our interest are the combination of AF with a mTOR inhibitor, sirolimus, used in patients with ovarian cancer and subtypes of lung cancer (NCT03456700; NCT01737502), demonstrating tolerable side effects and preliminary signs of efficacy. In addition, a new protocol (CUSP9v3) has been reported to be safe against glioblastoma using a combination of nine repurposed non-oncological drugs with temozolomide including auranofin (NCT02770378). Despite early indications of tolerability and synergistic potential of AF alone or in combination, the clinical evidence remains insufficient to fully establish the therapeutic value of auranofin and guide its integration into standard cancer care [65,66,67].
Clinical data on AF are scarce, as was acknowledged in this study. Therefore, it is essential to prioritize well-designed trials that investigate other promising combinations. Given its potential to modulate the tumor microenvironment and enhance immune responses across various cancer types AF’s combination with immune checkpoint inhibitors (e.g., PD-1/PD-L1 inhibitors), chemotherapeutic agents (e.g., paclitaxel, and cisplatin) and targeted therapies (e.g., ibrutinib) require further investigation [14,23,25]. Additionally, improving targeted delivery and identifying biomarkers that can predict patient response to AF-based therapies may be explored in order to increase efficacy while reducing adverse effects [66,68].
4. Challenges for Combination Therapy
Combination therapy has become a cornerstone of cancer treatment, improving efficacy, reducing drug resistance, and offering synergistic benefits. From a mechanistic perspective, AF represents a promising candidate for combination therapy because its primary action on redox homeostasis and TrxR inhibition which may sensitize cancer cells to current chemotherapy. Furthermore, by disrupting other altered cellular pathways such as the ubiquitin-proteasome system, NF-kB and PI3K/AKT/mTOR pathways, AF can enhance antiproliferation and overcome resistance mechanisms. Additionally, its immunomodulatory properties may promote ICD providing a rationale for its synergy with immunotherapy [14,23].
Nevertheless, multiple challenges must be overcome for successful implementation, for instance co-administered drugs may compete for metabolic pathways or alter bioavailability, potentially leading to additive or synergistic toxicities. As a lipophilic compound, AF faces challenges in absorption, distribution, and systemic delivery, which may affect the effective concentration delivered to cancer cells in tumors, and interfere with the metabolism and clearance of other co-administered drugs. Combinations may exceed tolerability due to cumulative toxicity or off-target effects. Additionally, genetic, epigenetic and environmental variability among patients and cancer types may introduce unpredictable pharmacological behavior hindering effective dose optimization and therapeutic efficacy potentially resulting in inconsistent clinical outcomes [9,14].
For instance, clinical data (NCT01737502, NCT03456700) reported significant adverse events including gastrointestinal disorders (80%) such as diarrhea, nausea and vomiting, blood system disorders (75%) like anemia, and other general disorders including fatigue (65%), arthralgia (45%), and metabolic imbalances (15–20%) [65,66]. These toxicities underscore the necessity for careful evaluation and monitoring when combining AF with other drugs, as co-administration may exacerbate the severity of side effects.
The mitigation of these issues is critical to contributing positively to overall patient survival using novel approaches. One strategy is to improve targeting through multimodal delivery approaches, including nanoformulations such as liposomes, nanoparticles and dendrimers, which can overcome the conventional limitations by enhancing solubility, increasing drug concentration at target sites, prolonging drug half-life, and reducing systemic toxicity and multi-drug resistance [69,70].
Although combination therapy significantly enhances cancer treatment efficacy and addresses drug resistance, inherent challenges represent a substantial barrier to success. Therefore, overcoming these obstacles requires innovative strategies and further research to optimize safety and accessibility, maximize therapeutic benefits and minimize adverse effects.
5. Conclusions and Future Perspectives
In conclusion, innovative strategies in oncology, including the implementation of novel combination therapies, are essential to overcome the challenges in oncology. Among the emerging agents, AF, a promising antineoplastic agent, has exhibited potent sensitizing effects when combined with chemotherapeutics, targeted inhibitors, immunotherapies, and metabolic modulators in multiple preclinical models. Its mechanisms of action, including redox disruption, metabolic interference, modulation of oncogenic pathways and immunomodulation, provide a strong rationale for combination approaches that simultaneously affect the survival, proliferation, and immune evasion of cancer cells. Consequently, future research should focus on identifying optimal combination strategies, including rational pairing with agents that target complementary pathways in cancer cells. Furthermore, the development of co-delivery platforms may enhance drug accumulation, improve pharmacokinetics and mitigate drug toxicity. Additionally, personalization of treatment regimens and integration of immunomodulatory properties may expand the therapeutic window to maximize efficacy while minimizing side effects. Overall, by addressing these challenges and optimizing combination strategies, the unique mechanistic profile of AF in combination therapy has the potential to improve clinical outcomes, particularly in resistant, recurrent and advanced tumors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bray F. Laversanne M. Sung H.Y.A. Ferlay J. Siegel R.L. Soerjomataram I. Jemal A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA-Cancer J. Clin.20247422926310.3322/caac.2183438572751 · doi ↗ · pubmed ↗
- 2Schwartz S.M. Epidemiology of Cancer Clin. Chem.20247014014910.1093/clinchem/hvad 20238175589 · doi ↗ · pubmed ↗
- 3IARC Cancer Today—Data Visualization Tool Available online: https://gco.iarc.who.int/today/en/dataviz/pie?mode=cancer&group_populations=1&multiple_populations=1&show_table_pie=1&details_other=1(accessed on 27 April 2025)
- 4WHO Cancer Available online: https://www.who.int/news-room/fact-sheets/detail/cancer#:~:text=Tobacco%20use%2C%20alcohol%20consumption%2C%20unhealthy,%2D%20and%20middle%2Dincome%20countries.(accessed on 27 April 2025)
- 5ACS. American Cancer Society Cancer Types Available online: https://www.cancer.org/cancer/types.html(accessed on 20 September 2025)
- 6WHO Global Cancer Burden Growing Amidst Mounting Need for Services Available online: https://www.who.int/news/item/01-02-2024-global-cancer-burden-growing--amidst-mounting-need-for-services(accessed on 27 April 2025)
- 7Wu Z.H. Xia F.N. Lin R. Global burden of cancer and associated risk factors in 204 countries and territories, 1980–2021: A systematic analysis for the GBD 2021 J. Hematol. Oncol.20241711910.1186/s 13045-024-01640-839614359 PMC 11607901 · doi ↗ · pubmed ↗
- 8Debela D.T. Muzazu S.G.Y. Heraro K.D. Ndalama M.T. Mesele B.W. Haile D.C. Kitui S.K. Manyazewal T. New approaches and procedures for cancer treatment: Current perspectives Sage Open Med.2021911010.1177/20503121211034366 PMC 836619234408877 · doi ↗ · pubmed ↗