High-Power Laser Therapy for Oral Lichen Planus: A Systematic Review
Jakub Fiegler-Rudol, Wojciech Niemczyk, Jacek Matys, Jakub Hadzik, Dariusz Skaba, Rafał Wiench, Marzena Dominiak

TL;DR
This review finds that high-power lasers like CO2 and Er:YAG are effective and safe for treating oral lichen planus, reducing symptoms and side effects compared to traditional methods.
Contribution
The study systematically evaluates high-power laser therapy as a novel alternative for managing oral lichen planus.
Findings
High-power lasers significantly reduce lesion size, pain, and recurrence in OLP patients.
CO2 lasers show better lesion resolution and pain relief, while Er:YAG lasers offer precision for localized lesions.
Laser therapy is associated with minimal side effects and faster recovery times.
Abstract
Background/Objectives: Oral lichen planus (OLP) is a chronic, autoimmune-mediated mucocutaneous disorder that significantly impacts patients’ quality of life. Conventional therapies, such as corticosteroids, are often associated with side effects, prompting the exploration of alternative treatments. High-power lasers, including CO2 and Er:YAG lasers, have emerged as promising options due to their precision and therapeutic potential in managing OLP. This systematic review aimed to evaluate the effectiveness of high-power lasers in reducing lesion size, pain, and recurrence rates in OLP patients. Methods: A comprehensive search was conducted in databases such as PubMed, Scopus, Embase and Cochrane using keywords related to laser therapy and OLP. Inclusion criteria focused on randomized controlled trials and clinical studies with clear methodologies. Data from eight studies were analyzed,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
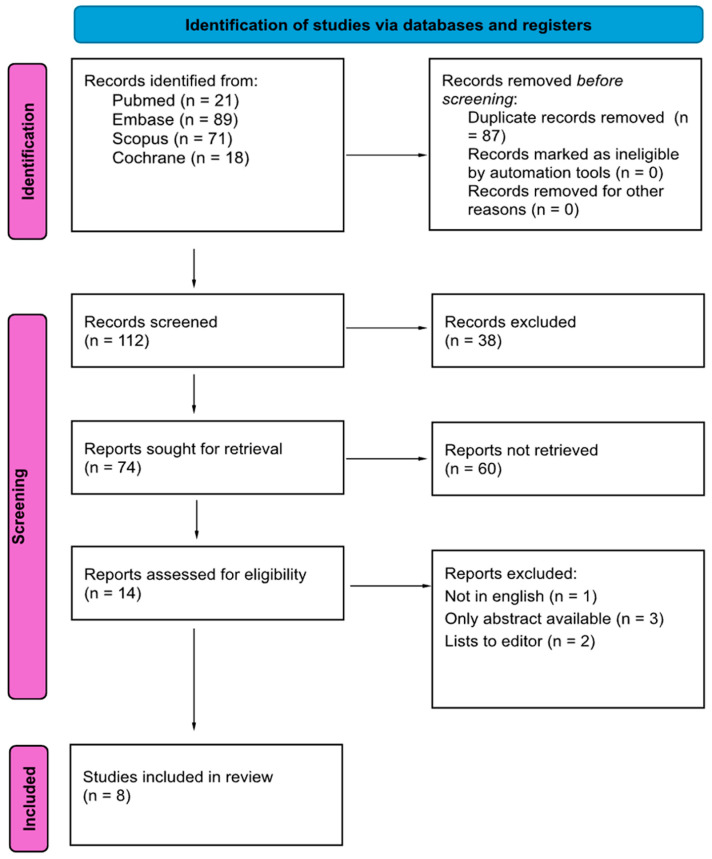 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOral Health Pathology and Treatment · Dermatologic Treatments and Research · Laser Applications in Dentistry and Medicine
1. Introduction
1.1. Rationale—Oral Lichen Planus
Oral lichen planus (OLP) is a chronic immune-mediated mucocutaneous disorder that affects the oral mucosa and commonly presents as reticular white striae, erythematous areas, or painful erosive and ulcerative lesions that significantly impair quality of life [1,2,3]. Although reticular OLP may remain asymptomatic, erosive forms often produce persistent burning sensations and pain, limiting patients’ ability to eat, speak, and maintain oral function. Diagnosis is typically based on characteristic clinical features supported by histopathological findings, including basal cell degeneration, a band-like lymphocytic infiltrate, and epithelial hyperkeratosis [4,5,6]. The etiology of OLP is multifactorial, yet it is widely accepted as a T-cell-mediated autoimmune disease, in which cytotoxic lymphocytes induce apoptosis of basal keratinocytes and perpetuate chronic inflammation [5,6,7]. Psychological stress, systemic comorbidities, medications, dental materials, and infectious agents also contribute to disease onset and persistence [7,8]. Conventional treatment relies primarily on topical or systemic corticosteroids, which reduce inflammation and provide symptomatic relief but are associated with adverse effects such as mucosal atrophy, opportunistic infections, systemic absorption, and limitations in long term use [9,10]. Because many patients require prolonged or repeated therapy, and because disease recurrence is common, interest has grown in alternative modalities capable of providing effective and sustained management with fewer complications.
1.2. Rationale—Lasers
High-power lasers have emerged as promising therapeutic options for OLP due to their ability to precisely ablate diseased epithelial tissue, reduce local inflammatory burden, and promote re-epithelialization while minimizing damage to adjacent structures. Carbon dioxide lasers, operating at 10,600 nm, have been widely used in oral soft tissue surgery because of their ability to vaporize superficial lesions efficiently and achieve excellent hemostasis with minimal thermal diffusion [11,12,13]. Erbium-doped lasers, such as the Er:YAG system, provide similarly precise ablation due to their strong absorption in water, resulting in controlled removal of affected tissue with limited collateral effects [13,14,15,16,17,18,19]. Nd:YAG lasers, with their deeper penetration and coagulative properties, have also been investigated for symptomatic relief in erosive and mixed-type OLP lesions. Evidence from clinical trials and observational studies supports the usefulness of these systems across different clinical presentations of OLP. CO_2_ lasers have demonstrated meaningful reductions in lesion size, symptom severity, and recurrence in erosive and atrophic lesions, outperforming or equaling conventional corticosteroids in several studies. Er:YAG and Nd:YAG lasers have shown benefit in improving lesion characteristics and pain scores, either alone or in combination with pharmacologic therapies, particularly in cases where conventional therapy produced limited results. Long term observational data suggest that CO_2_ laser vaporization may reduce the persistence of erosive lesions and, in some cohorts, correspond with lower rates of malignant transformation when compared with conservative care, although these findings should be interpreted cautiously due to variable follow-up durations and study heterogeneity. Systematic reviews and scoping analyses have further highlighted the value of high-energy lasers in OLP. Additional evidence suggests that erbium-based lasers, alone or in combination with adjunctive modalities such as photodynamic therapy, can improve patient comfort and may reduce recurrence in lesions considered potentially malignant, including certain forms of OLP.
In the context of this review, the term high-energy lasers refers specifically to laser systems capable of producing ablative or coagulative effects on oral mucosal tissues. These include carbon dioxide lasers operating at 10,600 nm, which achieve superficial tissue vaporization with strong hemostasis [19,20]; erbium-based lasers such as Er:YAG (2940 nm), characterized by high absorption in water and controlled ablation with minimal thermal damage [13,14]; and neodymium-doped lasers such as Nd:YAG (1064 nm), which penetrate deeper into tissues and provide significant photothermal and coagulative effects useful in managing erosive and inflammatory OLP lesions [17,20].
1.3. Objectives
This systematic review aims to evaluate the effectiveness of high-power laser therapy, including CO_2_, Er:YAG, and Nd:YAG systems, in the management of oral lichen planus. The objectives are to assess reported outcomes regarding lesion size reduction, pain improvement, recurrence, and safety, while examining how different laser types perform across various clinical forms of OLP. By synthesizing available clinical evidence, this review seeks to clarify the therapeutic role of high-energy lasers and identify gaps for future well-designed randomized controlled trials.
2. Materials and Methods
2.1. Focused Question
A systematic review was conducted following the PICO framework [21], as follows: In patients with oral lichen planus (Population), does treatment with high-power lasers, including CO_2_ and Er lasers (Intervention), compared to conventional therapies such as corticosteroids or no treatment (Comparison), result in greater reduction in lesion size, pain, and recurrence rates (Outcome)?
2.2. Search Strategy
This review has been registered with PROSPERO under the ID CRD42024617677. This systematic review was conducted following the PRISMA 2020 guidelines, with a comprehensive electronic search performed across MEDLINE (via PubMed), Embase, Scopus, and Cochrane Database covering studies published up to 31 December 2024 [22]. The search was conducted in April 2025. The search terms, detailed in Table S1, included a wide range of keywords related to high-power lasers (e.g., CO_2_, Er:YAG, Nd:YAG lasers) and their application in treating oral lichen planus. Furthermore, the authors conducted a “snowball” search to identify additional studies by examining the bibliographies of publications selected for full-text review, and Google Scholar was employed to corroborate the veracity of the cited studies. The electronic search was limited to studies published in English to comply with the inclusion criteria. The databases were searched by three authors (W.N., R.W., J.F-R.) using identical sets of search terms. Once potential studies were identified, all authors collectively reviewed them to ensure their suitability for inclusion. To collate the data from the included studies, two authors (W.N. and R.W.) conducted a collaborative literature search to gather the necessary data.
2.3. Outcome Measures
The primary outcomes assessed were lesion size, clinical severity, and pain intensity. Lesion size was measured either as diameter or surface area using calibrated photographs or direct intraoral measurements. Clinical severity was evaluated through standardized scoring systems such as the Thongprasom sign score and the REU index. Pain intensity was recorded using Visual Analogue or Numeric Rating Scales at baseline and follow-up. Secondary outcomes included recurrence, healing time, inflammatory biomarkers, adverse effects, and patient satisfaction. Recurrence was defined as the reappearance of symptomatic or clinically detectable lesions during follow-up. Healing time reflected the duration required for complete epithelialization of the treated area. When measured, inflammatory cytokines were quantified using laboratory assays. Adverse effects were documented based on clinical observation or patient report. Patient satisfaction was assessed through questionnaires or verbal feedback regarding comfort and treatment response.
2.4. Selection of Studies
This systematic review aimed to investigate the effectiveness of high-power laser therapy, including CO_2_ and Er:YAG lasers, in treating oral lichen planus. The criteria for study inclusion and exclusion are outlined in Table 1.
2.5. Risk of Bias in Individual Studies
During the initial phase of study selection, each reviewer independently evaluated titles and abstracts to minimize potential biases in the assessment process. Cohen’s κ test was used to measure the degree of inter-reviewer agreement [23]. Any disagreements concerning the inclusion or exclusion of studies were resolved through discussion among the authors until a consensus was achieved.
2.6. Quality Assessment and Risk of Bias Across Studies
Two independent reviewers, W.N. and J.F-R., conducted quality assessments of the included studies, focusing on key methodological criteria: random allocation of participants, balanced study and control groups within a 10% margin, use of a power meter to ensure accurate laser settings, clearly defined inclusion and exclusion criteria, confirmation of diagnosis through both clinical and histopathological methods, and assurance that the source of funding did not interfere with the study results. Studies scoring 3 points or less were classified as having a high risk of bias, those scoring 4–6 points as moderate risk, and those scoring 7 or more points as low risk. Any discrepancies in scoring were resolved through discussion to reach a consensus.
2.7. Data Extraction
After reaching a consensus on the selection of included articles, the two reviewers (J.F-R and W.N.) extracted data on the following:
Study Details: Author, year, and study design.Participants: Sample size, gender distribution, and age range.Treatment Types: Interventions compared (e.g., CO_2_ laser vs. corticosteroids).Laser Parameters: Wavelength and power output of lasers used.Outcome Measures:Follow-up: Duration of follow-up periods.Adverse Effects: Notable side effects or complications observed.
3. Results
3.1. Study Selection
Figure 1 provides a detailed flowchart of the research methodology, developed in alignment with PRISMA guidelines. The initial database search identified 199 articles, which were reduced to 112 after removing duplicates. Following the screening of titles and abstracts, 14 studies were deemed eligible for full-text review. Of these, 6 studies were excluded due to the following reasons: the language of the article was not English, the full text versions of the article were not available, or the article was a letter to the editor. Ultimately, the review incorporated 8 studies, all published within the past 16 years (2008–2024).
3.2. Risk of Bias and Quality Assessment of Evidence Results
Each study’s risk of bias was systematically assessed, with an overall rating (low, moderate, or high) assigned according to the guidelines from the Cochrane Handbook for Systematic Reviews of Interventions [24]. Among the eight included studies, none were classified as having a high risk of bias. Six studies earned eight points, while two scored seven points. Although none of the studies achieved the maximum score of nine, no exclusions were made based on quality concerns, as the omitted information was deemed non-critical for the thorough evaluation of the literature. A single point was allocated for each criterion met, whereas negative or ambiguous responses did not contribute additional points. A detailed breakdown of the criteria and the respective scores for each study is presented in Table 2.
The quality of evidence for various therapeutic interventions was evaluated using the GRADE guidelines provided by Cochrane [24], revealing significant variability (Table 3). For reduction in lesion size and pain relief, both supported by seven studies (RCTs and clinical trials), the evidence was rated as low due to moderate inconsistency and moderate imprecision [25,26,27,28,29,30,31,32]. Recurrence rates, assessed across five studies, demonstrated moderate-quality evidence, with imprecision being the primary concern [25,26,28,29,32]. Adverse effects, derived from two studies, also showed moderate-quality evidence, limited by moderate imprecision [26,32]. Patient satisfaction, informed by four studies, was rated as low quality due to moderate inconsistency and imprecision. These findings emphasize the varying levels of certainty across outcomes and highlight the need for more robust and precise research [25,28,31,32].
3.3. General Characteristics of the Included Studies
Out of the eight studies included, two explicitly calculated the required sample size before commencing the study, with methods such as balanced block randomization or statistical tools like G*Power (https://www.g-power.com/en/). The sample sizes varied significantly, ranging from 16 to 171 participants. The gender distribution was generally skewed towards female participants, with female-to-male ratios ranging from 3:1 to nearly equal in some studies. The mean ages of participants varied across studies, ranging from 44.8 ± 12.6 years to 62 years, with age ranges spanning from 24 to 78 years. Notably, only one study, conducted by Ibrahim et al. (2024) [26], employed a split-mouth design, while the rest followed other clinical trial methodologies. Detailed information regarding study designs, sample sizes, and demographic distributions is summarized in Table 4 and Table 5.
3.4. Main Study Outcomes
3.4.1. Lesion Size Reduction
Across the included studies, lesion size was evaluated using linear measurements, surface area estimation, the Thongprasom sign score, or the REU index [25,26,27,28,29,30,31,32]. CO_2_ laser therapy consistently produced measurable reductions in lesion dimensions during follow-up, with several studies reporting progressive decreases in clinical severity scores after vaporization [25,26,27,28,29]. Trials comparing CO_2_ lasers with corticosteroids showed greater reductions in lesion area and REU or TSS scores in the laser group [26,29]. Nd:YAG and Er:YAG lasers also demonstrated favorable effects on lesion contraction, particularly in erosive and atrophic forms, although outcomes varied according to baseline lesion characteristics and energy parameters [27,30,31]. Long-term observational data indicated sustained lesion regression following CO_2_ laser therapy, with most treated sites maintaining clinical improvement for years [32].
3.4.2. Pain Reduction
Pain was assessed using the Visual Analogue Scale or Numeric Rating Scale across all comparative and single-arm trials [25,26,27,28,29,30,31,32]. High-energy lasers produced rapid and marked improvements in pain scores, often noted within weeks of treatment [25,28]. CO_2_ laser therapy resulted in significant reductions in pain intensity and greater symptomatic relief compared with intralesional corticosteroid injections in split-mouth analyses [26]. Nd:YAG lasers produced significant decreases in pain when used alone or combined with systemic agents such as total glucosides of paeony [27,30]. Single-arm CO_2_ studies also reported consistent pain reduction over extended follow-up periods, with sustained symptom control observed up to one year or longer [28,32].
3.4.3. Recurrence
Recurrence was defined as the reappearance of symptomatic or clinically detectable lesions following initial healing. Studies with follow-up intervals ranging from three months to one year showed lower recurrence rates in laser-treated groups compared with corticosteroid controls [26,29]. Split mouth comparisons demonstrated considerably longer remission periods after CO_2_ laser vaporization than with pharmacologic therapy [26]. Long term observational research, including follow-up periods extending up to eighteen years, revealed recurrence patterns similar to shorter studies, with most recurrent lesions appearing as asymptomatic or reticular forms rather than erosive lesions [32]. Er:YAG and Nd:YAG lasers likewise demonstrated reduced recurrence in multi-arm trials, though outcomes varied with lesion morphology and device parameters [31].
3.4.4. Secondary Outcomes
Adverse effects were generally mild across studies and included transient postoperative discomfort and short healing times [25,26,27,28,29,30,31,32]. Epithelialization time varied with laser type, with Er:YAG treatments producing rapid re-epithelialization and Nd:YAG treatments requiring slightly longer intervals [31]. In the only study measuring inflammatory biomarkers, reductions in IL-1β, IL-6, and IFN-γ accompanied clinical improvement following high-energy laser ablation [31]. Where evaluated, patient satisfaction was high, with most patients reporting improved comfort and willingness to undergo the same treatment again [25,28,31,32].
Table 6 and Table 7 further summarize the results.
4. Discussion
4.1. Results in the Context of Other Evidence
This systematic review aimed to evaluate the effectiveness of high-power lasers, including CO_2_, Er:YAG, and Nd:YAG systems, in reducing lesion size, alleviating pain, and lowering recurrence rates in oral lichen planus. Across the eight included studies, the findings consistently indicate that high-energy laser therapy provides meaningful clinical benefits and represents an alternative or adjunct to conventional treatments, particularly for refractory or symptomatic erosive forms of OLP. The primary outcome of lesion size reduction was achieved across all laser types, with the strongest evidence supporting CO_2_ lasers. CO_2_ vaporization resulted in marked decreases in lesion dimensions and clinical severity scores, often outperforming corticosteroids in randomized comparisons [25,26,27,28,29]. Ibrahim et al. reported significantly greater improvements in REU and TSS scores with CO_2_ laser vaporization than with intralesional triamcinolone [26], while long-term observational data by Mücke et al. and Van der Hem et al. reinforced the durability of these responses [29,32]. Nd:YAG and Er:YAG lasers also contributed to lesion reduction, particularly in erosive and atrophic lesions, although effects varied depending on energy parameters and baseline presentation [27,30,31]. These results support the underlying rationale for laser ablation, as precise removal of altered epithelium diminishes the inflammatory infiltrate and promotes tissue regeneration [26,30]. Pain reduction, another key outcome, was consistently observed following high-power laser therapy. Both CO_2_ and Nd:YAG lasers rapidly decreased pain intensity as measured by VAS or NRS across all trials [25,26,27,28,29,30,31,32]. The split-mouth trial by Ibrahim et al. showed that while both CO_2_ vaporization and corticosteroids alleviated pain, CO_2_ therapy produced earlier symptomatic relief and longer-lasting comfort [26]. Nd:YAG lasers yielded comparable benefits even in the absence of adjunctive pharmacologic therapy [27], and combination protocols integrating Nd:YAG with total glucosides of paeony demonstrated enhanced analgesic response [30]. Sustained decreases in pain scores over long follow-up periods further underscore the symptomatic value of high-energy laser treatment [28,32]. Recurrence, a clinically significant concern in OLP, occurred less frequently following laser therapy than with conventional treatments. CO_2_ vaporization produced longer remission intervals and significantly reduced recurrence rates compared with corticosteroids, as shown in the split-mouth trial by Ibrahim et al. [26]. Observational data spanning up to eighteen years demonstrated that most recurrences following CO_2_ laser treatment were mild, reticular, and often asymptomatic [29,32]. Er:YAG and Nd:YAG lasers also showed promise in lowering recurrence, though findings were influenced by lesion morphology, laser mode, and patient adherence [31]. These results align with broader observations from scoping and systematic reviews suggesting that high-energy lasers can mitigate recurrence and maintain extended disease control [33,34,35,36,37,38]. Safety and tolerability outcomes were uniformly favorable. Adverse effects were mild and transient across all studies, typically limited to temporary discomfort or short healing intervals [25,26,27,28,29,30,31,32]. Healing time varied by wavelength, with Er:YAG generally enabling faster epithelialization than Nd:YAG [31]. Tarasenko et al. demonstrated reductions in inflammatory cytokines (IL-1β, IL-6, IFN-γ) following laser treatment, providing biological evidence of reduced inflammatory activity and correlating with symptomatic improvement [31]. Patient satisfaction, where assessed, was consistently high, reflecting the appeal of a minimally invasive treatment that avoids the systemic side effects associated with repeated corticosteroid use [25,28,31,32]. The discussion of laser therapy must also consider implications for malignant transformation. As OLP is classified as an oral potentially malignant disorder, long-term oncologic safety is essential [7]. Although only a minority of studies addressed this outcome directly, the available data are reassuring. Mücke et al. observed a lower frequency of squamous cell carcinoma among patients treated with CO_2_ vaporization compared with those receiving only symptomatic management, though heterogeneity in follow-up complicates definitive interpretation [29]. Similarly, Van der Hem et al. reported no malignant progression at treated sites throughout an average of eight years of observation [32]. While these findings suggest that laser therapy does not increase malignant risk and may, in some cases, reduce it, the evidence remains insufficient to draw firm conclusions. The broader literature supports the findings of this review. Prior analyses have consistently highlighted the advantages of CO_2_ and erbium-based lasers in reducing symptom burden, lowering recurrence, and improving healing characteristics in OLP [33,34,35,36,37,38,39,40,41]. These complementary findings reinforce the clinical potential of high-energy lasers and align with the results reported here. Overall, the evidence indicates that high-power laser therapy achieves the key objectives of reducing lesion size, improving pain, and decreasing recurrence in OLP while maintaining a favorable safety profile. The precision and selective action of laser devices provide therapeutic advantages consistent with contemporary principles of minimally invasive intervention. However, variability in protocols, small sample sizes, and limited long term comparative data highlight the need for more standardized and robust clinical trials to further define optimal treatment parameters and evaluate outcomes such as malignant transformation and long-term remission durability.
4.2. Limitations of Evidence
An important limitation of this review is the lack of homogeneity in the study designs, laser protocols, and outcome measures. Some studies, such as Agha-Hosseini et al. (2012), employed randomized designs, while others, including Van Der Hem et al. (2008), were non-randomized, increasing the risk of selection bias [25,32]. Additionally, the follow-up periods varied widely, ranging from weeks to several years, complicating comparisons of long-term efficacy. The measurement of outcomes also lacked standardization, relying primarily on subjective metrics like the VAS for pain and the Thongprasom sign score, which, while valuable, are less precise than imaging or histopathological evaluations. Few studies provided detailed descriptions of laser usage, for example, including whether it was applied in contact mode [25,27,29]. Another notable limitation is the small sample sizes across the studies [25,26,27,28,29,30,31,32]. This limitation reduces the statistical power of the findings and increases the risk of random variation influencing results. Furthermore, none of the studies included blood-based biomarkers or advanced imaging to objectively confirm lesion healing, which could have strengthened the findings. The variability in lesion types and locations, ranging from reticular to erosive forms, further complicates the generalizability of the results. Moreover, while lasers generally demonstrated fewer side effects than corticosteroids, the long-term risks, such as malignant transformation, were not adequately assessed in most studies. For instance, Mücke et al. (2015) explored the potential for squamous cell carcinoma transformation but reported inconsistent results due to the varied follow-up durations [29]. Despite these limitations, the findings suggest that high-power laser therapy offers substantial benefits over conventional treatments. Its minimally invasive nature reduced postoperative discomfort, and ability to achieve localized treatment without systemic side effects aligns with the principles of modern dentistry. The inconsistencies in study design and outcomes highlight the need for future research.
4.3. Limitations of Review
A notable limitation of this study is the narrative nature of synthesizing results, which the authors opted not to perform due to a lack of homogeneity among articles, due to significantly different protocols used. The variation in study groups across the reviewed research may have introduced bias, potentially impacting the objective evaluation of the effectiveness of the studies’ lasers. Given the limitations, the authors chose to provide a comprehensive summary of all available trials on the topic, allowing future researchers to identify and address any critical gaps overlooked in individual studies. However, the primary limitation of this review is the small number of randomized trials included. Conducting a systematic review and meta-analysis with a larger pool of relevant studies will be essential to strengthen future research. Interpretation of split-mouth study designs requires care, as intralesional corticosteroid administration, although primarily acting locally, may still undergo partial systemic absorption. This effect can reduce the independence of treatment outcomes between the two sides of the mouth and introduces the possibility of crossover influence. Such systemic diffusion may therefore bias comparisons between laser therapy and corticosteroid treatment in split-mouth trials, and acknowledging this limitation strengthens the interpretation of the resulting data.
4.4. Implications
Future studies should address these limitations by employing standardized protocols, including predefined laser parameters, consistent follow-up durations, and advanced diagnostic tools such as imaging and histopathology. Large-scale, multicenter randomized controlled trials are essential to validate the efficacy of laser therapy and ensure its reliability. Additionally, exploring the combination of laser therapy with pharmacological treatments or regenerative techniques could provide insights into optimizing patient outcomes. While the results of this review are promising, the heterogeneity of study designs, small sample sizes, and short follow-up periods prevent definitive conclusions. Nonetheless, the evidence strongly supports the potential of high-power laser therapy, particularly CO_2_ lasers, in the management of OLP. Future research should focus on addressing these gaps to fully establish lasers as a reliable and effective treatment modality for this chronic condition.
5. Conclusions
This systematic review evaluated the effectiveness of high-power laser therapy, including CO_2_, Er:YAG, and Nd:YAG systems, in reducing lesion size, alleviating pain, and limiting recurrence in oral lichen planus. Across the included studies, high-energy lasers consistently achieved clinically meaningful reductions in lesion severity and pain intensity, often with faster improvement and longer remission than conventional corticosteroid therapy. Recurrence rates were generally lower following CO_2_ vaporization than with pharmacologic treatment, and most relapses observed in long-term follow-up were mild and asymptomatic. Safety outcomes were favorable, with minimal adverse effects and predictable healing profiles across laser types. Although these findings support the therapeutic potential of high-power lasers for managing symptomatic or refractory OLP, the evidence base remains constrained by heterogeneity in study design, small sample sizes, and variability in laser parameters. Consequently, while the existing studies indicate that high-power lasers are a promising treatment modality aligned with contemporary minimally invasive approaches, definitive conclusions about their comparative superiority and long-term oncologic safety cannot yet be drawn. Future research should prioritize standardized treatment protocols, consistent outcome measures, and adequately powered randomized trials to clarify the optimal indications and long term benefits of laser therapy. By addressing these gaps, forthcoming studies may firmly establish high-power lasers as a reliable, evidence-based option for improving clinical outcomes in patients with oral lichen planus.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Raj G. Raj M. Oral Lichen Planus Stat Pearls [Internet]Stat Pearls Publishing Treasure Island, FL, USA 2024 Available online: https://www.ncbi.nlm.nih.gov/books/NBK 578201/(accessed on 1 January 2025)
- 2Gupta S. Jawanda M.K. Oral Lichen Planus: An Update on Etiology, Pathogenesis, Clinical Presentation, Diagnosis and Management Indian J. Dermatol.20156022222910.4103/0019-5154.15631526120146 PMC 4458931 · doi ↗ · pubmed ↗
- 3Hashemipour M.A. Sheikhhoseini S. Afshari Z. Nassab A.R.G. The relationship between clinical symptoms of oral lichen planus and quality of life related to oral health BMC Oral Health 20242455610.1186/s 12903-024-04326-238735922 PMC 11089796 · doi ↗ · pubmed ↗
- 4Nukaly H.Y. Halawani I.R. Alghamdi S.M.S. Alruwaili A.G. Binhezaim A. Algahamdi R.A.A. Alzahrani R.A.J. Alharamlah F.S.S. Aldumkh S.H.S. Alasqah H.M.A. Oral Lichen Planus: A Narrative Review Navigating Etiologies, Clinical Manifestations, Diagnostics, and Therapeutic Approaches J. Clin. Med.202413528010.3390/jcm 1317528039274493 PMC 11396719 · doi ↗ · pubmed ↗
- 5Lavanya N. Jayanthi P. Rao U.K. Ranganathan K. Oral lichen planus: An update on pathogenesis and treatment J. Oral Maxillofac. Pathol.20111512713210.4103/0973-029X.8447422529568 PMC 3329692 · doi ↗ · pubmed ↗
- 6Popa C. Sciuca A.M. Onofrei B.A. Toader S. Condurache Hritcu O.M. Boțoc Colac C. Andrese E.P. Brănișteanu D.E. Toader M.P. Integrative Approaches for the Diagnosis and Management of Erosive Oral Lichen Planus Diagnostics 20241469210.3390/diagnostics 1407069238611605 PMC 11011293 · doi ↗ · pubmed ↗
- 7Manchanda Y. Rathi S.K. Joshi A. Das S. Oral Lichen Planus: An Updated Review of Etiopathogenesis, Clinical Presentation, and Management Indian Dermatol. Online J.20231582310.4103/idoj.idoj_652_2238283029 PMC 10810384 · doi ↗ · pubmed ↗
- 8Borba Filla J. Fontanelli A.F. Brown M.A. Naval Machado M.A. Treatment of Symptomatic Oral Lichen Planus: A Literature Review Pol. Przegląd Otorynolaryngologiczny 201653035