Impact of Previous Thoracotomy on Outcomes of Open Thoracoabdominal Aortic Aneurysm Repair: A Retrospective Propensity Score-Matched Analysis
Muhyung Heo, Siwon Oh, Suryeun Chung, Dong Seop Jeong, Wook Sung Kim, Yang Hyun Cho, Kiick Sung

TL;DR
This study finds that repeat thoracotomy for aortic aneurysm repair does not significantly worsen early surgical outcomes compared to first-time procedures.
Contribution
The study provides evidence that repeat thoracotomy for TAAA repair is not associated with worse early outcomes in experienced centers.
Findings
Repeat thoracotomy had longer operative times but similar 30-day mortality compared to first-time thoracotomy.
Postoperative bleeding was more frequent in the repeat thoracotomy group, though not statistically significant.
No cases of paraplegia occurred, and other major complications were similar between groups.
Abstract
Objectives: Open repair remains widely used for TAAA (Thoracoabdominal Aortic Aneurysm), but disease progression may require reoperation via repeat thoracotomy, which is technically challenging. These procedures involve increased risks due to adhesions and altered anatomy. This study aims to evaluate the impact of repeat thoracotomy on early surgical outcomes in TAAA patients. Methods: We conducted a retrospective cohort study of 214 patients who underwent open TAAA repair between June 1996 and March 2023. Among them, 30 underwent repeat thoracotomy (RT), and 184 underwent their first thoracotomy (FT). To reduce baseline discrepancies, propensity score matching (3:1) was performed, resulting in 22 RT patients matched with 45 FT patients. The primary outcome was 30-day mortality, while secondary outcomes included postoperative complications. Results: In the matched cohort, the median…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
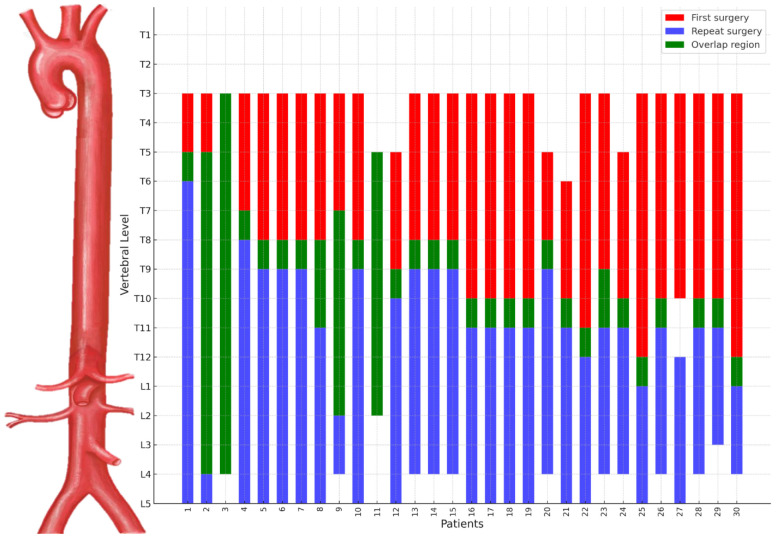 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAortic Disease and Treatment Approaches · Aortic aneurysm repair treatments · Cardiac and Coronary Surgery Techniques
1. Introduction
Managing thoracoabdominal aortic aneurysms (TAAA) requires an individualized approach tailored to the patient’s condition and the extent of intervention. Open repair remains a well-established modality, with contemporary series reporting acceptable operative mortality, low rates of major complications, and durable outcomes in high-volume and experienced centers [1,2,3]. Despite these positive results, late surgical failures remain challenging, often necessitating redo procedures due to disease progression in the residual aorta after prior descending aorta surgery [4]. Approximately 15% to 25% of patients undergoing TAAA open repair have a history of prior descending thoracic aorta surgery, indicating that reoperative scenarios are frequently encountered in clinical practice [3,5]. Redo surgeries present distinct technical challenges and heightened risks, particularly when repeat thoracotomy is required. Previous surgery involving the descending thoracic aorta complicates subsequent procedures due to adhesions and the complex dissection needed to address intricate lesions [6]. As a result, repeat thoracotomies require more meticulous planning than initial operations.
Predisposing factors such as connective tissue disorders, aortic dissection, and Crawford classification types II or III are often observed in patients undergoing redo TAAA procedures procedures [5,7,8]. However, prior studies have largely focused on reporting outcomes after reoperative thoracic aortic surgery, often including both descending thoracic and thoracoabdominal aneurysm repair, without specifically evaluating whether repeat thoracotomy itself contributes to operative risk in redo TAAA repair [5,8]. To address this gap, our study analyzes outcomes of open TAAA repair by comparing cases involving repeat thoracotomy with first-time TAAA surgeries using propensity score matching to achieve a balanced comparison. Specifically, we aimed to evaluate our institutional experience with TAAA open repair and assess the impact of repeat thoracotomy on early outcomes.
2. Methods
2.1. Patients
This retrospective cohort study included 214 patients who underwent TAAA surgery at Samsung Medical Center from June 1996 to March 2023. Among these patients, 30 required repeat thoracotomy due to prior descending aorta surgery, comprising the Repeat Thoracotomy (RT) group. Patients without a history of descending thoracic aorta surgery who underwent their first thoracotomy for thoracoabdominal repair were designated as the First Thoracotomy (FT) group. To reduce baseline discrepancies, propensity score matching at a 3:1 ratio was conducted based on age, replacement level, comorbidities, aneurysm type, and other relevant baseline characteristics (Table 1). After matching, the RT group included 22 patients, and the FT group included 45. This study was approved by the Institutional Review Board of Samsung Medical Center (SMC 2024-09-036-001, approved 15 October 2024), with informed consent waived as all data were de-identified.
2.2. Definitions
Thoracoabdominal aortic aneurysms were classified by the Crawford classification. For patients in the RT group, classification was based on the extent of reoperation and replacement level, employing the Crawford classification for consistency. The primary outcome was 30-day mortality. Respiratory complications were defined as the requirement for mechanical ventilation beyond 48 h. Early complications were defined as adverse events occurring within 30 days postoperatively, including permanent spinal cord injury resulting in paraplegia, acute renal failure necessitating dialysis, major ischemic or hemorrhagic stroke, and the need for extracorporeal life support.
2.3. Surgical Procedure
Anesthesia was induced with continuous pressure monitoring via a right radial arterial line, and one-lung ventilation was achieved using a double-lumen endotracheal tube. Additional monitoring included a second arterial line in the right femoral artery and a Swan-Ganz catheter inserted through the right internal jugular vein. Patients were positioned semi-laterally for a thoracoabdominal incision, which was extended to the abdominal midline. Partial cardiopulmonary bypass was initiated using cannulas in the left femoral artery and vein. Selective perfusion of the celiac, renal, and superior mesenteric arteries was employed to minimize organ ischemia. To prevent spinal cord ischemia in replacements extending below T10, a lumbar drain was used to maintain cerebrospinal fluid (CSF) pressure below 10 mmHg during surgery. Motor-Evoked Potentials (MEP) and Somatosensory-Evoked Potentials (SSEP) monitoring began after induction and before positioning in non-emergency cases, along with CSF drainage for patients at higher risk of spinal cord ischemia. In response to signal changes, continuous neuromonitoring facilitated immediate corrective interventions, such as adjusting perfusion flow or reducing cross-clamp time.
2.4. Statistical Analysis
Statistical analyses were conducted using R Statistical Software (version 4.2.0; R Foundation for Statistical Computing, Vienna, Austria). Continuous variables were expressed as mean (standard deviation) or median (interquartile range), while categorical variables were reported as proportions. Group comparisons were performed using the Chi-square or Fisher’s Exact test for categorical variables and the student t-test or the Mann-Whitney U test for continuous variables. The propensity score–matched analysis was designed to enable a more balanced and rigorous comparison of population-averaged outcomes between patients with and without repeat thoracotomy. To preserve the number of patients available for analysis while maintaining adequate balance, a 3:1 matching ratio was selected. Propensity score matching was performed using the nearest neighbor method with a caliper width of 0.2. Due to the small sample size of the RT group, not all baseline characteristics variables from Table 1 were used for matching. Instead, six variables were selected based on the comparison of baseline characteristics between the RT and FT groups, with a p-value ≤ 0.2. These variables included age, sex, connective tissue disease, chronic aortic dissection, cardiac surgery history, and Crawford type. After matching, the balance of variables was assessed using standardized mean differences (SMD), confirming that all SMD values were ≤0.2 (Supplementary Figure S1).
For comparisons between the matched groups, categorical and continuous variables were analyzed using the generalized estimating equation (GEE). Variables exhibiting complete separation were excluded from the GEE models to ensure model stability. Outcome analysis was conducted on the overall cohort using multivariable logistic regression for categorical variables and multiple linear regression for continuous variables. Each outcome was adjusted for covariates with a p-value ≤ 0.2 through backward selection, along with adjustment for the presence of repeat thoracotomy. Statistical significance was defined as a p-value < 0.05.
3. Results
3.1. Demographics and Baseline Characteristics
In the overall cohort, the median age was significantly lower in the RT group (49.1 years, IQR [40.1–56.3]) compared to the FT group (60.2 years, IQR [43.8–69.9]; p = 0.019) (Table 1). The RT group also demonstrated a higher prevalence of connective tissue disease (50.0% vs. 29.9%, p = 0.049) and chronic aortic dissection (83.3% vs. 62.0%, p = 0.039). Moreover, Crawford type III aneurysms were more frequent in the RT group than in the FT group (Table 1). Following propensity score matching, the median age in the RT group was 53.0 years (IQR [47.2–68.3]) compared to 53.3 (IQR [42.5–68.0]) years in the FT group, with no statistically significant difference (p = 0.793). Additionally, there were no significant differences between the matched groups regarding gender, prevalence of connective tissue disease, chronic dissection, or other key clinical variables.
Table 2 presents a detailed description of the RT group. Most patients had previously undergone descending thoracic aorta replacement (86.7%), with aneurysms being the main indication for reoperation (86.6%). The median interval between the initial and repeat surgeries was 3.4 years (IQR [1.0–4.9]). As shown in Figure 1, repeat thoracotomies frequently required a lower thoracic approach compared to the initial surgical intervention, reflecting extension of prior descending thoracic aortic repair into the thoracoabdominal segment.
3.2. Operative Data and Postoperative Outcomes
Operative data revealed no significant differences between the RT and FT groups in the overall cohort (Table 3). However, in the propensity-matched cohort, the median operation time was significantly longer in the RT group (500.0 min, IQR [476.0–552.0]) than the FT group (459.0 min, IQR [426.0–514.0]; p = 0.037). There were no significant differences between the groups in terms of cardiopulmonary bypass (CPB) time, aortic cross-clamp (ACC) time, use of lumbar drains, or MEP/SSEP monitoring (Table 3).
The 30-day mortality rates were comparable between the RT group (3.3%) and the FT group (5.4%) in the overall cohort (OR = 0.626, 95% CI: 0.033–3.653, p = 0.666). In the propensity-matched cohort, the 30-day mortality rates were 4.5% and 2.2% for the RT and FT groups, respectively (OR = 3.095, 95% CI: 0.184–52.158, p = 0.432) (Table 4). Importantly, no cases of paraplegia were reported in either group within the matched cohort. Acute renal failure requiring dialysis occurred in 13.6% of RT patients and 11.1% of FT patients (p = 0.799). Major stroke occurred in 9.1% of patients in the RT group but was not observed in the FT group. Postoperative bleeding was observed in 13.6% of the RT group and 2.2% of the FT group, with a higher proportion in the RT group. However, this difference was not statistically significant (OR = 10.263, 95% CI: 0.997–105.621, p = 0.050). Respiratory complications, hospital stay, and ICU duration showed no statistically significant differences between the two groups. Other complications, including gastrointestinal complications, graft infection, and ECLS, could not be analyzed due to data limitations.
4. Discussion
This study evaluated the impact of repeat thoracotomy on early surgical outcomes in patients undergoing open thoracoabdominal aortic aneurysm (TAAA) repair with prior left thoracotomy. When the overall cohort was stratified into first-time thoracotomy (FT) and repeat thoracotomy (RT) groups, differences in baseline disease characteristics were observed, particularly with respect to connective tissue disease and chronic aortic dissection.
Consistent with prior studies [5,8], the RT group demonstrated a higher prevalence of connective tissue disorders, reflecting the progressive nature of aortic disease in this population. Notably, chronic aortic dissection was highly prevalent in the RT group, accounting for approximately 80% of cases, and remained frequent in the overall cohort (approximately 60%). These proportions are higher than those reported in several prior series, in which chronic aortic dissection has typically accounted for about 30–40% of patients undergoing open TAAA repair [5,8]. Similarly, the prevalence of connective tissue disease in our cohort was relatively high, affecting approximately 30% of patients overall and nearly 50% of those in the RT group, compared with rates of roughly 10–15% reported in previous studies [5,8].
Many patients in the RT group had previously undergone descending thoracic aorta replacement, which influenced the extent of replacement required during subsequent TAAA surgery. Taken together with the baseline disease profile of this cohort, these findings suggest that repeat thoracotomy was commonly required due to progressive aortic disease extending beyond the initially treated segment, rather than isolated technical failure of the prior repair.
Given the inherent clinical differences between patients undergoing first-time and repeat thoracotomy, propensity score matching was applied to facilitate a more balanced comparison of early outcomes between groups. Despite the increased technical complexity and extended operative times associated with repeat thoracotomy during open TAAA repair, our results demonstrated no significant differences in early adverse outcomes, including mortality and major complications, compared to first-time TAAA surgeries. These findings underscore that, with meticulous preoperative planning and precise intraoperative execution, open TAAA repair performed in the setting of repeat thoracotomy can achieve early outcomes without a clear increase in adverse events compared with first-time TAAA procedures.
4.1. Challenges and Technical Considerations of Repeat Thoracotomy
Repeat thoracotomy presents distinct challenges, primarily due to adhesions, scarring, and altered anatomy from previous surgeries. These factors complicate surgical dissection, elevate the risk of bleeding and injury to surrounding structures, and contribute to prolonged operative times, ultimately increasing surgical risk and complexity. Our data confirmed these anticipated challenges, as indicated by the significantly longer operative times observed in the RT group compared to the FT group (500.0 min vs. 459.0 min, p = 0.037). This finding aligns with previous studies highlighting the increased technical demands of redo aortic surgery [9,10]. Despite these challenges, our analysis found no significant increase in early mortality or major complications, such as renal failure requiring dialysis, stroke, or paraplegia, in the RT group compared to the FT group. The absence of significant differences in these critical outcomes suggests that advanced surgical techniques and careful intraoperative management can mitigate the inherent risks of repeat thoracotomy. However, postoperative bleeding was observed at a higher rate in the RT group compared to the FT group (13.6% vs. 2.2%, p = 0.050). Although not statistically significant, the possibility of bleeding during open TAAA repair in the setting of repeat thoracotomy should not be overlooked.
Although surgical site infection was not specifically evaluated as an outcome in this study and no clear signal was identified, repeat thoracotomy inherently involves extensive dissection and prolonged operative time. Accordingly, while no conclusions can be drawn from the present data, careful attention to perioperative infection prevention remains warranted in this clinical setting.
4.2. Intraoperative Strategies to Minimize Risks
Several intraoperative strategies likely contributed to the favorable outcomes observed in the RT group. During aortic cross-clamping, selective perfusion techniques for the celiac, renal, and superior mesenteric arteries were crucial in minimizing organ ischemia. Additionally, CSF drainage was routinely employed when the replacement extended below the T10 level to mitigate the risk of spinal cord ischemia, a well-known complication of thoracoabdominal aortic surgery. MEP and SSEP monitoring, in conjunction with CSF drainage, enabled real-time assessment of spinal cord perfusion and immediate corrective measures when signal changes were detected. These approaches are well-documented in the literature as effective methods for reducing the incidence of paraplegia and other neurological complications in complex aortic surgeries [11,12,13,14]. Especially in the RT group, there were no cases of paraplegia, which can be attributed to the protective strategies described above and the concept of staged operations. Most repeat surgeries involved replacement below the segment treated in the initial surgery, similar to the staged TAAA approach, which has been shown to reduce the risk of paraplegia [15,16]. Studies indicate that following the initial surgery, remodeling of collateral vessels in large muscles provides blood flow to the spinal cord, helping maintain perfusion after descending aortic aneurysm repair. Likewise, the interval between the initial and redo surgeries may allow for developing a more robust collateral blood supply, potentially reducing the risk of ischemia.
4.3. Comparative Outcomes
Early studies have reported outcomes of open thoracoabdominal aortic aneurysm (TAAA) repair in patients with prior thoracic or aortic surgery; however, the specific contribution of repeat left-sided thoracotomy itself has been less well characterized [10,17]. Among the earliest reports focusing on this issue, Kawaharada et al. described open TAAA repair through redo left-sided thoracotomy following prior descending thoracic aortic surgery, reporting no statistically significant differences in early complications despite prolonged operative times related to adhesions and altered anatomy [9]. The propensity-matched analysis revealed no statistically significant differences in early mortality between the RT and FT groups, indicating repeat thoracotomy was not associated with worse early outcomes, rather than demonstrating equivalence. This finding is particularly significant given that nearly 90% of redo surgeries in the RT group were necessitated by disease progression in the residual aorta—a scenario frequently encountered in patients with connective tissue disorders or chronic aortic dissection
In our study, early mortality within 30 days was observed in 11 of 214 patients, with only one death (3.3%) in the redo group. Bleeding was the most common cause of mortality, accounting for 45.5% (5 cases) of deaths (Supplementary Table S1). Among these, one bleeding-related death in the RT group occurred during emergency surgery for impending rupture of a native aortic aneurysm at a level not previously operated on. In this case, lung parenchymal injury during the procedure resulted in severe bleeding and eventual death. Although rare, the bleeding-related death observed in the RT group highlights the need for heightened caution when performing open TAAA repair in the setting of repeat thoracotomy, particularly in emergency settings. Although this difference did not reach conventional statistical significance, the magnitude of the observed effect suggests that postoperative bleeding may represent a clinically relevant and hypothesis-generating trade-off associated with repeat thoracotomy.
Taken together, these findings suggest that prior left thoracotomy may not be associated with worse early outcomes in patients undergoing open TAAA repair at experienced centers. However, clinically anticipated risks related to repeat thoracotomy, particularly bleeding associated with adhesions and lung injury, should be carefully considered during surgical planning and perioperative management.
4.4. Limitations
This study has several limitations. First, it is a retrospective, single-center study, which may limit the generalizability of our findings. Moreover, as the study reflects outcomes from an experienced center with established perioperative protocols, the results may not be directly generalizable to other institutional settings with different levels of expertise or infrastructure. Although propensity score matching was employed to balance baseline characteristics, residual confounding cannot be excluded. In addition, alternative analytical approaches may yield different estimates, and residual confounding related to methodological constraints cannot be fully excluded. In particular, unmeasured factors such as prior operative complexity, emergency status, renal function or other clinical characteristics may have influenced both the likelihood of repeat thoracotomy and early outcomes. Furthermore, the small sample size of the data may limit the statistical interpretation of the results, highlighting the need for future analyses with larger datasets. Lastly, while this study focused on early outcomes, the long-term impact of repeat thoracotomy on survival and quality of life remains unclear and warrants further investigation.
5. Conclusions
In conclusion, in this propensity score–matched analysis, no statistically significant differences in early clinical outcomes between FT and RT groups undergoing open TAAA repair. These findings suggest that prior left thoracotomy, when present in patients undergoing open TAAA repair, may not be associated with worse early outcomes in appropriately selected patients treated at experienced centers. However, given the limited sample size and the potential for residual confounding, these results should be interpreted with caution. Rather than serving as definitive evidence to guide clinical decision-making, our findings underscore the importance of individualized assessment and institutional expertise when considering open TAAA repair in patients with a history of prior left thoracotomy for descending thoracic or thoracoabdominal aortic surgery. Further studies with larger cohorts and longer follow-up are warranted to better define patient selection and long-term outcomes in this high-risk population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Murana G. Castrovinci S. Kloppenburg G. Yousif A. Kelder H. Schepens M. de Maat G. Sonker U. Morshuis W. Heijmen R. Open Thoracoabdominal Aortic Aneurysm Repair in the Modern Era: Results from a 20-Year Single-Centre Experience Eur. J. Cardio-Thorac. Surg.2016491374138110.1093/ejcts/ezv 41526612715 · doi ↗ · pubmed ↗
- 2Moulakakis K.G. Karaolanis G. Antonopoulos C.N. Kakisis J. Klonaris C. Preventza O. Coselli J.S. Geroulakos G. Open Repair of Thoracoabdominal Aortic Aneurysms in Experienced Centers J. Vasc. Surg.201868634645.e 1210.1016/j.jvs.2018.03.41030037680 · doi ↗ · pubmed ↗
- 3Cook I.O. Green S.Y. Rebello K.R. Zhang Q. Glover V.A. Zea-Vera R. Moon M.R. Le Maire S.A. Coselli J.S. Comparison of Open Thoracoabdominal Repair for Chronic Aortic Dissections and Aneurysms J. Vasc. Surg.20248032333510.1016/j.jvs.2024.03.02638537876 · doi ↗ · pubmed ↗
- 4Coselli J.S. Reflection of Pioneers: Redo Thoracoabdominal Aortic Aneurysm Repair Controversies in Thoracic Aortic Aneurysm Surgery Gen. Thorac. Cardiovasc. Surg.20196716817410.1007/s 11748-018-0978-y 30069676 · doi ↗ · pubmed ↗
- 5Coselli J.S. Rosu C. Amarasekara H.S. Green S.Y. Zhang Q. Price M.D. Le Maire S.A. Reoperative Surgery on the Thoracoabdominal Aorta J. Thorac. Cardiovasc. Surg.2018155474485.e 110.1016/j.jtcvs.2017.08.02428947195 · doi ↗ · pubmed ↗
- 6Etz C.D. Zoli S. Kari F.A. Mueller C.S. Bodian C.A. Di Luozzo G. Plestis K.A. Griepp R.B. Redo Lateral Thoracotomy for Reoperative Descending and Thoracoabdominal Aortic Repair: A Consecutive Series of 60 Patients Ann. Thorac. Surg.20098875876710.1016/j.athoracsur.2009.04.14019699894 · doi ↗ · pubmed ↗
- 7Afifi R.O. Sandhu H.K. Trott A.E. Nguyen T.C. Miller C.C. Estrera A.L. Safi H.J. Redo Thoracoabdominal Aortic Aneurysm Repair: A Single-Center Experience over 25 Years Ann. Thorac. Surg.20171031421142810.1016/j.athoracsur.2016.09.01327914637 · doi ↗ · pubmed ↗
- 8Lau C. Gaudino M. Gambardella I. Mills E. Munjal M. Elsayed M. Girardi L. Reoperative Repair of Descending Thoracic and Thoracoabdominal Aneurysms†Eur. J. Cardio-Thorac. Surg.20175250150710.1093/ejcts/ezx 07228460036 · doi ↗ · pubmed ↗