Development and Validation of the Intimate Partner Violence Nursing Competency Scale (IPVNCS): A Psychometric Tool to Strengthen Clinical Detection and Intervention
David Casero-Benavente, Natalia Mudarra-García, Guillermo Charneco-Salguero, Leonor Cortes García-Rodríguez, Francisco Javier García-Sánchez, José Miguel Cárdenas-Rebollo

TL;DR
This paper introduces a new tool to assess nurses' skills in handling intimate partner violence, improving detection and care for victims.
Contribution
The paper presents the development and validation of the IPVNCS, a novel psychometric scale for evaluating nursing competencies in intimate partner violence management.
Findings
The IPVNCS demonstrated excellent reliability with a Cronbach's alpha of 0.97.
The scale was validated across four dimensions: Intervention and Referral, Detection and Assessment, Documentation and Recording-keeping, and Psychosocial Support.
The final model showed satisfactory fit indices, confirming its validity and reliability for clinical use.
Abstract
Background: Intimate partner violence (IPV) represents a major public health problem in Europe, with significant physical, psychological, and social consequences. Nurses are often the first professionals capable of detecting early signs of IPV, yet they lack validated instruments to assess their clinical competency in detection, evaluation, documentation, and intervention. This study aimed to develop and validate the Intimate Partner Violence Nursing Competency Scale (IPVNCS), aligned with the Nursing Intervention Classification (NIC 6403). Methods: A cross-sectional psychometric study was conducted among registered nurses in the Community of Madrid. A 30-item Likert-type self-administered instrument (1–5 scale) was developed based on NANDA, NIC 6403, and NOC frameworks. A total of 202 nurses participated. Reliability was assessed through Cronbach’s alpha. Construct validity was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
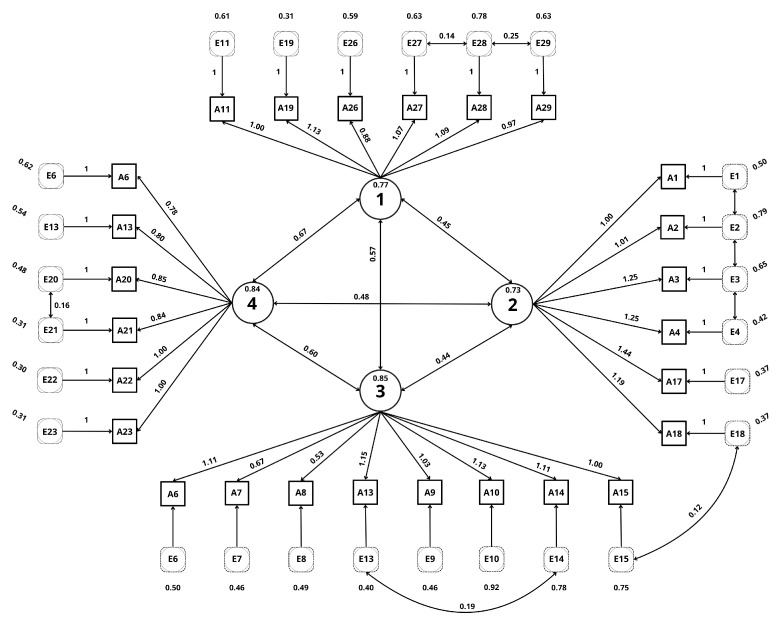 Figure 1
Figure 1- —IDIPHISA Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntimate Partner and Family Violence · Workplace Violence and Bullying · Elder Abuse and Neglect
1. Introduction
Intimate partner violence (IPV) is a critical public health issue in Europe, affecting millions of individuals each year. It includes physical, psychological, sexual, and economic abuse, with women being disproportionately affected. IPV is associated with chronic physical conditions, mental health disorders, and increased healthcare utilization. Improved detection within clinical settings is essential to mitigate these consequences.
Nurses are uniquely positioned for early identification due to their continuous proximity to patients in emergency departments, primary care, and inpatient settings. However, several barriers—including insufficient training, lack of protocols, and limited self-confidence—reduce their ability to identify and manage IPV effectively. Current literature indicates a lack of validated nursing-focused tools to assess clinical competencies regarding IPV detection, assessment, documentation, and intervention.
This study addresses this gap by developing and validating the Intimate Partner Violence Nursing Competency Scale (IPVNCS), which is grounded in NANDA diagnoses [1], NOC outcomes [2], and NIC 6403 [3] (“Abuse Protection Support: Partner”) (Table A1). The objective is to provide a psychometrically robust instrument to evaluate nurses’ perceived competency in managing IPV.
Despite advances in gender equality and efforts to eradicate the problem, it persists and manifests itself in various forms, ranging from physical to psychological and sexual violence. Women are the primary victims, although men can also suffer from it. The consequences of intimate partner violence are devastating for the physical and mental health of the victims, as well as for their social and economic well-being. It is essential to address this problem from a multidisciplinary perspective by implementing effective public policies and strengthening support systems for victims [4]. Nurses, because of their direct contact with patients, are therefore key to the early detection of intimate partner violence. However, they face challenges such as a lack of specific training and resources. Therefore, it is essential to have assessment tools that allow them to effectively identify situations of violence, make a nursing diagnosis, and provide comprehensive care to victims. Intimate partner violence (IPV) presents various factors, such as a history of child abuse [5] or low self-esteem, that increase vulnerability to this issue. Nurses must be aware of the cycle of violence and the risk factors in order to provide appropriate and personalized care.
The devastating consequences of intimate partner violence on physical and mental health make an effective response essential. Nurses, being in direct contact with the victims, are key to detecting and addressing this problem. The implementation of specific assessment instruments, the continuous training of active professionals, and university training at the degree level [6] are essential to improving the response to this public health problem. Therefore, this study aims to develop a scale with high validity and reliability. The IPVNCS does not assume that nurses are competent; rather, it aims to identify whether and in which specific domains competency gaps may exist in IPV detection and management, in order to guide targeted training and organizational interventions.
2. Materials and Methods
2.1. Study Design
A cross-sectional psychometric validation study was conducted in 2024 in the Community of Madrid. Ethical approval was granted by CEU San Pablo University (843/24/104). During the preparation of this manuscript, Perplexity Pro (Perplexity AI, Inc., 115 Sansome St, Suite 900, San Francisco, CA 94104, CA, USA) was used to improve the English language and readability of the text. The authors reviewed and edited the output and take full responsibility for the final content of the publication.
2.2. Participants and Sample
Participants were recruited through professional nursing organizations, healthcare centers, and institutional communication channels. Participation was entirely voluntary, and no incentives were offered.
A total sample of 202 participants was obtained, meeting the recommended 5–10 subjects per item for factor analysis.
2.2.1. Inclusion Criteria
Active clinical practice, an officially recognized nursing degree in Spain, and professional registration.
2.2.2. Exclusion Criteria
Exclusion criteria included retired or inactive nurses, non-accredited degrees, and nursing students.
2.3. Measuring Instrument
A 30-item Likert-type scale (1 = not competent; 5 = highly competent) was created based on:
- NANDA: Dysfunctional Family Processes (00063).
- NIC 6403: Abuse Protection Support (partner).
- NOC 2603: Family Integrity.
- Clinical guidelines for the detection and management of IPV.
The scale covered detection, assessment, psychosocial support, documentation, and referral.
2.4. Description of the IPVNCS
The Intimate Partner Violence Nursing Competency Scale (IPVNCS) is a self-administered instrument designed to assess perceived nursing competencies in the clinical management of intimate partner violence (IPV). Importantly, the IPVNCS does not assume that nurses are competent in IPV detection and intervention; rather, it aims to identify whether and in which specific domains competency gaps may exist in order to guide targeted educational, organizational, and clinical improvement strategies.
The initial version of the IPVNCS consisted of 30 items developed based on the NANDA–NOC–NIC framework, with particular alignment to NIC 6403 (“Abuse Protection Support: Partner”). Items were formulated to reflect routine nursing activities related to IPV across different clinical settings.
Each item is rated on a five-point Likert scale, ranging from 1 (“Not competent at all”) to 5 (“Highly competent”), indicating the respondent’s perceived level of competency in performing the specified activity. Completion of all items was mandatory within the electronic questionnaire, which prevented missing data.
Following exploratory and confirmatory factor analyzes, four core competency dimensions were identified:
- Detection and Assessment of Abuse: items addressing the ability to recognize physical, psychological, sexual, and social indicators of IPV and to assess risk factors. Example item: “I am able to identify clinical and behavioral indicators suggestive of intimate partner violence.”
- Documentation and Record-keeping: items related to accurate, standardized, and legally appropriate documentation of suspected or confirmed IPV cases. Example item: “I am competent in documenting suspected IPV cases using standardized clinical records.”
- Psychosocial Support: items reflecting the capacity to provide emotional support, encourage disclosure, and facilitate coping strategies for victims. Example item: “I am able to provide emotional support to patients who disclose intimate partner violence.”
- Intervention and Referral: items addressing safety planning, referral to specialized services, and coordination with multidisciplinary teams. Example item: “I am able to initiate appropriate referrals to social, legal, or specialized healthcare services for patients experiencing IPV.”
The final validated version of the IPVNCS comprised 26 items, with four items removed due to redundancy and low contribution to model fit. The complete English version of the scale is provided as Supplementary Table S1.
2.5. Data Collection
The questionnaire was distributed electronically using Microsoft Forms^TM^, and nurses could complete it at their convenience. Completion of all items was required by the platform in order to submit the questionnaire, which prevented missing data. No identifying information was collected. Data were collected between June and December 2024.
2.6. Statistical Analysis
Analyzes were conducted using SPSS 29^TM^ and AMOS 26^TM^. Reliability: Cronbach’s alpha. Construct validity:
- EFA with Promax rotation: The number of factors to be retained was determined based on a combination of eigenvalues greater than one, inspection of the scree plot, and theoretical interpretability of the factor structure. Missing data were not present, as completion of all items was mandatory within the electronic questionnaire.
- Kaiser–Meyer–Olkin (KMO) and Bartlett’s test.
- CFA using maximum likelihood estimation.
- Internal consistency was assessed using Cronbach’s alpha for both the total scale and each identified subscale.
Fit indices included /df, RMSEA, RMR, NFI, TLI, and CFI.
3. Results
3.1. Descriptive Data
The profile of the sample reveals a clear female predominance (81.7%), with a majority concentration in the 20–30 and 31–40 age groups. In terms of education, the high percentage of participants with Bachelor’s degrees and diplomas stands out, while doctorates represent a minority. Work experience is relatively evenly distributed among the different age groups, although there is a slight tendency towards those with more than 16 years of experience. With regard to the main occupation, primary care and hospital care account for most of the sample, while other areas such as teaching and social care are less represented (Table 1).
3.2. Exploratory Factor Analysis
An exploratory factor analysis with Promax rotation was conducted to identify the underlying structure of the 30 items in a sample of 202 participants. The analysis revealed a four-factor solution (Table 2). Promax rotation was selected to allow for correlations between factors, which is consistent with the multidimensional nature of the constructs assessed (Table 3). The resulting four factors exhibited high and consistent factor loadings. The IPVNCS demonstrated high internal consistency for the total scale (Cronbach’s = 0.970). Subscale reliability was also high, with Cronbach’s values ranging from 0.888 to 0.919 across the four dimensions (Table 4). The adequacy of the data for factor analysis was confirmed by the Kaiser–Meyer–Olkin index (KMO = 0.947) and Bartlett’s test of sphericity (p < 0.001) (Table 5 and Table 6). These results support the proposed factor structure of four identified dimensions: Dimension 1: Intervention and referral (items 11; 19; 26; 27; 28; 29); Dimension 2: Detection and assessment of abuse (items 1; 2; 3; 4; 16; 17); Dimension 3: Documentation and record-keeping (items 6; 7; 8; 9; 10; 13; 14; 15) and Dimension 4: Psychosocial support (items 5; 12; 20; 21; 22; 23).
3.3. Confirmatory Factor Analysis
A confirmatory factor analysis was conducted to identify the underlying structure of the variables. Two models were compared: an initial model and a final model, obtained after the elimination of items with low factor loadings and high communality. The final model showed a better fit according to /df = 2.066; Parsimony = 720.736; RMR = 0.52; RMSEA (0.073); NFI (0.86); TLI (0.91); and CFI (0.92). These results suggest that the final model provides an adequate representation of the latent structure of the data (Table 7). For this purpose, items 18, 24, 25 and 30 were removed for redundancy (Figure 1).
These removed items correspond to the initial 30-item version and are not included in the final 26-item scale presented in Supplementary Table S1.
4. Discussion
The instrument obtained from the present study demonstrates that the refinement of the initially developed scale has significantly improved its psychometric properties. This study represents an initial validation of the IPVNCS, providing evidence of construct validity through exploratory and confirmatory factor analyzes, as well as internal consistency reliability. By eliminating 4 redundant items, a superior internal consistency ( = 0.97) and a clearer factor structure have been achieved, supported by a KMO value of 0.947 and a significant Bartlett’s test of sphericity. This optimization is in line with existing literature, which emphasizes the importance of reducing redundancy to improve the accuracy and discriminant validity of scales [7]. The findings of this study may have important implications for assessing the nursing profession’s knowledge of intimate partner violence intervention. Given the scarce existence of tools for measuring professional practice, with the focus of the obtained scales being victim-oriented [8], the professional’s attitude is extremely important for managing social and health resources [9]. The refined scale allows for a more accurate assessment of the proposed dimensions, facilitating its application in clinical settings as an element of management and training of human resources, as well as part of research and undergraduate and postgraduate education. As we can see in the following study [10] on gender-based violence among healthcare students and professionals currently practicing [10], the lack of perception of this issue and the lack of knowledge about it are once again highlighted. The refined version of the scale provides an efficient tool for assessing nursing competencies related to intimate partner violence and may contribute to improving both clinical practice and care management.
For all these reasons, it is especially beneficial in clinical, research, and teaching contexts, as well as in assessing the quality of care for patients who are victims of intimate partner violence. A brief and specific scale facilitates the application and interpretation of results without sacrificing precision, allowing for the evaluation of the strengths of health professionals within the nursing field to train with precision. As we saw in the study [11], the results indicated that training to detect and how to act was deficient, along with institutional barriers to case identification: ‘lack of time in the consultation (27.2%), absence of detection protocols for case management (22.8%), saturation of health services (22.8%). Among the personal barriers to GBV were: the disinterest of health personnel in identifying cases of GBV (29.4%) [11]. With this scale, it is possible to measure the dimension affected within the nursing process (NP) and to act more specifically to solve the barriers.
To our knowledge, most existing instruments focus primarily on victims, whereas the IPVNCS addresses nursing competencies related to the comprehensive management of intimate partner violence [12] as can be seen in ‘Training should not be restricted or focused exclusively on violence against women; rather, it should be placed in the broader context of the study of gender inequalities in health and the biases arising from the lack of this perspective in both clinical practice and epidemiological research’.
Finally, these data suggest that the scale is a valid and reliable tool for assessing nursing competencies in the field of detection, intervention, and support for victims of intimate partner violence. Robust psychometric properties were obtained, allowing for an accurate and structured assessment of the skills of nurses, with positive implications for improving the care and management of intimate partner violence cases in the healthcare setting. The refinement of these items allowed for the optimization of the accuracy and relevance of the factors measured by the scale, reducing the overlap of results.
Importantly, the IPVNCS is intended as a formative and supportive tool rather than a punitive or evaluative instrument. Its primary purpose is to guide professional development and identify training needs, particularly among early-career nurses, and to support institutional strategies aimed at improving care for individuals experiencing intimate partner violence.
5. Limitations
This study has several limitations that should be considered when interpreting the results. First, the validation was conducted using a single convenience sample of nurses from the Community of Madrid, which may limit the generalizability of the findings to other geographic, cultural, or healthcare contexts. Replication studies in different regions and healthcare systems are therefore warranted.
Second, both the exploratory and confirmatory factor analyzes were performed using the same sample. While this approach is acceptable for initial scale development and refinement—particularly to assess model fit after item reduction—it may inflate model fit indices. External validation using an independent sample would provide stronger evidence for the stability of the factor structure. Internal consistency was evaluated for both the overall scale and each subscale, demonstrating good to excellent reliability. Nevertheless, further studies using independent samples are required to confirm the stability of subscale reliability and the factor structure.
Third, the IPVNCS assesses self-perceived competencies, which may be influenced by social desirability or self-assessment bias. The scale does not measure actual clinical performance, and future studies should explore associations between IPVNCS scores and objective indicators of clinical practice.
Finally, the mandatory completion of all items, while preventing missing data, may have influenced response patterns. However, this approach ensured complete datasets for psychometric analysis.
6. Conclusions
The Intimate Partner Violence Competency Scale for Nurses (IPVNCS) is a theoretically grounded instrument with demonstrated initial construct validity and excellent internal consistency reliability. It is designed to accurately assess the skills of nurses in the detection, intervention, and support of victims of intimate partner violence. Aligned with the NIC 6403 nursing intervention (Table A1), the IPVNCS allows for a comprehensive and non-discriminatory assessment. The results of the validation confirm its reliability and usefulness for clinical practice, facilitating the identification of strengths and areas for improvement in the care of victims.
7. Future Research Directions
Future research should focus on the external validation of the IPVNCS in independent samples and diverse clinical and cultural settings to confirm its reliability and validity. Longitudinal studies are also needed to evaluate the sensitivity of the IPVNCS to changes over time, particularly in the context of targeted educational or training interventions.
Additionally, qualitative studies exploring nurses’ perceptions of the IPVNCS could provide valuable insights into its usability, acceptability, and integration into routine clinical practice. Comparative studies assessing the IPVNCS alongside existing IPV-related assessment tools may further clarify its relative strengths and potential applications.
Importantly, future implementation should emphasize the formative and supportive use of the IPVNCS, avoiding its perception as a punitive or evaluative tool. The scale is intended to support professional development, particularly for early-career nurses, and to inform institutional strategies aimed at improving IPV-related care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1NANDA International Nursing Diagnoses: Definitions and Classification 2024–202613 th ed.Thieme New York, NY, USA 2024
- 2Moorhead S. Johnson M. Maas M.L. Swanson E. Nursing Outcomes Classification (NOC): Measurement of Health Outcomes 6th ed.Elsevier St. Louis, MO, USA 2018
- 3Bulechek G.M. Butcher H.K. Dochterman J.M. Wagner C.M. Nursing Interventions Classification (NIC)7th ed.Elsevier St. Louis, MO, USA 2018
- 4European Union Agency for Fundamental Rights (FRA) Violence Against Women: An EU-Wide Survey. Main Results Publications Office of the European Union Luxembourg 2014 Available online: https://fra.europa.eu/en/publication/2014/violence-against-women-eu-wide-survey-main-results-report(accessed on 14 December 2024)
- 5Uysal Yalçın S. Zonp Z. DinçS. Bilgin H. An examination of effects of intimate partner violence on children: A cross-sectional study conducted in a paediatric emergency unit in Turkey J. Nurs. Manag.2022301648165710.1111/jonm.1367335560694 · doi ↗ · pubmed ↗
- 6Ali P. Mc Garry J. Younas A. Inayat S. Watson R. Nurses’, midwives’ and students’ knowledge, attitudes and practices related to domestic violence: A cross-sectional survey J. Nurs. Manag.2022301434144410.1111/jonm.1350334734662 · doi ↗ · pubmed ↗
- 7Manuel Batista-Foguet J. Coenders G. Alonso J. Análisis factorial confirmatorio. Su utilidad en la validación de cuestionarios relacionados con la salud Med. Clín.2004122212710.1157/1305754214980156 · doi ↗ · pubmed ↗
- 8Mejia C.R. Cardona-Rivero A. Galindo V. Teves-Arccata M. Chacon J.I. Fernández-Espíndola L. Martinez-Cornejo I. Factores asociados con el machismo entre estudiantes de Medicina de ocho ciudades en cinco países Latinoamericanos Rev. Colomb. Psiquiatr.202352 S 70S 7610.1016/j.rcp.2021.09.004 · doi ↗