Local Pharmacological Interventions for Pain Relief During Peripheral Venous Cannulation: A Systematic Review with Implications for Clinical Nursing Practice
Aleksandra Maruszak, Damian Romańczuk, Sandra Lange, Wioletta Mędrzycka-Dąbrowska, Grzegorz Cichowlas, Anna Gąsior

TL;DR
This paper reviews local pain-relief methods for reducing discomfort during IV needle insertion in adults and finds them effective and safe for clinical use.
Contribution
The study systematically evaluates the effectiveness and feasibility of local pharmacological interventions for pain reduction during venous cannulation.
Findings
Local pharmacological interventions like vapocoolant sprays and topical anesthetics significantly reduce procedural pain during cannulation.
These interventions improve patient satisfaction and have a favorable safety profile.
Implementation of these methods in clinical practice is influenced by practical and organizational factors.
Abstract
Background/Objectives: Peripheral venous cannulation is one of the most frequently performed invasive procedures in adult patients and is often associated with procedural pain. Despite the availability of various pain-reduction strategies, analgesia during cannulation is not consistently implemented in routine clinical practice. The aim of this review was to identify local pharmacological interventions recommended for reducing procedural pain during peripheral venous cannulation, to assess their clinical effectiveness, and to determine which interventions may be feasibly incorporated into everyday clinical practice. Methods: A literature review was conducted including randomized controlled trials, prospective studies, and meta-analyses involving adult patients undergoing peripheral venous cannulation. Outcomes of interest included procedural pain intensity, clinical effectiveness of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
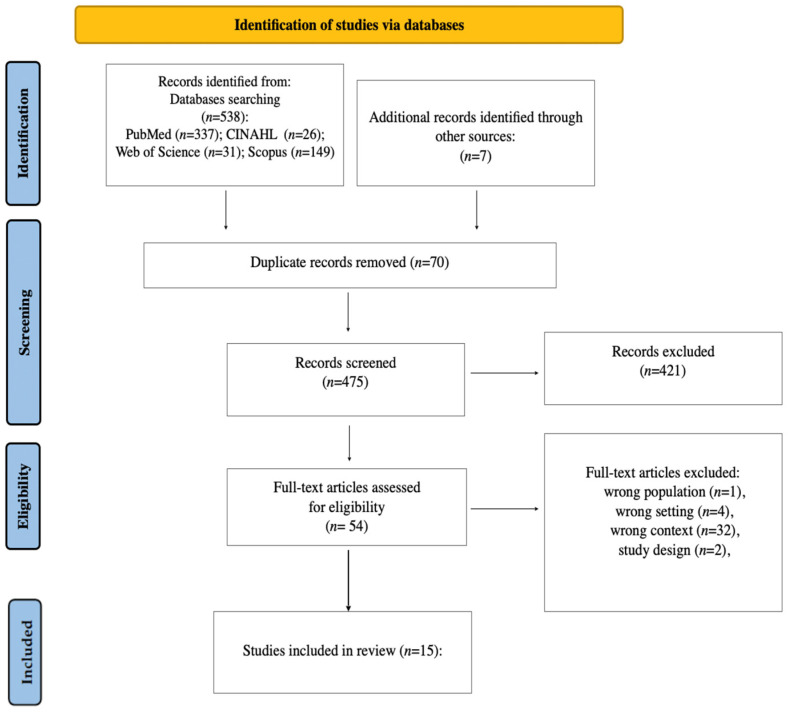 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPediatric Pain Management Techniques · Central Venous Catheters and Hemodialysis · Pain Management and Opioid Use
1. Introduction
Intravenous catheter insertion is one of the most frequently performed procedures in hospitals and outpatient clinics, becoming a standard component of patient care. Although the procedure is considered routine by medical staff, for many patients it represents a significant source of stress, anxiety, and pain. Unpleasant experiences associated with cannulation may affect not only the patient’s subjective comfort but also their cooperation during the procedure, consequently influencing its effectiveness and safety. Procedural pain may trigger physiological responses such as increased heart rate, elevated blood pressure, and increased cortisol levels. For this reason, effective pain management and stress-reduction strategies are essential in clinical practice. Both pharmacological and non-pharmacological methods are used to divert attention and minimize the procedural pain associated with cannulation. The choice of an appropriate method depends on the type of procedure, the patient’s age, clinical condition, and the availability of resources [1,2,3,4,5,6]. The use of pharmacological local-anesthetic methods enables effective reduction in procedure-related pain; however, their selection depends on factors such as onset and duration of action, method of administration, potential adverse effects, availability of agents, and individual patient preferences. Additionally, effective pain control contributes to improved hospitalization experiences, enhances patient trust in medical staff, and may reduce the development of anxiety related to future medical procedures. In recent years, increasing attention has been directed toward studies comparing different local anesthesia strategies and non-pharmacological techniques in order to identify the most effective and best-tolerated approaches for patients [7,8,9,10,11,12]. Although several systematic reviews and meta-analyses have evaluated the efficacy of vapocoolants and topical anesthetics, limited attention has been given to how these interventions can be implemented in routine clinical and nursing practice across different healthcare systems. In particular, evidence addressing organizational constraints, staff training, and availability of pharmacological agents in Central and Eastern European settings remains scarce [13,14,15,16]. This review aims not only to synthesize recent clinical evidence (2015–2025) but also to highlight practical and contextual factors influencing the feasibility of pain-reducing interventions during peripheral venous cannulation.
Aim
The aim of this review is to identify which local pharmacological interventions are recommended during peripheral venous cannulation to reduce procedural pain, to evaluate their clinical effectiveness, and to determine which of these interventions can be incorporated into routine clinical practice.
The research questions were:
Q1: What level of pain intensity is experienced during peripheral vascular cannulation?
Q2: Which local pharmacological interventions are recommended during peripheral vascular cannulation in adult patients
Q3: What is the clinical effectiveness of these interventions?
Q4: Do these interventions affect other outcomes, such as patient satisfaction, anxiety, or safety, or provide additional benefits?
2. Methods
2.1. Study Design
This systematic review of the literature was guided by the Joanna Briggs Institute critical appraisal tools for use in JBI Systematic Reviews [17,18], and was conducted following the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [19] (Supplementary Materials).
2.2. Search Strategy
The following databases were searched: PubMed, CINAHL, Web of Science, and Scopus. The following keywords were used: adults, outpatients, inpatients, ‘Peripheral Catheterization’, Venipuncture, ‘peripheral intravenous catheter’ OR ‘venous access’ OR ‘PIVC’, ‘IV insertion’, ‘Pain Management’, ‘Analgesia’, ‘Pain Reduction’, ‘Pain Prevention’, ‘Pain relief’, intervention, pharmacological, EMLA, ‘topical anesthetics’. Keywords were entered along with their combinations using AND or OR. Search strategies applied to the search are presented in Table 1. The number of articles found during each search test was limited to studies conducted between 2015 and 2025. The final search was carried out on 25 December 2025.
Two reviewers independently screened all titles and abstracts for eligibility. Full-text articles were independently assessed based on predefined inclusion and exclusion criteria. All publications were analyzed by title and abstract to exclude duplicates and irrelevant entries. Full-text articles were then read and critically evaluated according to the eligibility criteria (PICO framework and inclusion/exclusion criteria). The reference lists of studies identified during the initial search were also screened to ensure that no relevant research was overlooked. The PICO framework and all of the inclusion and exclusion criteria applied to the search are presented in Table 2 and Table 3. Disagreements were resolved through discussion, and when necessary, a third reviewer was consulted.
We included only studies evaluating local pharmacological interventions for pain reduction during peripheral venous cannulation in adults. Studies evaluating exclusively non-pharmacological interventions (e.g., distraction, audiovisual techniques, vibration devices) were excluded.
2.3. Data Extraction
Data were extracted by AM, WMD. The following information was extracted: author (year), study design, sample size, setting, intervention, description of intervention, outcome measures, pain scale used, and results.
2.4. Data Synthesis
A quantitative meta-analysis was not performed due to substantial clinical and methodological heterogeneity across the included studies. This included the use of different pain assessment scales (NRS, VAS, and VRS), variability in pharmacological agents, differences in application timing and dosage, variation in cannula sizes and clinical settings, and inconsistent outcome reporting. Therefore, pooling of effect sizes and formal statistical heterogeneity assessment (e.g., I^2^ statistics) was not methodologically appropriate, and a structured narrative synthesis was adopted. In addition, a structured narrative approach was selected to enhance clinical interpretability and practical applicability of the findings for routine nursing and clinical practice.
2.5. Quality Assessment
Two researchers independently assessed the quality of the included studies. The critical appraisal tools used to assess quality were JBI Checklists for randomized controlled trials [19]. The score was divided into three categories: high, moderate, and low (Table 4). A point was only awarded if the answer to a question from the tool was ‘Yes’. Any discrepancies were resolved through discussion until consensus was reached.
Of the 15 included studies, 10 were classified as high-quality, four as moderate-quality, and one as low-quality according to the JBI critical appraisal tools. The most frequent sources of potential bias were the lack of blinding of participants and personnel, as well as unclear allocation concealment. These methodological limitations may reduce the strength of causal inferences drawn from some studies.
2.6. Ethical Approval
Since this study was a systematic review, ethical approval was not required.
3. Results
3.1. Study Selection
The database search resulted in a total of 538 articles. A total of 70 duplicates and 423 articles were removed after abstract review. After full-text analysis of articles, 39 studies were removed due to having the wrong population, wrong setting, wrong context, or study design. A total of 15 studies with randomized controlled trials were included in the analysis (Figure 1). The studies were conducted in Germany (n = 2), USA (n = 5), Iran (n = 3), Japan (n = 2), Denmark (n = 1), Turkey (n = 1) and India (n = 1).
3.2. Characteristics of Included Studies
Rather than reproducing the content of Table 5 in narrative form, this section provides a higher-level synthesis of findings across studies, highlighting consistent patterns and clinically relevant trends in pain reduction.
3.3. Pain Intensity During Peripheral Venous Cannulation
To improve comparability across studies, results were grouped by pain assessment scale (NRS, VAS, and VRS) and by type of pharmacological intervention rather than directly compared across all studies. This approach reflects differences in scale properties and reporting formats that precluded standardized quantitative pooling. In the studies analyzed above, pain intensity associated with peripheral venous cannulation was most commonly assessed using the Numerical Rating Scale (NRS) and the Visual Analogue Scale (VAS). In control groups receiving placebo or no intervention, pain intensity was generally moderate and ranged from NRS 3 to 6, whereas in groups receiving pain-reducing interventions it ranged from NRS 2 to 4 [2,5,6,13,14]. In groups in which vapocoolant spray, cryospray, or ethyl chloride was used, pain intensity was lower, typically NRS 1–2, compared with NRS 3 to 5 in control groups [2,5,7,9,13]. The use of topical local anesthetics in the form of creams or patches was also associated with low pain scores. In randomized studies, mean pain intensity in intervention groups ranged from NRS 1.5 to 2, compared with approximately NRS 3 in placebo groups [15]. In the study by Yoshida et al., pain assessed using the VAS was 2 in the group receiving a lidocaine–prilocaine patch, whereas a value of 4 was reported in the group receiving injectable lidocaine [6]. Pain intensity was also dependent on the size of the cannula used during the procedure. In a comparative study, pain intensity in the control group was NRS 5 for 17G cannulas and NRS 3 for 20G cannulas. In the intervention group, corresponding values were NRS 2 to 3 and NRS 1 to 2, respectively [2,12].
3.4. Pharmacological Interventions Recommended During Peripheral Venous Cannulation
The presented studies evaluated several pharmacological methods aimed at reducing pain during peripheral venous cannulation. The most frequently analyzed interventions included:
- Cryotherapy, including vapocoolant spray, ethyl chloride and cryospray. These interventions do not require injection and are characterized by a very rapid onset of action [2,3,5,9,13].
- Topical local anesthetics in the form of creams or patches, including EMLA cream, tetracaine gel, topical ketamine and diclofenac patches. These agents also do not require disruption of skin integrity; however, their effectiveness depends on the duration of application on the skin [2,6,11,16].
- Injectable lidocaine, which is an effective local anesthetic but requires disruption of skin continuity and may therefore cause additional procedural pain [2,6].
3.5. Clinical Effectiveness of the Interventions
Interventions involving cryotherapy demonstrated largely consistent and clinically noticeable effects across most studies, with a typical reduction in pain intensity of approximately 1 to 2 points on the NRS. According to published thresholds for minimal clinically important difference (MCID) in acute procedural pain, a reduction of approximately 1.3–2.0 points on numerical or visual analog scales is generally considered clinically meaningful. Therefore, while several interventions achieved changes likely to be perceived as beneficial by patients, some reported differences may represent only marginal clinical improvement.
Vapocoolant vs. placebo: NRS 2 vs. 4 [13].Vapocoolant vs. placebo (venipuncture): NRS 1 vs. 3 [5,7].Ethyl chloride vs. placebo: NRS 2 vs. 4 [2].Cryospray vs. control group: NRS 1 vs. 3 [9].
It should be noted, however, that not all studies demonstrated a clinically significant effect. In the study by Edwards et al. 2017, the difference between the intervention and placebo groups was small and not clinically significant: NRS 2 vs. 2.5 [10].
2.EMLA cream, lidocaine–prilocaine patch, topical ketamine, injectable lidocaine
EMLA vs. placebo: 1.66–1.11 vs. 1.9–3.16—effect depending on application time and study population [15].Lidocaine–prilocaine vs. injectable lidocaine: VAS 2 vs. 4 [6].Topical ketamine: In the study by Heydari et al., both topical ketamine and EMLA produced similar pain scores, NRS 1.7, and were more effective than placebo, NRS 3.16 [3].
3.6. Interventions and Their IMPACT on Other Outcomes (e.g., Satisfaction, Anxiety, Safety)/Other Benefits
In the analyzed studies, in addition to pain intensity, other clinical outcomes were also assessed. The most frequently reported outcomes included patient satisfaction, safety of the applied interventions, and their impact on the technical aspects of cannulation [7]. Studies comparing vapocoolant spray, cryospray, or ethyl chloride with placebo or no intervention demonstrated that the use of these methods was associated with higher patient-reported satisfaction and a greater willingness to use the same method again in the future [5,7,9]. In some studies, positive evaluations of the procedure by healthcare staff were also reported, with no significant differences observed in first-attempt success rates or the technical difficulty of cannulation [3,7]. The use of topical local anesthetics in the form of creams or patches, particularly lidocaine–prilocaine (EMLA), was associated with high patient satisfaction and low procedural pain scores; however, some studies indicated a longer preparation time for cannulation due to the need for an adequate application period [16]. In studies comparing lidocaine–prilocaine patches with injectable lidocaine, the transdermal form was rated as more comfortable, mainly due to the absence of additional pain related to anesthetic injection [6]. With regard to safety, the majority of the analyzed studies did not report clinically significant adverse events related to the applied interventions. Vapocoolant spray and cryospray were generally well tolerated, and reported adverse effects were mild and transient [5,9].
4. Discussion
The aim of this review was to identify local pharmacological interventions recommended during peripheral venous cannulation to reduce procedural pain, to assess their clinical effectiveness, and to determine which of these interventions may be incorporated into routine clinical practice. The results of the analysis allowed answers to be provided to the formulated research questions. Overall, the observed pattern of modest but generally clinically meaningful pain reduction suggests that the choice of intervention should be guided not only by efficacy but also by feasibility, availability, and workflow integration in routine clinical settings. Common methodological weaknesses across the included studies included small sample sizes, lack of participant and assessor blinding, unclear allocation concealment, and variability in cannula size and clinical context. These limitations increase the risk of bias and reduce confidence in the precision of reported effect estimates.
The analysis of the included studies demonstrated that peripheral venous cannulation in adult patients is most commonly associated with moderate-intensity pain, as confirmed by multiple studies [2,5,10,13]. Pain intensity varied depending on the clinical context and technical parameters, particularly cannula size, with larger cannulas being associated with higher pain levels [2,12]. These findings indicate that cannulation should not be regarded as a pain-neutral procedure.
Various local pharmacological interventions were evaluated in the analyzed studies [2,4]. The lack of a unified standard of care highlights the need to tailor analgesic methods to organizational and clinical conditions. In many countries, nurses have the authority to independently apply selected local-analgesic methods, whereas in Poland the scope of such competencies is more limited, which may hinder the routine implementation of effective interventions.
Most of the analyzed interventions demonstrated significant effectiveness in reducing procedural pain compared with placebo or no intervention. The most consistent effects were observed with the use of vapocoolants and topical local anesthetics in cream or patch form [2,3,5,9,15]. The effectiveness of vapocoolant spray was additionally confirmed in a meta-analysis [2]. Injectable lidocaine also showed an analgesic effect; however, its use was associated with additional pain related to the injection itself [6]. These differences support the need for individualized selection of analgesic interventions.
Beyond pain reduction, the interventions also influenced other clinical outcomes, particularly patient satisfaction and procedure safety [7,9].
The conducted review indicates that local pharmacological interventions are effective and safe in reducing pain during peripheral venous cannulation and may be integrated into routine clinical practice. In particular, vapocoolant sprays and topical anesthetics in cream or patch form appear to be feasible options for widespread use. In the context of the Polish healthcare system, these findings support consideration of expanding nurses’ competencies regarding the independent use of selected local-analgesic methods, which could contribute to improved quality of care, patient comfort, and standardization of procedural pain management. Accordingly, the strength of the recommendations derived from this review should be aligned with the overall quality of the evidence, which ranged from moderate to high but was limited by methodological heterogeneity and risk of bias in several studies.
Our findings are broadly consistent with recent systematic reviews and meta-analyses reporting modest but clinically relevant reductions in pain associated with vapocoolant sprays and topical anesthetics. However, compared with these prior reviews, which often emphasize pooled effect estimates under controlled conditions, the present review highlights greater variability in effectiveness across real-world clinical settings, likely driven by differences in application protocols, staff training, and organizational constraints.
5. Limitations
When interpreting the results of this analysis, several limitations should be considered. The included studies differed in terms of study design, types of interventions, duration of application, and pain assessment scales used. The subjective nature of pain scales may have affected the comparability of results. Additionally, studies conducted outside the Polish healthcare system may limit the direct transferability of some interventions to national clinical practice. This systematic review was not registered in PROSPERO, which may increase the risk of reporting bias and reduce methodological transparency. Furthermore, the absence of pooled effect estimates, formal heterogeneity assessment (e.g., I^2^), sensitivity analyses, and evaluation of publication bias limits the precision and generalizability of the conclusions.
6. Conclusions
Peripheral venous cannulation in adult patients is most commonly associated with moderate-intensity pain and should not be regarded as a pain-neutral procedure.Pharmacological interventions demonstrate significant clinical effectiveness in reducing pain associated with the cannulation procedure.The majority of the analyzed pharmacological interventions are characterized by good patient acceptance and a favorable safety profile.The use of pharmacological interventions prior to peripheral venous cannulation not only reduces pain but also improves patient satisfaction and overall patient experience during hospitalization.
7. Implications for Clinical Practice
The results presented in this article indicate that pharmacological methods for reducing pain during peripheral venous cannulation can and should be integrated into the cannulation procedure in routine clinical practice, particularly in high-demand settings such as emergency departments, operating theaters, and surgical wards. Each of the analyzed interventions is characterized by distinct advantages; therefore, consideration of all available options and selection of the most appropriate method for specific patient populations is recommended. In the context of the Polish healthcare system, the findings of this review may serve as a basis for discussion on expanding the competencies of nurses regarding the independent application of selected analgesic methods. Such an approach could significantly contribute to improving the quality of care, increasing patient comfort and satisfaction, and standardizing the management of procedural pain in clinical practice in Poland.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zhu Y. Peng X. Wang S. Chen W. Liu C. Guo B. Zhao L. Gao Y. Wang K. Lou F. Vapocoolant spray versus placebo spray or no treatment for reducing pain from intravenous cannulation: A meta-analysis of randomized controlled trials Am. J. Emerg. Med.2018362085209210.1016/j.ajem.2018.03.06830253890 · doi ↗ · pubmed ↗
- 2Rüsch D. Koch T. Seel F. Eberhart L. Vapocoolant spray versus lidocaine infiltration for radial artery cannulation: A prospective, randomized, controlled clinical trial J. Cardiothorac. Vasc. Anesth.201731778310.1053/j.jvca.2016.06.00827590462 · doi ↗ · pubmed ↗
- 3Heydari F. Khalilian S. Golshani K. Majidinejad S. Masoumi B. Massoumi A. Topical ketamine as a local anesthetic agent in reducing venipuncture pain: A randomizedcontrolled trial Am. J. Emerg. Med.202148485310.1016/j.ajem.2021.03.05533836388 · doi ↗ · pubmed ↗
- 4Srivastava V.K. Das P.K. Gautam S.K.S. Jaisawal P. Kadiyala V.N. Rambhad S. Comparative evaluation of volatile anesthetic agents for attenuation of venous cannulation pain: A prospective, randomized controlled study J. Clin. Diagn. Res.201610 UC 01UC 0410.7860/JCDR/2016/19970.841227790552 PMC 5072052 · doi ↗ · pubmed ↗
- 5Mace S.E. Prospective, randomized, double-blind controlled trial comparing vapocoolant spray vs placebo spray in adults undergoing venipuncture Am. J. Emerg. Med.20163479880410.1016/j.ajem.2016.01.00226979261 · doi ↗ · pubmed ↗
- 6Yoshida S. Miyasaka K.W. Suzuki R. Fujita N. Abe S. Comparison of analgesic effect of local anesthetic injection for pain relief during peripheral venous insertion in adult surgical patients: A prospective observational study J. Perianesthesia Nurs.20254053153410.1016/j.jopan.2024.06.10839297819 · doi ↗ · pubmed ↗
- 7Barbour T. O’Keefe S. Mace S.E. Patient and health care provider responses from a prospective, double-blind, randomized controlled trial comparing vapocoolant spray versus placebo spray in adults undergoing venipuncture in the emergency department Pain Manag. Nurs.20181939139910.1016/j.pmn.2017.09.00629153919 · doi ↗ · pubmed ↗
- 8Akhgar A. Mazidabadi Farahani A. Akbari H. Sedaghat M. Jalili M. Mirfazaelian H. Comparison of the effects of vapocoolant spray and topical anaesthetic cream (lidocaine-prilocaine) on pain of intravenous cannulation: A randomised controlled trial Emerg. Med. J.20254237337710.1136/emermed-2024-21447940118519 · doi ↗ · pubmed ↗