Early (<6 Days) Extracranial Carotid Revascularization After Intravenous Thrombolysis for Stroke: A Scoping Review
Giovanni Coppi, Luiz Felippe Milazzo, Marco Damiano Pipitone, Giovanni Zambello, Francesco Zaraca, Reinhold Perkmann

TL;DR
This review examines the safety of early carotid surgery after stroke treatment, finding rare complications but needing more research.
Contribution
The study provides a scoping review of early carotid revascularization outcomes after thrombolysis, highlighting gaps in current evidence.
Findings
CEA had lower symptomatic bleeding risk than CAS (1.9% vs. 8.6%).
Most hemorrhages occurred in patients operated within 48–72 h from IVT.
Overall mortality was low at 1.1% with 3.7% wound complications.
Abstract
Background: Current guidelines recommend delaying extracranial carotid revascularization for at least 6–7 days after intravenous thrombolysis (IVT). However, evidence remains inconclusive, and patients with minimal or no brain lesions may benefit from earlier intervention. Objective: This scoping review evaluates outcomes of carotid revascularization performed within six days of IVT in patients with small strokes or no imaging-detected lesions. Design: We searched Medline, EMBASE, and Cochrane CENTRAL for studies published between 2005 and 2025 reporting carotid revascularization after IVT. Primary outcomes included perioperative ischemic stroke, symptomatic intracranial hemorrhage (sICH), asymptomatic intracranial bleeding (aICB), and wound complications. Data on timing, imaging findings (CT/MRI), and stroke severity (NIHSS or modified Rankin scale) were extracted. The review followed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
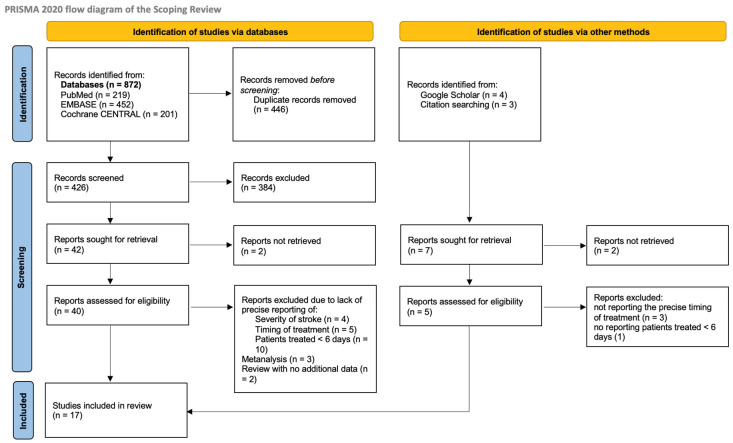 Figure 1
Figure 1| Author | Year | Country | Design of the Study | Population and Sample Size | Intervention Type | |
|---|---|---|---|---|---|---|
| 1 | Bellomo T. et al. [ | 2024 | USA | Retrospective analysis of a single-center cohort (Mass. General Hospital). | 56 stroke pts submitted to carotid revascularization after IVT (4.9%) | 35 CEA, 21 CAS (15 catheter-based interventions for stroke: 9 before CEA and 6 before CAS) |
| 2 | Doo Hyuk Kwon et al. [ | 2022 | Republic of Korea | Retrospective analysis of a cohort of emergent carotid intervention at a single center (Keimyung University School of Medicine). | 19 pts with stroke submitted to emergent CAS after IVT (11 ICA occlusions excluded) | 19 CAS: 11 pts with ICA occlusion, 6 pts with tandem lesion (not considered in the review), 2 pts with ICA stenosis (included in the scoping review) |
| 3 | Johal A.S. et al. [ | 2021 | UK | Retrospective study using a large population-based dataset from the National Vascular Registry in the United Kingdom (UK-NVR). | 1055 stroke pts submitted to IVT and CEA (11.7%) | CEA (patients with CAS or carotid bypass were excluded from the study) |
| 4 | Deiana G. et al. [ | 2020 | Italy | Retrospective analysis of a cohort of patients from two centers (Brotzu Hospital, Cagliari, Italy and Santissima Annunziata Hospital, Sassari, Italy). | 11 stroke pts submitted to CEA after IVT (15.7%) | CEA under locoregional anesthesia in all patients |
| 5 | Ijäs P. et al. [ | 2018 | Finland | Retrospective analysis of a single-center cohort of patients (Helsinki University Hospital, Helsinki, Finland). Comparison between pts operated <48 h after IVT and pts operated >48 h and <14 days. | 128 pts submitted to CEA after IVT (15.7%) | All CEA, no data regarding surgical technique or anesthesia |
| 6 | Gunka I. et al. [ | 2017 | Czech Republic | Retrospective analysis of a single-center cohort of patients (Charles University Hospital, Prague, Czech Repuplic). | 13 pts submitted to CEA after IVT (14%)—4 patients with acute extracranial carotid occlusion | CEA under locoregional anesthesia (general anesthesia in selected patients) |
| 7 | Adachi K. et al. [ | 2017 | Japan | Retrospective analysis of a single-center cohort of patients treated with CAS < 2 wks of stroke | 16 patients undergoing urgent/emergent CAS for stroke/stroke in evolution—4 receiving IVT (25%) | CAS with embolic protection |
| 8 | Yamamoto Y. et al. [ | 2016 | Japan | Case report on emergent CEA after IVT for deteriorating symptoms | One emergent CEA due to fluctuating symptoms | CEA under general anesthesia |
| 9 | Azzini C. et al. [ | 2016 | Italy | Retrospective analysis of a single-center cohort of patients treated with CEA (also <12 h) after IVT | 34 stroke pts submitted to CEA after IVT | CEA under general anesthesia with routine shunt |
| 10 | Bazan H.A. et al. [ | 2015 | USA | Retrospective analysis of a single-center cohort of patients treated with CEA/CAS after IVT | 31 stroke pts submitted to carotid revascularization after IVT | IVT: CEA 25 − CAS 6 |
| 11 | Vellimana A.K. et al. [ | 2014 | USA | Retrospective analysis of a single-center cohort of patients treated with CEA after IVT | 11 stroke pts submitted to carotid revascularization after IVT | CEA under general anesthesia. Intraoperative neuromonitoring with EEG. Selective shunting on EEG indication |
| 12 | Koraen-Smith L. et al. [ | 2014 | Sweden | Retrospective analysis of a prospectively collected national database (Swedvasc and Riks-Stroke). | 79 stroke pts submitted to carotid revascularization after IVT | IVT: CEA 71 − CAS 6 + 2 pts with aborted TEA due to high bifurcation |
| 13 | Yong Y.P. et al. [ | 2013 | UK | Retrospective analysis of a single-center cohort of patients treated with CEA after IVT | Seven stroke pts submitted to CEA after IVT | CEA under locoregional or general anesthesia |
| 14 | Sallustio F. et al. [ | 2012 | Italy | Retrospective analysis of a single-center cohort of patients treated with CAS after IVT | Six stroke pts submitted to CAS after IVT | CAS under local anesthesia with embolic protection device (distal filter) |
| 15 | Leseche G. et al. [ | 2012 | France | Retrospective analysis of a single-center cohort of patients with STROKE IN EVOLUTION | Seven pts with stroke in evolution (fluctuating symptoms) after IVT | CEA under locoregional anesthesia/general anesthesia with routine shunting |
| 16 | Bartoli M.A. et al. [ | 2008 | France | Retrospective analysis of a single-center cohort of patients treated with CEA after IVT | 12 stroke pts submitted to CEA after IVT | IVT: CEA 12 |
| 17 | Abou-Chebl A. et al. [ | 2005 | USA | Retrospective analysis of a single-center cohort of patients treated with CAS after IVT + GPIIb/IIIa Antagonists | 12 stroke pts submitted to emergent endovascular treatment and IVT + GPIIb/IIIa Antagonists (2 patients receiving CAS) | CAS in two patients associated with endovascular treatment of intracranial lesion |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCerebrovascular and Carotid Artery Diseases · Acute Ischemic Stroke Management · Moyamoya disease diagnosis and treatment
1. Introduction
Today, intravenous thrombolysis with rTPA (IVT) is the mainstay of ischemic stroke treatment if the patient presents within 4.5 h from symptoms onset [1]. Its use has faced a steady increase in the last 20 years, reaching almost 10% of all stroke admissions [2].
Extracranial internal carotid artery (ICA) stenosis accounts for approximately 10–20% of ischemic strokes. Current evidence strongly supports revascularization of 50–99% symptomatic stenoses in appropriately selected patients within 14 days of symptom onset, as this timing is critical to reduce the risk of stroke recurrence [3].
The extensive implementation of IVT has thus resulted in a progressive rise in the incidence of symptomatic ICA stenoses requiring subsequent intervention, thereby underscoring the critical need to evaluate the safety of revascularization in this specific setting and to define the optimal timing [4].
Revascularization should, in fact, be timed carefully: performing it too early may increase bleeding risks associated with IVT, such as intracranial hemorrhage (ICH) and surgical site bleeding. Conversely, delaying the procedure too long can raise the likelihood of recurrent stroke, which may be up to 5.5–22% in the first week in patients with symptomatic ICA stenosis [5,6,7,8,9].
The latest guidelines from the European Society for Vascular and Endovascular Surgery recommend postponing carotid revascularization for approximately six days following IVT, due to an increased risk of intracerebral hemorrhage and cervical hematoma. This carries a Class IIa recommendation with Level of Evidence B [3], primarily based on a meta-analysis by Kakkos et al. [5].
It is still uncertain whether patients with minimal or no cerebral ischemic involvement, who naturally present a lower risk of ICH [10], can safely undergo earlier revascularization following thrombolysis, thereby potentially decreasing the likelihood of recurrent stroke and shortening hospital stay [3].
The aim of this scoping review is to therefore systematically analyze the published results of carotid revascularization after thrombolysis to see if early revascularization after thrombolysis can be safely performed in patients with small or no brain lesions. Severity of stroke is used as a surrogate marker for the extension of the lesion in case a definite report on the dimension of the lesion cannot be identified [11,12]. The data produced will be used to assess if further studies on the topic are needed and if a multicenter dedicated randomized controlled trial could be run.
2. Materials and Methods
2.1. Study Design
To answer the relevant question, a scoping review protocol was drafted using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) [13], which was revised and reviewed by all components of the research team. The final protocol was registered prospectively with the Open Science Framework on 29 April 2025 (https://osf.io/m7b8n/overview). Appendix A provides the PRISMA-ScR Checklist of the present study (Table A1).
2.2. Research Question
The review question was as follows: “Can stroke patients with very small or no ischemic brain lesions be safely submitted to early (within 6 days) extracranial carotid revascularization after systemic thrombolysis?” The question was developed using the PICO (population, intervention, comparator, and outcomes) framework.
2.3. Relevant Studies Identification
The aim of this study was to identify publications describing the results of extracranial carotid revascularization (either carotid endarterectomy—CEA—or carotid artery stenting—CAS) after systemic thrombolysis, which also provided timing of treatment in relation to thrombolysis and extension of the ischemic lesion at imaging.
Data collection included type of publication, study population, outcome data (including perioperative stroke or death, ICH, and neck hematoma), timing of treatment after thrombolysis and brain lesions dimension. When provided, the severity of stroke at admission, evaluated either with the National Institute of Health Stroke Scale (NIHSS) or with the modified Rankin scale (mRs), was also included to act as a surrogate marker of the extension of the ischemic lesion [11,12]. All results were reported qualitatively and compared to the results of delayed revascularization (i.e., >6 days) obtained by previous metanalysis on the topic. Evaluation of methodological quality of the studies was not performed, as it is not required by the scoping review guidelines.
Only English peer-reviewed journal papers published between 2005 and 2025 were included. Type of publications were randomized controlled trials, non-randomized controlled trials, observational studies (prospective and retrospective cohort studies), case–control studies, case series, individual case reports, and descriptive cross-sectional studies, as well as qualitative studies, systematic reviews, and meta-analyses that met the inclusion criteria.
Expert opinions and letters to the editor covering the topic of the review were also screened to identify eventual relevant data.
Three online databases (EMBASE, PubMed, and Cochrane CENTRAL) were used. A dedicated search on Google Scholar was also performed to identify potential studies that may not have been included in the selected databases (such as congress abstracts, communications at meetings, other). Studies predominantly centered on the use of mechanical thrombectomy or the treatment of tandem lesions (i.e., intracranial and extracranial internal carotid artery) were excluded, as they would act as confounding factors. Studies reporting only on the results in patients with extracranial internal carotid artery occlusion were also excluded. Reference lists of the selected studies were screened for possible additional data.
The full electronic search strategy for the EMBASE database is provided in Appendix B. The search strategies for the other databases were derived from this one.
2.4. Studies Selection
A software based on artificial intelligence (Rayyan, Qatar Computing Research Institute, Doha, Qatar.) [14] was utilized to identify duplicates. Exclusion of duplicates was then manually confirmed (no automated exclusion). Two reviewers (G.C., L.F.M.) independently evaluated all articles by title and abstract. Full texts of the articles that met the inclusion criteria were obtained, and a second review was conducted to confirm inclusion based on the full text. Any disagreements were resolved through discussion and consultation with a third reviewer (M.D.P.).
2.5. Data Charting Process
A data extraction table on Microsoft Word (Microsoft Corp, Redmond, WA, USA) was specifically developed to collect the relevant data for this review. The extraction variables (columns) included the following: author and journal of publication (if any), country of origin, year of publication, methodology/methods, population and sample size, intervention type (CAS or CEA), number of patients treated within 6 days, dimension of brain lesions/no lesions, severity of stroke (NIHSS/mRS), and outcomes of treatment (death, ischemic stroke, symptomatic intracranial hemorrhage(sICH)/asymptomatic intracranial bleeding (aICB), neck hematoma/bleeding requiring reoperation). Finally, a comment column was incorporated to provide a concise narrative synthesis of the principal findings of each study, offering a more detailed examination of the reported complications and an assessment of the respective strengths and limitations of each manuscript. The data extraction table was collaboratively developed by two reviewers (G.C., L.F.M.) to specify the variables for extraction. Each reviewer independently performed data charting. The results of data charting were subsequently discussed for each included paper by both reviewers to refine the instrument through an iterative process of discussion and revision and to ensure consistency and homogeneity of the extracted data. The same procedure of discussion/revision was applied when compiling the comment column of the data extraction table. A specific analysis of the outcomes was conducted whenever patient-level data were available within the article.
2.6. Reporting the Results
Data were reported in textual format as counts (n) and percentages (%), as means with standard deviations (SD), or as medians with ranges or interquartile ranges (IQR), as appropriate. Missing values were denoted by a dash (–). Incidence rates for predefined outcomes, together with corresponding 95% confidence intervals (CI), were calculated when sufficient data were available. Likewise, odds ratios (OR) were computed for outcomes with adequate data. Statistical significance was assessed using Fisher’s exact test, with a two-sided significance level set at p < 0.05. The analyses were performed using R (v4.5.2) (R Foundation for Statistical Computing, Vienna, Austria).
The comment column of the data extraction table was employed to correlate, when feasible, complications—particularly ICH—with their timing in relation to IVT administration and the degree of neurological impairment of each patient.
3. Results
3.1. Search Results and Selection of the Studies
Through the selected databases (PubMed, EMBASE, and Cochrane CENTRAL), a total of 872 publications were found. Four additional abstracts were added through research on Google Scholar and one through citation searches. After removing duplicates (n = 446), a total of 426 publications were manually screened using titles and abstracts.
Based on titles and abstracts, 384 publications were further removed, and the full-text versions of additional 2 articles could not be retrieved, thus leaving 40 articles to be evaluated through full text.
Of the 40 articles assessed, 24 were excluded for the following reasons: absence of data on lesion extension and/or stroke severity at admission (n = 4); lack of information regarding treatment timing after IVT (n = 5); and failure to include patients treated within 6 days of IVT or inability to isolate outcomes for this subgroup, as results were reported only in aggregate for the entire study population (n = 10).
Systematic reviews that did not provide additional primary data (n = 2) and meta-analyses (n = 3) were also excluded from the analysis. However, their findings were incorporated as comparative references in the discussion section.
Of the five studies identified through alternative search methods, three were excluded due to the absence of precise information regarding the timing of treatment, and one was excluded for failing to report data on patients treated within six days.
Overall, 17 studies were included in the present scoping review.
The detailed PRISMA-ScR flow diagram of study selection is shown in Figure 1.
3.2. Study Characteristics
Table 1 provides an overview of the characteristics of the included studies.
The evidence consisted of one case report [15] and multiple retrospective analyses: 14 single-center cohort studies [8,16,17,18,19,20,21,22,23,24,25,26,27], one two-center cohort review [28], and two analyses based on national databases [29,30]. No randomized controlled trials addressing this topic were identified through the literature search. Furthermore, nine studies incorporated a control arm, which included either patients with symptomatic carotid stenosis undergoing carotid revascularization without intravenous thrombolysis (n = 8) [16,18,19,22,23,29,30,31] or patients treated exclusively with intravenous thrombolysis without subsequent carotid revascularization (n = 1) [21].
Except for the two studies based on national databases, all cohorts were derived from university or tertiary care hospitals. Geographically, ten studies were conducted within the European Region (Italy: n = 3; France: n = 2; UK: n = 2; Sweden: n = 1; Finland: n = 1; Czech Republic: n = 1), four studies originated from the USA, and three from East Asia (Japan: n = 2; Republic of Korea: n = 1).
Three studies [8,16,27] specifically included patients who had previously/simultaneously undergone intracranial catheter-based interventions for the presenting stroke. All other studies did not address this specific issue in their Methods section; therefore, it was assumed this subset of patients was not included.
Although treatment of tandem lesions was an exclusion criterion for the present review, two of these studies [8,27] were already incorporated in the most comprehensive meta-analysis on the subject by Kakkos et al. [5]. The third one [16] was added following consensus among the reviewers (G.C., L.F.M., M.D.P.), as it employed a propensity score-matched design comparing patients undergoing revascularization without IVT, and the rate of intracranial catheter-based interventions was relatively low (15/56, 26.7%). Moreover, this cohort displayed a contemporary approach to stroke management, supporting its relevance.
Patient-level data were available exclusively for small series.
3.3. Results
3.3.1. Severity of Stroke at Admission and Timing Between IVT and Carotid Revascularization
The results of the included studies are reported in Table 2.
A total of 1459 patients were included across 17 studies. Of these, 35 patients (2.4%) underwent CAS, while 1424 patients (97.6%) received CEA.
All the included studies reported results for patient treated within 2 weeks from IVT. Concerning the timing variable addressed in the scoping review—specifically, treatment within six days following intravenous thrombolysis (IVT)—data for 402 patients were identified. However, several studies reported timing in narrower intervals (seven studies < 24 h [15,17,18,19,20,27], two studies < 48 h [8,20], and four studies < 72 h [8,21,28,30]) rather than providing aggregated data for the <6-day timeframe.
With respect to the second component of the scoping review question—namely, the extent of the ischemic brain lesion—eight studies [17,18,19,20,21,24,25,26] reported this parameter as an exclusion criterion, meaning that carotid revascularization was performed exclusively in patients whose brain lesions were below this predefined size. Specifically, four studies [21,24,25,26] included patients with lesions involving less than one-third of the middle cerebral artery (MCA) territory, one study [20] applied an Alberta Stroke Program Early CT Score (ASPECTS) ≥ 8, and three studies [17,18,19] employed both criteria.
One study provided a brief qualitative description of the lesions [23], while another also reported the mean ischemic lesion volume for the entire cohort [24]. Only a single case report described treatment in a patient with an ischemic lesion exceeding one-third of the MCA territory [15].
Conversely, seven studies [8,16,22,27,28,29,30] did not provide any information regarding lesion size.
The severity of stroke at admission was instead well-reported in all studies. Three studies reported the median value of the modified Rankin scale (mRs) [16,28,29], while the other 14 used the National Institute of Health Stroke Scale (NIHSS) [15,17,18,19,20,21,22,23,24,25,26,27,30].
Notably, all studies reporting the mRS included a statistically significant higher proportion of patients with disabling stroke (mRS ≥ 3) in the IVT group compared to the control group (patients with no IVT), with prevalence ranging from 18.2% to 57% [16,28,29].
Studies reporting NIHSS scores predominantly included patients with moderate stroke (NIHSS 5–15). NIHSS values were presented either as median with range (Ijäs et al.: 6(0–20); Gunka et al.: 7 (3–18); Yong et al.: 15 (10–22)) [8,18,23] or as mean with standard deviation (overall mean: 10.2 ± 2.8) [17,21,22,23,25,26,27,31]. Patient-level NIHSS data were reported in nine studies [15,17,18,19,22,23,24,26,27]. Across these studies, individuals undergoing CAS generally exhibited higher baseline NIHSS scores, with an overall mean of 13.4 ± 1.5.
3.3.2. Ischemic Stroke at 30 Days
One study (Johal et al., 1055 patients) did not differentiate outcomes for ischemic versus hemorrhagic stroke, whereas the series by Vellimana et al. (11 patients) reported only the incidence of hemorrhagic stroke [22,29]. After excluding these two cohorts, the 30-day incidence of ischemic stroke was 10 events among 393 patients (2.5%; 95% confidence interval [CI], 1.2–4.6).
Among these ten events, one major stroke resulting in death occurred in a patient who underwent surgery within 24 h of intravenous thrombolysis (IVT) and presented with unstable neurological symptoms [18]. Additionally, one ischemic stroke was reported in a patient operated within 48 h [8], one retinal infarction in a patient treated at 3 days, and one minor stroke at 5 days post-IVT [30]. Four strokes occurred in patients operated after 48 h, although the exact timing was not clearly specified [8], and for two patients, the timing of postoperative stroke was not reported [16].
No detailed information regarding lesion extent or severity of stroke at admission was available for patients who experienced postoperative ischemic stroke.
3.3.3. Asymptomatic Intracranial Bleeding (aICB) Plus Symptomatic Intracranial Hemorrhage (sICH) at 30 Days
Johal et al. did not distinguish outcomes between ischemic and hemorrhagic stroke [29]. After excluding these cohort, the 30-day incidence of aICB plus sICH was 16 events among 397 patients (4.0%; 95% CI, 2.1–6.0). When restricting the analysis to symptomatic cases only, the incidence decreased to 10 of 397 patients (2.5%; 95% CI, 1.0–4.1), as 6 patients exhibited radiological findings without clinical symptoms. Notably, 13 of 16 events (81.2%) occurred within 48–72 h following IVT.
Regarding the type of revascularization, sICH occurred in three patients in the CAS group (3/35, 8.6%; 95% CI, 0–17.9) compared with seven patients in the CEA group (7/362, 1.9%; 95% CI, 0.5–3.4).
Patients undergoing CAS demonstrated significantly higher odds of developing sICH compared with those undergoing CEA (OR = 4.75; 95% CI, 1.17–19.28; p = 0.049).
The precise extent of brain lesions in patients with sICH or aICB could not be determined from the analyzed studies. Patient-level data on stroke severity were available for 10 individuals (9 with NIHSS scores and 1 with mRS), comprising three cases of aICB and seven cases of sICH, drawn from six studies [19,21,22,23,26,28]. Among patients with aICB, one-third (33.3%) presented with a modified Rankin Scale (mRS) score of 5 at admission, indicative of a disabling stroke, while the remaining two had mRS scores between 0 and 2. All patients with sICH exhibited moderate stroke severity according to NIHSS (range: 6–23), with 5 of 7 (71.4%) presenting with NIHSS scores greater than 10 at admission.
3.3.4. Overall Stroke (Ischemic and Hemorrhagic) at 30 Days
For the entire cohort included in the scoping review, the combined incidence of ischemic stroke and hemorrhagic complications was 45 out of 1459 cases (3.1%; 95% CI, 2.2–4.0). This composite outcome encompassed ischemic stroke, sICH, and aICB.
No detailed information regarding lesion extent or severity of stroke at admission was available for patients who experienced postoperative ischemic stroke.
3.3.5. Death at 30 Days
Similarly, excluding the subset of patients from Vellimana et al. [22], the rate of death at 30 days for the remaining studies was instead 17/1484 (1.1%; 95% CI, 0.6–1.7).
3.3.6. Wound Bleeding/Access Site Complications at 30 Days
No series including CAS patients reported access site complications (bleeding/pseudoaneurysm). Excluding the subset of patient from Vellimana et al., whose study only reported the outcome of sICH [22], the rate of wound bleeding/access site complication at 30 days was 55/1484 (3.7%; 95% CI, 2.7–4.7).
Only two studies specifically focused on patients requiring reoperation [8,30], whereas three studies also included cases of neck hematoma or wound complications that did not necessitate surgical reintervention [16,21,29]. The temporal distribution of wound complications was assessed exclusively by Johal et al., who reported a statistically significant increase in wound complication rates when CEA was performed within five days following IVT [29].
4. Discussion
Patients requiring extracranial carotid revascularization following IVT represent a small subset of the overall stroke population treated with IVT; however, their proportion has progressively increased over the past two decades, currently accounting for approximately 10% of all CEA for symptomatic patients [29].
Although the primary research question of this scoping review could not be definitively addressed due to limitations in the available evidence, several key observations emerged:
- Low risk of ischemic stroke and mortality after CEA: The incidence of postoperative ischemic stroke and death among patients undergoing CEA after IVT appears to be low.
- Higher complication risk with CAS, particularly sICH: Patients treated with CAS exhibit a higher risk of complications, notably sICH. However, this results should be interpreted with caution for several reasons. First, it is important to recognize that this cohort represents a distinct clinical subset, as CAS is frequently performed in the hyperacute phase (within hours) in patients with severe strokes and is often combined with intracranial thrombectomy for tandem lesions. These patients typically present with more severe neurological deficits and are exposed to the additional hemorrhagic risk of dual antiplatelet therapy [17,27], although the combination of IVT and dual antiplatelet therapy does not appear to be associated with an increased incidence of sICH, as suggested by recent findings from Cavalcante et al. [31]. Second, it must be emphasized that there is a marked numerical imbalance between the CEA (n = 1424) and CAS (n = 35) cohorts: this substantial volume disparity and inherent selection bias further limits any possible assumption.
- Wound complications after CEA: The reported incidence of wound-related complications following CEA after IVT is higher, largely influenced by the retrospective analysis by Johal et al. involving 1055 IVT patients [29]. Notably, this outcome encompassed bleeding and hematomas not necessarily requiring surgical reintervention, and the exact number of reoperations was not specified, leaving uncertainty regarding the clinical significance of these events.
- Limited data on infarct size as a selection criterion: The extent of cerebral infarction after IVT is rarely analyzed in the context of carotid revascularization and is primarily used as an exclusion criterion (typically, patients are considered for intervention if the infarct size is less than one-third of the middle cerebral artery territory and/or the ASPECT Score is ≥8). Although infarct size is a recognized risk factor for sICH [10], none of the patients who developed sICH had documented infarct dimensions in the reviewed studies. This limited characterization of the extent of brain lesions represents an intrinsic limitation of all available studies and substantially hampers the identification of potential risk factors that could aid in patient selection.
- Stroke severity as a determinant of complications: Stroke severity at admission was more consistently reported, and NIHSS scores were available for most patients who experienced sICH. In this subgroup, over 70% had NIHSS > 10, indicating moderate stroke severity; one patient had a modified Rankin Scale score of 5, reflecting a disabling stroke. Stroke severity is increasingly acknowledged as a major determinant of perioperative complications in the setting of carotid revascularization after stroke [4,32].
- Timing of revascularization and risk of sICH: Most postoperative sICH events occurred when revascularization was performed within 48–72 h of IVT, while the remaining occurred more than two weeks after IVT. No cases were observed between 4 and 6 days post-IVT in our analysis. The pooled sICH rate among patients undergoing CEA was 1.9%, comparable to rates reported in stroke patients undergoing CEA without prior IVT [10,33].
Symptomatic intracranial hemorrhage remains the most critical and feared complication following carotid revascularization in patients who have received IVT. The current body of evidence is inconclusive: while most studies report no increased risk of sICH after CEA in this setting [8,9,16,18,21,25,28,29,30], others (two studies, both coming from the same authors) suggest a higher incidence of intracranial bleeding [22,34]. A recent metanalysis on the association of IVT to acute stenting (and its required antiplatelet therapy) also underlines that the risk of sICH might be lower than previously feared in the specific setting of tandem lesions [31], thus further supporting a more proactive approach to carotid revascularization.
The Society for Vascular Surgery guidelines recommend delaying carotid revascularization for at least 48 h in clinically stable stroke patients (without previous IVT) to mitigate the risk of sICH and other neurological complications [35], as corroborated by the metanalysis of Hasan et al. [36]. Although not specifically targeted to the evaluation of IVT patients, this study further supports the higher risk of early (<48 h) revascularization of stroke patients also reported by our scoping review. More recently, two meta-analyses have proposed an even longer delay—approximately 6 to 7 days—before intervention for the subset of patients with previous IVT [5,37]. Although such postponement may reduce hemorrhagic risk, it must be weighed against the substantial risk of recurrent ischemic stroke, which can reach 8–22% within the first week [3].
This recommendation has been incorporated into the latest European Society for Vascular Surgery guidelines, which state the following: “For patients with acute ischemic stroke due to a symptomatic 50–99% carotid stenosis who have received IVT, delaying CEA or CAS by six days following completion of thrombolysis should be considered (Class IIa, Level of Evidence B).” However, these same guidelines acknowledge that postponing revascularization in patients without ischemic lesions at post-IVT brain imaging could be unnecessary [3].
The evidence underpinning this recommendation primarily derives from one of the aforementioned meta-analyses [5] and a single large retrospective study by Vellimana et al., based on the National Inpatient Sample (NIS) [34].
A critical appraisal of these sources is warranted before generalizing their conclusions to all IVT-treated patients, particularly given the rarity of sICH. Notably, both meta-analyses included asymptomatic intracranial hemorrhages in their outcome measures, as exemplified by the study by Deiana et al. [28], who reported three such events detected exclusively through routine postoperative imaging, which was systematically performed in all IVT patients regardless of neurological status. This approach may have led to underreporting of hemorrhages in the non-IVT group, where imaging was performed only in cases of neurological deterioration. An additional case of sICH reported by Fortin et al. [38] occurred in a patient with a large hemispheric infarction who underwent surgery 15 days after IVT. Given the prolonged interval, the causal relationship with IVT appears doubtful, although the event was counted in both metanalysis. Interestingly, Kakkos et al. [5] conducted a sensitivity analysis excluding studies with delayed (>7 days) or unreported intervention timing, and this yielded a nonsignificant odds ratio for intracranial bleeding for CEA after IVT versus CEA with no IVT (OR 1.66; 95% CI 0.17–16.43).
Furthermore, the dominant influence of the NIS-based study on pooled estimates introduces significant limitations. While its large sample size (551 IVT patients and 120,738 non-IVT patients) is a strength, the NIS is an administrative rather than a clinical database, whose possible inaccuracy in the setting of carotid revascularization has already been reported [39]. Moreover, the inclusion of transient ischemic attacks (without a defined percentage) in the control group compromises the reliability of comparative risk estimates.
Overall, the available studies on carotid revascularization following IVT consist exclusively of retrospective analyses derived from single-center or multicenter registries, resulting in substantial heterogeneity regarding outcome definitions, inclusion criteria, and timing of revascularization. The absence of prospective investigations and randomized controlled trials significantly limits the strength of the conclusions that can be drawn from the current evidence.
Findings from this scoping review are not conclusive and underscore the need for prospective studies to clarify optimal timing and patient selection for carotid revascularization after IVT, particularly regarding the characteristics of brain lesions. Multicenter registries are needed due to the low number of adverse events.
5. Conclusions
Further multicenter prospective registries addressing carotid revascularization after IVT are warranted to refine management strategies for this specific patient population, in order to avoid excessive delays. Future studies should clearly define outcome measures and complication criteria prior to enrollment, including the incidence of recurrent ischemic events during the waiting period for CEA or CAS, the role of medical treatment with single or dual antiplatelet therapy after IVT, and a thorough characterization of brain lesions at admission and after IVT, as these aspects have been poorly or not addressed in the available literature. Although a randomized controlled trial would be ethically acceptable and scientifically desirable, its feasibility appears limited given the low frequency of adverse events reported in the current literature.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Powers W.J. Rabinstein A.A. Ackerson T. Adeoye O.M. Bambakidis N.C. Becker K. Biller J. Brown M. Demaerschalk B.M. Hoh B. Guidelines for the Early Management of Patients with Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association Stroke 201950 e 344e 41810.1161/STR.000000000000021131662037 · doi ↗ · pubmed ↗
- 2Suolang D. Chen B.J. Wang N.-Y. Gottesman R.F. Faigle R. Temporal Trends in Stroke Thrombolysis in the US by Race and Ethnicity, 2009–2018 JAMA 20213261741174310.1001/jama.2021.1296634633406 PMC 8506301 · doi ↗ · pubmed ↗
- 3Naylor R. Rantner B. Ancetti S. de Borst G.J. De Carlo M. Halliday A. Kakkos S.K. Markus H.S. Mc Cabe D.J.H. Sillesen H. Editor’s Choice—European Society for Vascular Surgery (ESVS) 2023 Clinical Practice Guidelines on the Management of Atherosclerotic Carotid and Vertebral Artery Disease Eur. J. Vasc. Endovasc. Surg.202365711110.1016/j.ejvs.2022.04.01135598721 · doi ↗ · pubmed ↗
- 4Hayson A. Burton J. Allen J. Sternbergh W.C. Fort D. Bazan H.A. Impact of Presenting Stroke Severity and Thrombolysis on Outcomes Following Urgent Carotid Interventions J. Vasc. Surg.20237870271010.1016/j.jvs.2023.04.03137330150 · doi ↗ · pubmed ↗
- 5Kakkos S.K. Vega de Ceniga M. Naylor R. A Systematic Review and Meta-Analysis of Peri-Procedural Outcomes in Patients Undergoing Carotid Interventions Following Thrombolysis Eur. J. Vasc. Endovasc. Surg.20216234034910.1016/j.ejvs.2021.06.00334266765 · doi ↗ · pubmed ↗
- 6Nordanstig A. Gu T. Henze A. Wester P. Fox A.J. Johansson E. Risk of Stroke Recurrence After Intravenous Thrombolysis in Patients with Symptomatic Carotid Stenosis Can. J. Neurol. Sci.20245152152810.1017/cjn.2023.28437681233 · doi ↗ · pubmed ↗
- 7Johansson E. Cuadrado-Godia E. Hayden D. Bjellerup J. Ois A. Roquer J. Wester P. Kelly P.J. Recurrent Stroke in Symptomatic Carotid Stenosis Awaiting Revascularization: A Pooled Analysis Neurology 20168649850410.1212/WNL.000000000000235426747885 · doi ↗ · pubmed ↗
- 8Ijäs P. Aro E. Eriksson H. Vikatmaa P. Soinne L. Venermo M. Prior Intravenous Stroke Thrombolysis Does Not Increase Complications of Carotid Endarterectomy Stroke 2018491843184910.1161/STROKEAHA.118.02151729991655 · doi ↗ · pubmed ↗