Pelvic Floor Muscle Training Following Surgery for Pelvic Organ Prolapse: Recommendation from Scientific Literature
Gianfranco Lamberti, Donatella Giraudo, Gianluca Ciardi, John Kenneth Levis

TL;DR
Pelvic floor muscle training after pelvic organ prolapse surgery may help improve urinary, sexual, and pelvic pain issues, but more research is needed to confirm its effectiveness.
Contribution
This scoping review maps the evidence for conservative rehabilitation interventions, emphasizing PFMT's potential role in post-POP surgery recovery.
Findings
PFMT shows benefits for symptom severity and pelvic muscle function in women with pelvic organ prolapse.
Postoperative rehabilitation may improve urinary continence, sexual function, and pelvic pain, though evidence is limited.
Current research often prioritizes surgical revision over conservative management, leaving gaps in understanding rehabilitation effectiveness.
Abstract
Background: POP surgery improves anatomical support and quality of life, but urinary, bowel, sexual, and pain issues are common after surgery. The role of rehabilitation in addressing these problems is recognized, though not yet clearly defined. Objective: This scoping review aims to map the clinical evidence on conservative rehabilitation interventions for urinary, bowel, and sexual dysfunction, and pelvic pain after POP surgery. Methods: In accordance with PRISMA-ScR guidelines, we included randomized controlled trials, cohort studies, observational studies, and systematic reviews relevant to post-surgical rehabilitation options frequently encountered in clinical settings, including pelvic floor muscle training (PFMT), physiotherapy, and multimodal programs. Meta-analysis was not conducted due to clinical and methodological heterogeneity across the studies. Results: PFMT demonstrates…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
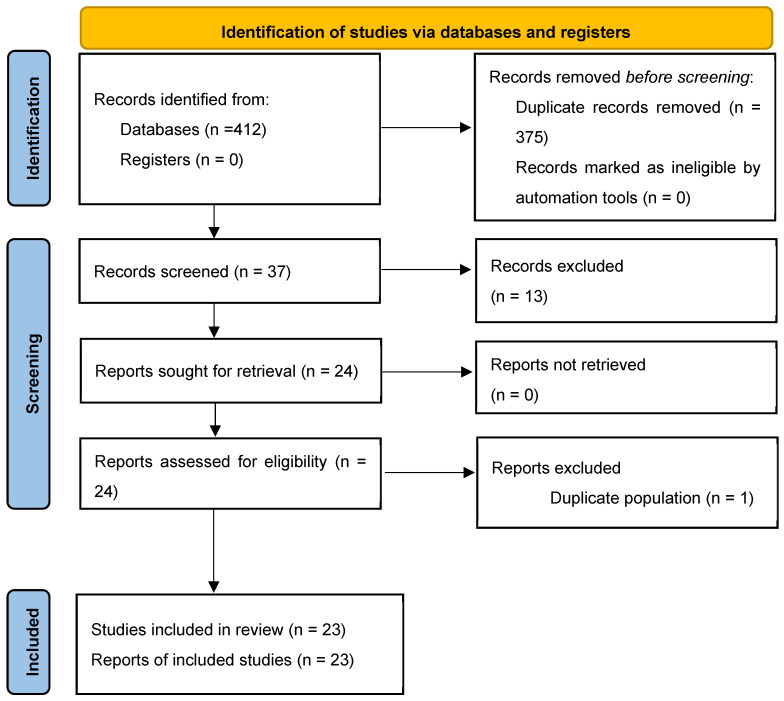 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPelvic floor disorders treatments · Enhanced Recovery After Surgery · Ureteral procedures and complications
1. Introduction
Pelvic organ prolapse (POP) refers to the descent of one or more pelvic organs—uterus, vagina, bladder, or bowel—through the vaginal canal. Prolapse is categorized as apical (uterine or post-hysterectomy vault), anterior (cystocele, urethrocele, or paravaginal defect), or posterior (enterocele, rectocele, or perineal defect). POP is prevalent in postmenopausal women and frequently involves multiple compartments simultaneously.
In the early stages, many women have no symptoms. As prolapse worsens, pelvic pressure, discomfort, and organ-specific issues affect daily activities and quality of life.
From a pathophysiological standpoint, pelvic organ prolapse is the ultimate manifestation of a progressive failure in the pelvic support structures, involving both the pelvic floor muscles and connective tissue. The International Continence Society (ICS) recommends that evaluating pelvic floor health should include standardized tests of muscle strength, endurance, coordination, and relaxation, along with a systematic examination of pelvic organ support using the POP-Q system [1]. This thorough approach helps clinicians link structural issues with functional impairments and symptoms.
Apart from digital exams, pelvic floor ultrasound—especially transperineal and endovaginal scans—has become an important method for assessing levator ani strength, hiatal size, organ mobility, and connective tissue defects. Ultrasound allows objective visualization of muscle injury, avulsions, and support problems that are closely linked to prolapse development, recurrence, and postoperative problems [2,3].
The biomechanical model called Petros’ Integral Theory explains how tissue damage relates to clinical symptoms. It suggests that prolapse and related urinary, bowel, sexual, and pain issues stem from weakened ligament support and altered neuromuscular control of the pelvic floor [4]. Surgery can fix anatomy but does not automatically restore nerve and muscle function. Hence, postoperative rehabilitation, especially pelvic floor muscle training, is crucial for re-establishing proper muscle coordination, load sharing, and continence within the support system.
This comprehensive understanding of anatomy, neuromuscular control, and tissue mechanics underpins why rehabilitation is an essential part of managing women undergoing pelvic organ prolapse surgery.
Pelvic floor muscle training (PFMT) is the primary conservative management option for women with symptomatic POP. PFMT aims to strengthen, coordinate, and enhance the endurance of pelvic floor muscles, which can improve the support of pelvic organs and alleviate symptoms such as incontinence and pelvic discomfort. Success depends on accurate assessment, supervised exercise instruction, and patient adherence, with studies showing symptom improvement and enhanced functional capacity [5,6].
Treatment depends on prolapse stage, symptoms, and patient preference, and includes conservative approaches—like observation, pessaries, and PFMT—or surgery. Surgery can be vaginal, laparoscopic, robotic, or open, with or without mesh. Choice depends on patient expectations, reproductive plans, and goals. Both methods aim to restore support and reduce symptoms [7].
About 11% of women will have POP surgery by age 79 [8]. This risk may double in the next 20 years due to aging.
Despite the anatomical success of prolapse repair, many women experience recurrence or new-onset pelvic floor dysfunctions after surgery. Rates of anatomical recurrence range from 19% to 45%. Reoperation rates reach 3–20%, depending on the surgical technique and length of follow-up [9,10,11]. Stress urinary incontinence may persist or newly appear in 4–50% of patients [12,13,14]. De novo overactive bladder symptoms occur in about 5–30% [13,14,15,16]. Dyspareunia and sexual dysfunction are reported in 5–17% of women [12]. New-onset dyspareunia affects about 7% two years after vaginal repair [13,14,16,17]. Bowel dysfunctions such as obstructed defecation persist in up to 37% of cases. Fecal incontinence occurs in up to 5% [16,18,19]. Chronic or new pelvic pain develops in 2.5–17% of cases, especially after mesh-based repairs or sacrospinous fixation [13,16,20,21].
These dysfunctions—whether persistent or new—impact the urinary, bowel, sexual, and pain domains and worsen quality of life. Table 1 presents the main outcomes and rates, highlighting the need for targeted rehabilitation.
Emerging evidence suggests that women with stronger pelvic floor muscle function before surgery may be less likely to have recurrence or require reoperation. This supports PFMT in the perioperative phase, as it has demonstrated benefits such as increased muscle strength and coordination, reduced risk of recurrent urinary, bowel, or sexual dysfunction, and improved quality of life after surgery.
The multidisciplinary management of complications after pelvic reconstructive surgery—especially mesh complications—has been emphasized in the Joint Position Statement from AUGS, SUFU, SGS, and IUGA (2020/2021) [25]. This highlights the value of conservative approaches, such as pelvic floor physical therapy, pain management, and psychological support. It aligns with evidence supporting physiatrically guided rehabilitation as part of conservative management for postoperative pelvic floor dysfunction.
Pelvic surgery may affect the function of pelvic floor muscles, and the connective tissue supporting pelvic organs, leading to dysfunction. PFMT specifically targets strength, endurance, and coordination, which can help reduce symptoms of prolapse, urinary and fecal incontinence, and sexual dysfunction, therefore representing a practical and low-risk support intervention.
Adding PFMT to perioperative care aligns with the Enhanced Recovery After Surgery (ERAS) model, which encourages early mobilization, multimodal management, and faster recovery [26]. These methods aim to improve healing and quality of life beyond anatomy alone.
Despite increasing attention, available literature remains fragmented and lacks a comprehensive synthesis of postoperative rehabilitation strategies following POP surgery.
This review focuses on dysfunctions likely to respond to PFMT—such as incontinence, defecatory disorders, sexual dysfunction, and pelvic pain—not on mechanical issues like retention, mesh exposure, or structural failure, which are outside rehabilitation. The aim is to identify and summarize evidence for PFMT in postoperative rehab for POP in women, examining effects on recovery, quality of life, and recurrence, while highlighting current knowledge gaps and directions for future research and practice. Although the primary focus of this review is postoperative rehabilitation, selected preoperative studies were included to provide a necessary interpretative framework for understanding the timing and potential mechanisms of pelvic floor muscle training. Specifically, preoperative trials allow comparison of neuromuscular training delivered in the presence of distorted pelvic anatomy with training applied after surgical restoration of support. The consistent lack of postoperative benefit following preoperative PFMT observed in high-quality trials suggests that anatomical correction may be a prerequisite for effective neuromuscular re-education. In this way, preoperative evidence directly informs the postoperative context by clarifying the physiological conditions under which rehabilitation is more likely to be effective.
2. Materials and Methods
2.1. Rationale for Choosing a Scoping Review Design
A scoping review was chosen because of the varied study designs, interventions, and outcomes in the POP rehab literature. Existing research is fragmented and variable, especially regarding bowel function, pain, and sexual health. Included studies range from RCTs to systematic reviews, but outcomes are inconsistently reported. A scoping review helps map the evidence and gaps, and clarifies the range of rehab strategies for POP-related dysfunction. This follows guidance from the Joanna Briggs Institute (JBI) [27] and the PRISMA-ScR checklist [28].
2.2. Eligibility Criteria
The eligibility criteria were defined using the Population–Concept–Context (PCC) framework recommended by JBI. The population of interest included women who underwent surgical treatment for pelvic organ prolapse (POP), regardless of surgical approach or stage of prolapse. The concept focused on any form of postoperative rehabilitation intervention, including pelvic floor muscle training (PFMT), biofeedback, electrical stimulation, manual therapy, behavioral education, or multidisciplinary care. The context encompassed all healthcare settings in which postoperative rehabilitation was provided, including inpatient, outpatient, and community-based services, without restriction by geographic location or healthcare system.
Studies were eligible for inclusion if they met the following criteria:
- (a)Involved women after POP surgery;
- (b)Evaluated at least one form of pelvic floor rehabilitation;
- (c)Reported outcomes related to urinary, bowel, sexual function, pain, or recurrence (quality of life outcomes were also considered when available);
- (d)Were published in peer-reviewed journals and written in English or French.
Both empirical studies (randomized controlled trials, observational studies, feasibility or pilot studies) and secondary literature (systematic reviews, narrative reviews, expert consensus, clinical reports) were considered eligible for inclusion, reflecting the exploratory aim of this scoping review. Articles without clinical outcome data relevant to the dysfunctions of interest, those reporting exclusively anatomical outcomes, or those lacking methodological transparency were excluded from structured appraisal but could be referenced narratively for context.
2.3. Information Sources and Search Strategy
A comprehensive search strategy was developed in consultation with the Joanna Briggs Institute (JBI) methodological guidance for scoping reviews. The following electronic databases were searched: PubMed/MEDLINE, Embase, CINAHL, Scopus, PEDro, and Google Scholar. The PubMed search string combined controlled vocabulary (MeSH terms) and free-text terms related to pelvic organ prolapse, surgery, and rehabilitation. Search strategies were then adapted to the indexing systems of each database (Emtree for Embase, CINAHL Headings for CINAHL, keyword and title/abstract fields for Scopus and PEDro). For Google Scholar, simplified keyword combinations were applied, given the limitations of Boolean operators, and the first 200 results were screened as recommended for scoping reviews. The complete search strategies for all databases are provided in Table S1. No restrictions were applied on language, publication date, or geographic location at the initial search stage.
2.4. Screening of Records and Critical Appraisal
All records were manually screened by two independent reviewers, while a third opinion was requested to solve conflicts. After removing duplicates and unreadable records, a first screening for title and abstract was applied. Then, eligible papers were recovered in full text, and by application of inclusion criteria (PCC) relevant articles were selected for the final stage of the review.
Although not even performed for scoping design, we planned a critical appraisal for included papers, in order to inform the interpretation of findings and highlight areas where evidence is more or less robust. Particularly, we used the following:
- -Cochrane Risk of Bias 2 (RoB 2) [29] and PEDRO scale tools for RCTs.
- -AMSTAR 2 [30] checklist for systematic review.
- -SANRA (Scale for the Assessment of Narrative Review Articles) [31] for narrative reviews.
- -JBI Checklist for Text and Opinion [32] for expert opinion papers.
3. Results
As shown in Figure 1, the database search yielded 412 records: 65 from PubMed, 98 from Embase, 38 from CINAHL, 11 from PEDro, and 200 from Google Scholar. After removal of duplicates, 37 unique records remained. These were screened by title and abstract, leading to the exclusion of 12 studies that did not meet the eligibility criteria. The full text of the remaining 24 articles was retrieved and assessed for eligibility. Among these, one article was excluded from the quantitative count because it reported on the same study population as another included publication, although both were retained for descriptive purposes as they provided complementary information (e.g., different outcomes or follow-up periods). As a result, 23 studies were included in the final synthesis: 15 randomized controlled trials, 4 systematic reviews, 2 narrative reviews, and 1 expert or opinion paper.
4. Appraisal
Sixteen of our included papers [33,34,35,36,37,38,39,40,41,42,43,44,45,46,47] were RCTs, and Rob 2 evaluation was performed. Four systematic reviews [48,49,50,51] were analysed through AMSTAR 2 tool; two narrative reviews [52,53] was examined with SANRA scale, and finally a clinical opinion paper [54] was analysed through JBI text & opinion tool.
Table 2, Table 3, Table 4 and Table 5 summarizes included articles’ main characteristics and appraisal.
4.1. Overall Commentary on Randomized Controlled Trials and Reviews Evaluating PFMT After POP Surgery
The randomized and secondary literature on PFMT as an adjunct to surgery for pelvic organ prolapse (POP) provides a broad yet heterogeneous picture. Most studies converge on the feasibility and safety of perioperative rehabilitation but diverge regarding its additive benefit beyond surgical repair.
Dawson et al. (2018) [36] conducted a randomized controlled trial following vaginal reconstructive surgery for POP to evaluate whether an early, structured physiotherapy program—focused on muscle awareness, strength, and coordination—could improve postoperative recovery compared with standard care. Both groups demonstrated significant improvements in pain, urinary symptoms, and quality of life (PFDI-20, PFIQ-7, WHOQOL-BREF) at twelve weeks, with no statistically significant differences between them. Although available only as a conference abstract, this trial supports the feasibility and safety of early postoperative rehabilitation and provides preliminary evidence that structured physiotherapy may facilitate functional recovery.
Barber et al. (2014) [33] examined perioperative behavioral therapy combined with PFMT (BPMT) versus usual care. At two years, BPMT did not significantly improve urinary or prolapse symptom scores (UDI, POPDI) or anatomical outcomes. This high-quality multicenter trial—with masked assessors and robust outcome definitions—offers strong evidence that brief perioperative PFMT confers no measurable benefit when performed alongside surgical correction. Nonetheless, the authors acknowledged that targeted rehabilitation might still be relevant for women with residual or de novo dysfunctions after surgery, encouraging further research in this subgroup.
In a secondary analysis of the same OPTIMAL trial, Borello-France et al. (2023) [34] investigated adherence to BPMT and its association with outcomes at 24 months. Despite standardized therapist training, long-term adherence was poor, and no additional benefit was detected from perioperative PFMT. These findings highlight behavioral and motivational barriers to sustained engagement, suggesting that postoperative rehabilitation requires individualized follow-up, prolonged supervision, and strategies to enhance adherence rather than short perioperative programs.
Brandt and Janse van Vuuren (2022) [35] compared three postoperative strategies in women undergoing reconstructive surgery for stage II–III POP: (1) PFMT alone, (2) PFMT combined with abdominal training using pressure biofeedback and EMG guidance, and (3) standard postoperative counseling. Both PFMT groups, trained twice weekly for six months, achieved superior gains in pelvic muscle strength, endurance, and contraction speed compared with controls. However, quality-of-life (P-QOL) and anatomical (POP-Q) improvements were similar across all arms, indicating that the primary benefit was derived from surgical repair itself. Despite a modest sample and short follow-up, the study confirms that postoperative PFMT is a safe and feasible means of restoring muscular performance, even if its short-term symptomatic advantages remain limited.
Similarly, Duarte et al. (2020) [37] found no added benefit from an intensive PFMT regimen (four preoperative and seven postoperative sessions) over surgery alone. Both groups experienced significant postoperative improvements in prolapse symptoms (PFDI-20), pelvic floor strength, quality of life, and sexual function at 40 and 90 days, with no significant between-group differences.
Frawley et al. (2010) [38] investigated individualized PFMT as an adjunct to prolapse surgery or hysterectomy. Despite 1 preoperative and 7 postoperative sessions over 12 months, no significant between-group differences emerged in symptoms or quality of life. Participants receiving physiotherapy exhibited greater ability to perform correct pelvic floor contractions, but this did not translate into measurable clinical gains. As noted by Bø et al. (2022) [52], the trial provides early evidence of improved muscular control without a clear symptomatic impact during the first postoperative year.
Jarvis et al. (2005) [39] reported more favorable short-term results. In 60 women undergoing corrective surgery for incontinence or POP, perioperative physiotherapy—including PFMT, the “Knack,” and bladder-bowel education—led to greater reductions in urinary symptoms, enhanced quality of life, and stronger pelvic contractions at 12 weeks compared with standard care. However, the trial was small and methodologically limited, and later [50] classified it as a preliminary feasibility study with inconclusive efficacy.
In the long-term follow-up of the OPTIMAL study, Jelovsek et al. (2018) [40] confirmed the lack of any sustained effect of perioperative BPMT. At five years, neither anatomical nor symptomatic outcomes differed significantly between behavioral and standard care groups, effectively ruling out delayed or cumulative benefits of PFMT.
Liang et al. (2019) [41] explored a short-term perioperative PFMT program combining four supervised sessions with daily home exercises. Both groups improved across prolapse-related symptoms, but the PFMT group demonstrated greater reductions in urinary distress (UDI-6) at 42 and 60 days. No differences were noted in POPDI-6 or CRADI-8 scores. These findings suggest that early supervised PFMT may selectively support urinary recovery by reactivating bladder control mechanisms, warranting longer-term studies to confirm its global impact.
McClurg et al. (2014) [43] conducted a feasibility RCT comprising one preoperative and six postoperative sessions over 12 weeks. The PFMT group reported fewer prolapse symptoms and stronger muscle performance at 12 months, confirming safety, acceptability, and potential symptomatic benefit, though the study was not powered to assess efficacy.
Pauls et al. (2014) [45] evaluated a structured postoperative PFMT program (five sessions with EMG feedback). Temporary improvements in EMG activity and muscle control were observed at 12 weeks but were not maintained at 6 months, reinforcing the view that short-term supervised PFMT yields transient neuromuscular gains without long-term anatomical or symptomatic advantages.
Wang et al. (2023) [46] analyzed the interaction between preoperative pelvic pain and postoperative outcomes within the OPTIMAL cohort, concluding that perioperative PFMT may have selective benefits for women with preexisting pain syndromes, although it does not influence anatomical results or overall satisfaction.
Weidner et al. (2017) [47] also found no significant differences in pelvic floor impact (PFIQ), sexual function (PISQ-12), body image, or general health (SF-36) at 24 months between BPMT and standard care. Both groups showed sustained improvement from baseline, underscoring that surgery remains the main determinant of postoperative recovery.
Among the secondary literature, Espiño-Albela et al. (2022) [49] synthesized RCTs comparing perioperative PFMT versus standard care, finding consistent gains in muscle strength and reduced symptom distress (PFDI-20, PFIQ-7), but no effect on anatomical recurrence or POP-Q staging. The review supports integration of PFMT into peri- and postoperative pathways while calling for standardized, long-term protocols.
De Oliveira et al. (2024) [48] conducted a meta-analysis of PFMT after hysterectomy, reporting moderate-quality evidence of significant improvements in sexual function (+5 FSFI points) but uncertain effects on urinary symptoms and quality of life due to high heterogeneity. The review confirms PFMT as a safe, feasible, and potentially beneficial approach, though long-term structural effects remain unproven.
Shahid et al. (2025) [50], in a Cochrane review of 7 RCTs (1032 women), found no significant effect of perioperative PFMT on prolapse awareness, reoperation rates, or failure rates, and no clinically relevant changes in symptom or QoL scores.
Similarly, Zhang et al. (2016) [51] reported that perioperative PFMT did not significantly affect prolapse symptoms, quality of life, or POP-Q measures, reinforcing the notion that the strong surgical effect may mask any incremental rehabilitation benefit.
The International Urogynecology Consultation chapter by Bø et al. (2022) [52] reached the same conclusion, stating that no consistent evidence supports PFMT—before or after surgery—as a means to enhance surgical outcomes or prevent recurrence.
Finally, Basnet et al. (2020) [53], in a narrative review, summarized that structured perioperative PFMT programs demonstrate inconsistent efficacy and generally do not provide measurable advantages over surgery alone, despite being safe and well tolerated.
Two additional randomized controlled trials—Nyhus et al. (2020) [44] and Mathew et al. (2021) [42]—explored the effects of preoperative PFMT in women awaiting surgical repair for pelvic organ prolapse (POP).
Both studies implemented intensive, prolonged, and well-supervised programs lasting approximately 20–22 weeks, with high adherence rates (70–80%). Despite their methodological rigor and adequate statistical power, neither trial demonstrated significant differences between PFMT and standard care in postoperative outcomes, including pelvic floor muscle strength, prolapse symptom severity, or quality of life at six months.
These findings suggest that preoperative conditioning alone does not modify the postoperative recovery trajectory in women with advanced POP. Mechanical constraints imposed by prolapsed organs and the dominant corrective effect of surgery likely limit the potential impact of muscular training before anatomical restoration.
Taken together, these results complement the neutral findings of peri- and postoperative RCTs, underscoring that the timing and context of PFMT application are crucial determinants of its efficacy. The evidence indicates that PFMT achieves its full rehabilitative potential after surgical correction—when pelvic anatomy has been restored and neuromuscular recruitment, proprioception, and continence mechanisms can be effectively re-educated—rather than as a preoperative preventive measure.
4.2. Interpretive Reflection: Implications of Preoperative Evidence for Postoperative PFMT
The inclusion of these preoperative studies provides an important comparator for interpreting the peri- and postoperative literature.
Mathew et al. (2021) [42] found no added effect of preoperative PFMT on symptoms or quality of life related to urinary and colorectal-anal discomfort in women scheduled for POP surgery; postoperative symptomatic improvements were reached regardless of PFMT. Similarly, Nyhus et al. (2020) [44], showed no effect of preoperative PFMT on pelvic floor muscle contraction, POP symptoms, or anatomical prolapse after surgery. In all patients, POP symptoms improved at the 6-month follow-up, likely due to anatomical correction of the POP.
These consistent null findings indicate that the preoperative period is not the most effective therapeutic window for achieving lasting functional benefits—most likely because of the mechanical and neurophysiological distortion inherent to advanced prolapse.
By contrast, the postoperative phase, in which surgical correction restores pelvic anatomy, appears to provide a more favorable environment for neuromuscular re-education, recovery of voluntary control, and prevention of recurrence. In this sense, preoperative studies indirectly reinforce the overall conclusion of peri- and postoperative trials: PFMT is best conceptualized as a rehabilitative rather than a preventive intervention, whose efficacy depends on functional strengthening, individualized supervision, and sustained continuity after surgery.
5. Discussion
On the basis of the available evidence, randomized trials do not demonstrate a clear preventive effect of PFMT on postoperative anatomical outcomes or prolapse recurrence. However, when these findings are interpreted within current biomechanical and neuromuscular models of pelvic floor function, PFMT may be more appropriately conceptualized as a rehabilitative intervention aimed at functional recovery, neuromuscular re-education, and long-term maintenance of pelvic floor performance rather than as a strategy for short-term anatomical prevention. This perspective is primarily supported by narrative and theoretical contributions in the literature and should therefore be considered hypothesis-generating rather than directly evidence-proven by the studies included in the present review.
Several factors may explain the limited additional clinical impact of PFMT observed in available trials. Most rehabilitation protocols were short, typically lasting 6 to 12 weeks, which is likely insufficient to induce stable neuromuscular adaptations and long-term functional integration. Furthermore, many interventions lacked true individualization, using standardized exercise prescriptions that did not adequately address differences in baseline muscle function, symptom profiles, or patient-specific biomechanical characteristics. Adherence issues and variability in supervision intensity may have further attenuated treatment effects. These methodological and clinical limitations should be considered when interpreting the neutral findings of existing trials.
A key factor in understanding these results is the strong therapeutic effect of surgery itself. Surgical correction restores anatomy and pelvic support immediately, directly relieving symptoms such as heaviness, bulging, or the sensation of incomplete emptying. By repositioning the organs and re-establishing the appropriate tension of the fascial support system, surgery profoundly modifies the biomechanics and neurophysiology of the pelvic floor. Such a marked anatomical and functional impact can overshadow or mask any additional effects of PFMT, especially during the early postoperative months when outcomes are typically assessed. In almost all studies, both intervention and control groups showed substantial improvements in symptoms and quality of life, mainly attributable to the corrective effect of surgery. Under these conditions, it becomes difficult to identify incremental benefits of rehabilitation.
Another limiting factor concerns the structure of the PFMT protocols applied. Most perioperative programs were short-term—generally lasting between 6 and 12 weeks—and focused on isolated muscle activation rather than on progressive, functional, and integrated approaches. True neuromuscular adaptation, however, requires time, repetition, and progressive loading. Short or non-individualized interventions rarely support stable motor learning, movement automatization, and integration into daily motor patterns. Therefore, longer, progressive, and individualized rehabilitation protocols may be required to achieve stable muscular recovery and to translate physiological gains into clinically meaningful outcomes. Exercises should nevertheless be prescribed according to the same principles and modalities that have proven effective in the conservative management of POP, as described in the protocols by Brækken et al. [5] and subsequent systematic reviews, which precisely define the parameters of intensity, frequency, and duration of pelvic floor muscle training. In line with the recommendations of the American College of Sports Medicine (ACSM) [55], training should be sufficiently intense, repetitive, and personalized to optimize the recovery of strength, power, and muscular endurance, thereby ensuring functional consolidation and preventing recurrences or de novo dysfunctions.
Several studies support the efficacy of PFMT when performed with adequate intensity and continuity: only a truly strong pelvic floor can counteract prolapse recurrence, as demonstrated by its effect on reducing low-grade prolapse and treating stress and urgency urinary incontinence. In all these contexts, clinical benefits emerge only when the exercise is correctly executed, with load progression and professional supervision, confirming that the quality of training represents the essential basis for functional recovery and long-term stability of surgical and rehabilitative outcomes.
Moreover, the outcome measures used—often symptom questionnaires or anatomical assessments—may be too coarse to detect subtle improvements in proprioception, endurance, or coordination that PFMT can induce.
From a biomechanical perspective, the type of exercise is also of fundamental importance: coordination among the pelvic floor, abdominal wall, and respiratory dynamics is crucial after POP surgery. In some studies, women performing PFMT in combination with abdominal exercises reported sensations of tension, heaviness, or downward pressure—signs that occur when intra-abdominal pressure is poorly controlled during training [31]. This highlights a crucial principle: re-educating the musculature, rather than simply treating symptoms, is essential for long-term pelvic stability. Effective rehabilitation should therefore include respiratory education, pressure control, and coordinated activation of pelvic, abdominal, and postural musculature. Such integrated re-education optimizes function and may help prevent recurrences or the onset of new dysfunctions over time. The use of hypopressive techniques, to date, has shown no proven efficacy [56,57].
To achieve these objectives, PFMT should be incorporated into personalized, progressive, and multidisciplinary rehabilitation pathways rather than proposed as a short-term perioperative intervention. The impact of surgery on prolapse makes it unlikely to observe measurable PFMT effects in the early postoperative phase; however, once healing is complete and mechanical correction stabilized, training becomes crucial to transform anatomical repair into functional competence. In this phase, muscle re-education promotes recovery of control, awareness, and body confidence, consolidating surgical outcomes and integrating them into daily motor patterns.
From a physiological standpoint, the post-surgical stabilization phase represents a particularly favorable moment for neuromuscular recovery. Once normal anatomy is restored, the pelvic floor can be retrained under optimal conditions, leading to improvements in proprioception, motor control, and continence reflexes. In this sense, PFMT should not be regarded as an accessory or merely a preventive intervention, but rather as a rehabilitative process that consolidates surgical repair by restoring coordinated neuromuscular function within the reconstructed anatomy. Moreover, targeted exercises may exert a selective effect on postoperative pain modulation (see literature on exercise and post-surgical pain mechanisms), underscoring the importance of individualized programs tailored to the patient’s preoperative symptom profile.
The rationale for postoperative PFMT extends beyond muscle strengthening to encompass recovery of neuromuscular integration and tissue healing. Pelvic surgery may temporarily impair the structural and functional integrity of the pelvic floor muscles and connective tissues that support the bladder and organs [48]. Training interventions improve coordination, endurance, and vascularization of the pelvic floor, thereby promoting optimal muscle recruitment and enhancing pelvic support [35,38,43]. These mechanisms contribute not only to the prevention of recurrence but also to the recovery of continence, defecatory efficiency, and sexual function.
Conceptually, this rehabilitative approach parallels the Enhanced Recovery After Surgery (ERAS) paradigm, which emphasizes early mobilization, multimodal rehabilitation, and optimization of functional recovery [26]. ERAS protocols primarily focus on optimizing the immediate postoperative phase through measures such as optimized fluid management, multimodal analgesia, early mobilization, reduction in complications, and shortening of hospital stay. In this context, the principles of ERAS provide a conceptual background supporting early functional activation and patient engagement. However, the structured rehabilitation programs discussed in the present review extend beyond the ERAS time window and should be regarded as complementary long-term functional strategies rather than direct components of ERAS pathways. Integrating PFMT within ERAS-oriented pathways may therefore facilitate more complete healing, minimize pain and stiffness, and accelerate the restoration of pelvic function and quality of life after prolapse repair.
Interventions specifically addressing patients with pre-existing pain or hypertonia may improve comfort, adherence, and the overall recovery trajectory.
Clinically, PFMT is a safe, feasible, and well-tolerated intervention. Although adverse events were not a primary outcome in the included studies, available evidence consistently indicates that PFMT is a safe intervention with a very low incidence of complications. In the most recent Cochrane review, 9 of 63 trials reported adverse events, with 66 events among 1083 participants (6%). Almost all were minor and transient, consisting mainly of vaginal discharge, spotting, or local discomfort. Importantly, these events were largely associated with intravaginal or intrarectal training devices rather than with PFMT itself, and no serious adverse effects were reported [58]. High-quality evidence consistently demonstrates that PFMT has an excellent safety and tolerability profile. Adverse effects are rare, generally mild and transient, and consist mainly of occasional discomfort or pain, with no serious complications reported [59]. More recent randomized trials further confirm these findings. No adverse events were observed during an eight-week supervised multimodal PFMT program, with perfect attendance (100%) and high participant satisfaction (84.6%) [60]. Similarly, in a 12-week PFMT randomized trial including 126 women, high adherence, significant functional and quality-of-life improvements, and no clinically relevant complications attributable to PFMT were reported [61].
Overall, PFMT should be considered an essential complement to prolapse surgery and implemented within sufficiently long, guided, and individualized programs tailored to each patient’s functional profile. A structured, continuous rehabilitation plan allows the long-term maintenance of gains and enhances the contribution of surgery to overall quality of life. To optimize long-term functional recovery, PFMT should be integrated into structured postoperative care pathways rather than delivered as an isolated intervention. Integration should include early postoperative assessment of pelvic floor function, individualized rehabilitation planning based on symptom profile and neuromuscular deficits, progressive supervised training phases, and scheduled long-term follow-up to support maintenance and adherence. Multidisciplinary collaboration among surgeons, physiotherapists, nurses, and primary care providers is essential to ensure continuity of care and timely adjustment of treatment strategies. Embedding PFMT within standardized postoperative pathways enables functional rehabilitation to directly complement anatomical repair, addressing persistent or de novo dysfunctions and improving durable quality-of-life outcomes.
Adherence to treatment also represents a significant barrier. In the postoperative phase, some patients fear that contractions might interfere with healing or cause pain, while others perceive exercise as unnecessary after surgical correction. These behavioral and motivational barriers compromise training continuity and attenuate its effects. However, when educational support and professional supervision are maintained over time, adherence rates and clinical outcomes improve significantly, confirming that the quality, duration, and personalization of the therapeutic pathway are as decisive as the exercise protocol itself. Improving adherence to PFMT in clinical practice requires structured, theory-driven, and patient-centered strategies. According to the International Continence Society State-of-the-Science report [62], key modifiable determinants of adherence include self-efficacy, positive intention to adhere, perceived benefits of the exercises, attitudes toward treatment, and integration of PFMT into daily activities. Effective strategies identified in the literature include individualized exercise prescription with goal setting, regular supervised follow-up, enthusiastic therapist engagement, structured treatment protocols, and the use of behavioral change models. Additional supportive tools, such as exercise diaries, audio prompts, reminder systems, and digital monitoring, may further enhance long-term adherence. These elements appear essential for translating neuromuscular improvements into durable functional outcomes.
From an applied standpoint, current evidence supports directing postoperative rehabilitation toward selected patients with residual or de novo dysfunctions, rather than universally prescribing it to all women undergoing POP surgery. A selective approach allows for optimization of resources and maximization of therapeutic impact. At the same time, future studies should accurately report PFMT parameters—intensity, frequency, supervision, and progression—since most studies failed to provide essential details, thereby limiting reproducibility and interpretation. Defining standardized, transparent, and replicable rehabilitation models is a key step in clarifying the actual clinical value of PFMT after POP surgery.
Based on the available randomized evidence, there is currently no high-level evidence that multimodal pelvic floor muscle training (MPFT) after prolapse surgery provides additional global benefits over surgery alone across different prolapse types. Nevertheless, from a clinical and pathophysiological perspective, individualized postoperative rehabilitation remains a reasonable and potentially valuable approach for managing persistent or de novo pelvic floor dysfunctions, including overactive bladder, stress urinary incontinence, pelvic pain, and dyspareunia. This strategy should be considered a targeted functional intervention aimed at symptom relief and quality-of-life improvement rather than a universally preventive or outcome-modifying treatment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Madhu C. Swift S. Moloney-Geany S. Drake M.J. How to use the Pelvic Organ Prolapse Quantification (POP-Q) system?Neurourol. Urodyn.201837 S 39S 4310.1002/nau.2374030614056 · doi ↗ · pubmed ↗
- 2Lai W. Wen L. Li Y. Huang X. Qing Z. Concordance of tomographic ultrasound and multiplanar ultrasound in detecting levator ani muscle injury in patients with pelvic organ prolapse P Lo S ONE 201813 e 019986410.1371/journal.pone.019986429979693 PMC 6034800 · doi ↗ · pubmed ↗
- 3Pietrus M. Pityński K. Gawron I. Socha M.W. Nowosielski K. Biskupski-Brawura-Samaha R. Waligóra M. Diagnostic utility of translabial ultrasound in pelvic organ prolapse: A prospective observational study J. Obstet. Gynaecol.202444238697510.1080/01443615.2024.238697539105256 · doi ↗ · pubmed ↗
- 4Petros P. Liedl B. Palma P. Riccetto C. Ding S. A practical ligament-based diagnostic system for cure of pelvic symptoms and prolapse Ann. Transl. Med.2024122710.21037/atm-23-175938721453 PMC 11075956 · doi ↗ · pubmed ↗
- 5Braekken I.H. Majida M. Engh M.E. BøK. Can pelvic floor muscle training reverse pelvic organ prolapse and reduce prolapse symptoms? An assessor-blinded, randomized, controlled trial Am. J. Obstet. Gynecol.2010203170.e 1170.e 710.1016/j.ajog.2010.02.03720435294 · doi ↗ · pubmed ↗
- 6Wang T. Wen Z. Li M. The effect of pelvic floor muscle training for women with pelvic organ prolapse: A meta-analysis Int. Urogynecol. J.2022331789180110.1007/s 00192-022-05139-z 35312800 · doi ↗ · pubmed ↗
- 7Pizzoferrato A.C. Thuillier C. Vénara A. Bornsztein N. Bouquet S. Cayrac M. Cornillet-Bernard M. Cotelle O. Cour F. Cretinon S. Management of female pelvic organ prolapse—Summary of the 2021 HAS guidelines J. Gynecol. Obstet. Hum. Reprod.20235210253510.1016/j.jogoh.2023.10253536657614 · doi ↗ · pubmed ↗
- 8Olsen A.L. Smith V.J. Bergstrom J.O. Colling J.C. Clark A.L. Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence Obstet. Gynecol.19978950150610.1016/S 0029-7844(97)00058-69083302 · doi ↗ · pubmed ↗